REVISTA
PAULISTA
DE
PEDIATRIA
www.rpped.com.br
ORIGINAL
ARTICLE
Analysis
of
factors
associated
with
excess
weight
in
school
children
Renata
Paulino
Pinto
a,
Altacílio
Aparecido
Nunes
b,
Luane
Marques
de
Mello
b,∗aProgramadePós-Graduac¸ãoemSaúdenaComunidade,FaculdadedeMedicinadeRibeirãoPreto,UniversidadedeSãoPaulo
(FMRP/USP),RibeirãoPreto,SP,Brazil
bDepartamentodeMedicinaSocial,FaculdadedeMedicinadeRibeirãoPreto,UniversidadedeSãoPaulo(FMRP/USP),
RibeirãoPreto,SP,Brazil
Received1December2015;accepted24April2016 Availableonline26July2016
KEYWORDS Obesity; Overweight; Dietaryhabits; Healthbehavior; Schoolchildren
Abstract
Objective: To determine the prevalence of overweight and obesity inschoolchildren aged 10to16yearsanditsassociationwithdietaryandbehavioralfactors.
Methods: Cross-sectionalstudythatevaluated505adolescentsusingastructuredquestionnaire andanthropometricdata.ThedatawasanalyzedthroughtheTTestforindependentsamples andMann---WhitneyTesttocomparemeansandmedians,respectively,andChi2Testfor propor-tions.Prevalenceratio(RP)andthe95%confidenceintervalwasusedtoestimatethedegree ofassociationbetweenvariables.Thelogisticregressionwasemployedtoadjusttheestimates toconfoundingfactors.Thesignificancelevelof5%wasconsideredforallanalysis.
Results: Excessweightwasobservedin30.9%oftheschoolchildren:18.2%ofoverweightand 12.7%ofobesity.Therewasnoassociationbetweenweightalterationsanddietary/behavioral habitsinthebivariateandmultivariateanalyses.However,associationswereobservedin rela-tion togender.Dailyconsumption ofsweets[PR=0.75(0.64---0.88)]andsoftdrinks [PR=0.82 (0.70---0.97)]waslessfrequentamongboys;havinglunchdailywasslightlymoreoftenreported byboys[OR=1.11(1.02---1.22)].Physicalactivitypracticeof(≥3times/week)wasmoreoften mentionedbyboysandtheassociationmeasuresdisclosedtwo-foldmorephysicalactivityin thisgroup[PR=2.04(1.56---2.67)]whencomparedtogirls.Approximately30%ofboysand40% ofgirlsstatedtheydidnotperformactivitiesrequiringenergyexpenditureduringfreeperiods, withboysbeing32%lessidlethangirls[PR=0.68(0.60---0.76)].
Conclusions: A high prevalence of both overweight and obesity was observed, as well as unhealthy habits inthestudy population, regardless ofthepresence ofweight alterations. Healthpromotion strategiesin schoolsshould be encouraged,inorder to promotehealthy habitsandbehaviorsamongallstudents.
©2016SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
∗Correspondingauthor.
E-mails:[email protected],[email protected](L.M.Mello). http://dx.doi.org/10.1016/j.rppede.2016.04.005
PALAVRAS-CHAVE Obesidade;
Sobrepeso;
Hábitosalimentares; Comportamento desaúde; Escolares
Análisedosfatoresassociadosaoexcessodepesoemescolares
Resumo
Objetivo: Determinaraprevalênciadesobrepesoeobesidadeemescolaresentre10e16anos esuaassociac¸ãocomfatoresalimentaresecomportamentais.
Métodos: Esteéumestudotransversal,queavaliou505escolaresatravésdequestionário estru-turado edadosde antropometria.ParaaanálisedosdadosforamutilizadosoTesteT para amostrasindependenteseoTestedeMann-Whitneyparacomparac¸ãodemédiasemedianas, respectivamente,eoTestedoChi2paraproporc¸ões.ARazãodePrevalência(RP)eseus respec-tivosintervalosdeconfianc¸aa95%foiempregadocomoestimadordeassociac¸ãoeregressão logísticamúltiplaparaajustamentoporfatoresdeconfusão.Emtodasasanálises,considerou-se umníveldesignificânciade5%.
Resultados: Observou-seexcessodepesoem30,9%dosescolares:18,2%desobrepesoe12,7% de obesidade. Nãoseobservou associac¸ão entreasalterac¸ões de pesoe hábitos alimenta-res/comportamentaisnasanálisesbivariadasemultivariadas.Entretanto,foramencontradas associac¸õesquantoaosexo.Consumirdoces[RP=0,75(0,64-0,88)]erefrigerantesdiariamente [RP=0,82(0,70-0,97)]foramhábitosrelatadospor273(54,1%)crianc¸as,menosfrequentemente pelosmeninos.Almoc¸ardiariamentefoihábitodiscretamentemaisobservadoentreos meni-nos[RP1,11(1,02-1,22)].Praticaratividadefísica(≥3vezes/semana)foimaisreferidopelos meninoseasmedidasdeassociac¸ãorevelaramduasvezesmaisatividadefísicanessegrupo [RP=2,04(1,56-2,67)],quandocomparadocomodasmeninas.Cercade30%dosmeninose40% dasmeninasdisseramnãorealizaratividadescomgastodeenergianosperíodoslivres,sendo osmeninos32%menosociososdoqueasmeninas[RP=0,68(0,60-0,76)].
Conclusões: Observou-sealtaprevalênciatantodesobrepesoeobesidadequantodehábitos pouco saudáveis napopulac¸ão estudada,independentemente dapresenc¸ade alterac¸õesdo peso.Estratégiasdepromoc¸ãodasaúdenasescolasdevemserestimuladas,nosentidodese incentivarhábitosecomportamentossaudáveisentretodososestudantes.
©2016SociedadedePediatriadeS˜aoPaulo. PublicadoporElsevier EditoraLtda.Este ´eum artigoOpenAccesssobumalicenc¸aCCBY(http://creativecommons.org/licenses/by/4.0/).
Introduction
Obesityisachronicdiseasecharacterizedbyexcessbodyfat withconsequenthealth damage.1The WorldHealth Orga-nization (WHO) considers obesitya public health problem associatedwithhighmorbidityandmortalityrates.1 Accord-ing to the Brazilian Association for the Study of Obesity and Metabolic Syndrome (ABESO), exogenousobesity rep-resentsapproximately95%ofcases2and,similarlytowhat occursinadults,childhoodobesity isalsoaccompaniedby comorbiditiessuchassystemicarterialhypertension(SAH), glucose intolerance, orthopedic problems and cholesterol metabolismalterations,amongothers.2Geneticfactorsand apositivebalancebetweencaloricintakeandenergy expen-ditureare some of the etiological factorsinvolved in the pathogenesis of obesity.2 Among the exogenous factors, overfeeding in the early years of life seems to influence thenumberofadipocytes,probablyexplainingwhy50%---65% ofobeseadultswereobesechildren.3Adolescenceis con-sidered by some authors oneof the most critical periods ofhuman development,during whichtypicalphysiological changesseem,amongotherthings,toincreasetheriskof obesitydevelopmentanditsfuturepersistence.4
However,obesityis knowntohave amultifactorial eti-ology, where environmental and behavioral factors seem to influence its onset, most likely justifying the variable prevalence observed between different regions. The low-estprevalenceratesofobesityinchildrenandadolescents
areobserved in Asia (2.9%) and Africa (3.9%),5,6 whereas thehighestonesarefoundintheUnitedStates(31.8%).7In LatinAmerica,theprevalenceofobesity amongpreschool childrenis 6.2%inCosta Rica, 6.5%inBolivia, 7%in Chile and7.3%in Argentina.8Brazilian Studies intheNorthand Northeastregionsshowthatoverweightandobesityaffect 25%---30%ofchildrenbetweenfiveandnineyears,whereas intheSoutheastandMidwestregionsthispercentageranges from32%to40%.9AnotherstudyinRioGrandedoSuland SantaCatarinafound aprevalenceof 14.4%ofoverweight and7.5%ofobesityinpreschoolchildren.10
AlthoughthestateofSãoPaulohasthehighestpopulation concentrationanditiswheremanystudiesonthissubject aredeveloped,thefewstudiesintheliteratureinvolvingthe populationofschoolchildreninpreadolescenceand adoles-cencedatebacktomorethan10yearsandhaveprevalence ratesthatvaryconsiderably.11---14Additionally,dataon obe-sity/overweight in healthy children who do not undergo medicaltreatment or supervision and have overweight as theonlyfactortobeinvestigated,arealsoscarce.
establishitsassociationwithsomecommonaspectsofthis population’sroutinelife.
Method
This is a cross-sectional study, carried out in Elementary Schools in the city of Ribeirão Preto, state of São Paulo, Brazil, involving students aged 10---16 years. The study wasapprovedbyRibeirãoPretoSchoolBoard(Registration 879/073/2012) and approved by the Institutional Review BoardofHospitaldasClínicasdaFaculdadedeMedicinade RibeirãoPreto(FMRP-USP).
AccordingtodatafromthestateEducationSecretariat, 16,785childrenandadolescentswereenrolledin 2013,in 66 schools of the Ribeirão Preto School Board. To obtain a representative sample of the studied population, two schoolswereselectedfromeachcity district,withatotal of11schoolsparticipatinginthestudy.
To calculate sample size, we considered a prevalence rateof 40%ofoverweightandobesityamongchildrenand adolescents,admittingamaximumsamplingerrorof5%and a95%confidencelevel,accordingtotheformula(finite pop-ulation):
n= Z2(1−y)/2Np(1−p) d2(N−1)+Z2(1−y)/2p(1−p)
Therefore,aminimumsamplesizeof361 studentswas estimated.Anticipatinglossesandaimingtomaintainregion representativeness,thetotalnumberconsistedof505 stu-dents. Only students enrolled in the public elementary schools of Ribeirão Preto school network, who agreed to participateandwhoseparentsorguardiansauthorizedtheir participation were considered eligible. Pregnant students wereexcluded, aswell as adolescentswith diseases that couldinterferewithbodycomposition.
Datawere collected throughfieldresearch, withvisits beingscheduledtoselectedschoolsandinterviewswith stu-dentscarriedoutovertheyears2013and2014.Duringthe firstvisit,fivestudentsfromeachschoolyear/gradewere randomlyselectedandatthattime,theyreceived informa-tionabout theresearch andthe procedurestobecarried outatthefollowingvisits.Thetermsofassentandconsent weregiventoeachselectedchildtobetakentotheparents. Theinterviewsandanthropometricmeasurements(weight, height,waist,hip)wereperformedaftertheparentsorlegal guardiansgavetheirpermission.
Body mass was measured using a Plenna standard portabledigitalscale(Plenna®,SãoPaulo,SP,Brazil), cer-tifiedby INMETROandthat haditsown certification(two weighings), with an error margin of±100g. For the mea-surementsofwaistandhipcircumference,a2-meterSanny anthropometric measuring tape (Sanny®, São Paulo, SP, Brazil) was used. Height was measured using a portable, retractableWISO210cmcompactstadiometer(WISO®,Sao Jose,SC, Brazil), withafrontal displayandmeasurement screenwithresolutioninmillimeters(1mm)andnumbered ateverycentimeter.Forbetterhandlingandtransportofthe device,astainlesssteelplatformwasproducedonwhichthe stadiometerwassettoallowthetransportandmeasurement inastandingandverticalposition.
Body Mass Index (BMI) was used to characterize over-weight and obesity, calculated according to the WHO recommendations.1Theparametersusedforthediagnoses wereZ-scoresofBMI/age,forwhichpercentiles>85and≤97 representoverweight;>97and≤99.9representobesityand percentiles>99.9 correspondtosevereobesity,considering referencevaluesforchildrenandadolescentsaged5toup to20yearsofage.
Dataregardingthepracticeofphysicalactivity,dietand lifestylewereobtainedthroughastructuredquestionnaire consisting of closed questions, where students answered abouttheirdietaryhabits(waterintake,havingbreakfast, lunch,snacksbetweenmealsanddinnerdaily;eatingsweets and drinking soft drinks) and behavioral habits, such as screentime,includingtelevision,computerandvideogame use,andthetypeofactivitiestheyperformedintheirfree time.
The collected data were stored in Excel spreadsheets 2010®(California,USA)andtheentriesweremadeand ver-ified by twopeople. Data were analyzed using the STATA software, version 13.0 (Texas, USA) and MedCalc®, ver-sion13.2.2.1(Ostend,Belgium).Thedescriptiveanalysesof dataareshownintables,containingabsoluteandrelative frequencies (categorical data).As most quantitative data showedan asymmetricdistributionin thenormalitytests, itwasdecidedtoshowthemasmediansandtheir respec-tiveinterquartile(IQ)intervals.Onlythevariablesageand heightareshownasmeanandstandarddeviation.
Whenanalyzingthecontinuousvariables,Student’st-test wasusedfor independentsamplesandtheMann---Whitney test for comparison of means and medians, respectively. The chi-square test was used to compare the propor-tionsbetweengroups.Whenanalyzingthecategoricaldata, prevalence ratio(PR)and theirrespective95% confidence intervals wereusedtoestimatethe degree ofassociation betweenvariables.Themultiplelogisticregressionmethod wasemployedtoadjusttheestimatesforconfounding fac-tors.Asignificancelevelof5%wasconsideredinallanalyses.
Results
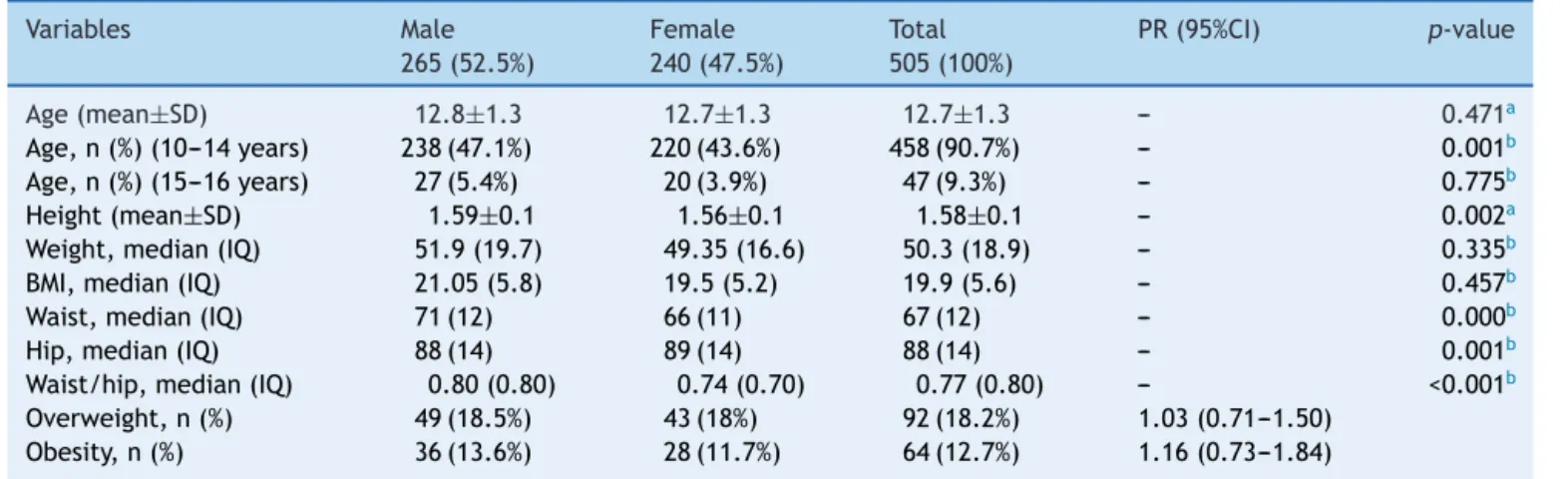
Ofthe505studiedchildren,265(53%)weremalesand91% belongedtotheagegroupof10---14years.Themeanageof thestudypopulationwas12.7±1.3years(12.8±1.3forboys and12.7±1.3forgirls),withnodifferencebetweenthe gen-ders(p>0.05).Theobservedmeanheightwas1.58±0.09m, significantly higher in boys (mean of 1.59±0.11 boys and 1.56±0.07 in girls; p<0.05). The median waist, hip and waist/hip ratio werealso significantlyhigher amongmale students (p>0.05). Fortheother variables, therewereno differencesbetweenthegenders(Table1).
Table1 Profileofthestudypopulationaccordingtogender.
Variables Male
265(52.5%)
Female 240(47.5%)
Total 505(100%)
PR(95%CI) p-value
Age(mean±SD) 12.8±1.3 12.7±1.3 12.7±1.3 --- 0.471a
Age,n(%)(10---14years) 238(47.1%) 220(43.6%) 458(90.7%) --- 0.001b
Age,n(%)(15---16years) 27(5.4%) 20(3.9%) 47(9.3%) --- 0.775b
Height(mean±SD) 1.59±0.1 1.56±0.1 1.58±0.1 --- 0.002a
Weight,median(IQ) 51.9(19.7) 49.35(16.6) 50.3(18.9) --- 0.335b
BMI,median(IQ) 21.05(5.8) 19.5(5.2) 19.9(5.6) --- 0.457b
Waist,median(IQ) 71(12) 66(11) 67(12) --- 0.000b
Hip,median(IQ) 88(14) 89(14) 88(14) --- 0.001b
Waist/hip,median(IQ) 0.80(0.80) 0.74(0.70) 0.77(0.80) --- <0.001b
Overweight,n(%) 49(18.5%) 43(18%) 92(18.2%) 1.03(0.71---1.50) Obesity,n(%) 36(13.6%) 28(11.7%) 64(12.7%) 1.16(0.73---1.84)
IQ,interquartileinterval;waist/hip,waist-to-hipratio.
a ttestforindependentsamples. b Mann---Whitneytest.
in64(12.7%)students,ofwhich56.3%wereboys[PR=1.16 (0.73---1.84)].
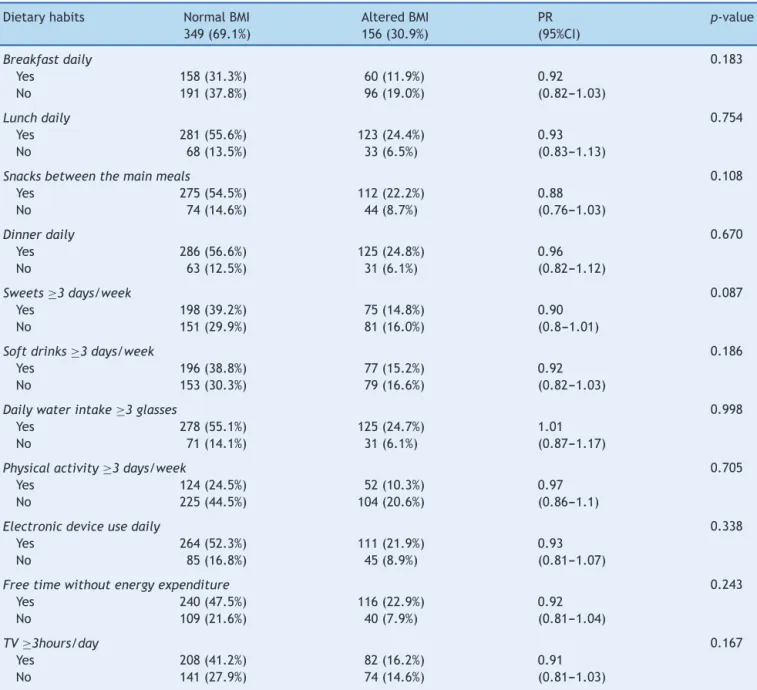
Whenanalyzingthedietaryhabitsanddailyactivitiesof theschoolchildren, consideringthe presenceof BMI alter-ations, it was observed that approximately 50% of the children with BMI alteration, i.e., obesity or overweight, admittedconsumingsweetsand/orsoftdrinksdaily,while dailywaterintakeandthehabitofhavingbreakfast,lunch, snacksbetweenmealsanddinnerdailywasmorefrequently reportedbystudentswithnormalBMI(Table2).Itwasalso observedthatmanystudentsdidnotperformregular physi-calactivity.Ofthe156studentswithalteredBMI,104(66%) admittednotperforminganyfrequentphysicalactivity,116 (74%)reportedspendingmany oftheirfreehoursin activ-itieswithout energyexpenditureand82(53%)watchedTV formorethanthreehoursaday.
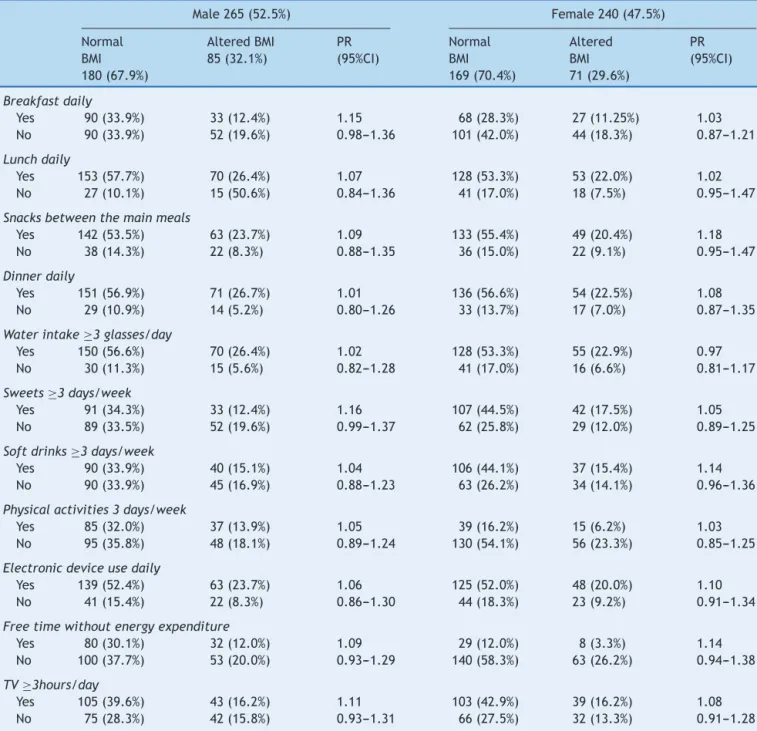
When evaluating the same variables considering the gender, it was observed that 273 (54.1%) students said they consumed sweets and soft drinks daily, a habit sig-nificantlymorefrequent amonggirls[PR=0.75 (0.64---0.88) andPR=0.82 (from0.70 to0.97),respectively]. The habit of having lunch daily was more often reported by boys [OR=1.11 (1.02---1.22)]. As for the daily water intake and havingbreakfast,lunch,snacksbetweenmealsanddinner daily,wereequallyreportedbystudentsfrombothgroups (Table3).
Only 35% of the study population reported practicing sometypeofregular physicalactivity.Whenassessing the positive responses to this item, the practice of physical activitywasmostoftenreportedbythegroupofmale stu-dents (24% of boys versus 11% of girls). The analysis of the association between this variable andgender showed that boyswere two-fold more physically activethan girls [PR=2.04(1.56---2.67)].Asforthevariablefreehours with-outenergyexpenditure,approximately30%ofboysand40% ofgirlssaidtheyperformednoactivitieswithenergy expen-diture in their free time, with the girls being 32% more inactivethan boys[PR=0.68 (0.60---0.76)].It wasobserved that boys use more electronic devices (40%) when com-paredtogirls(34%),buttherewasnosignificantdifference between the genders [PR=1.06 (0.95---1.17)]. Watching TV
daily was a very frequent habit. Approximately 60% of all assessed students admitted spending more than three hoursaday watchingTV, withnodifferencebetweenthe groups [PR=1.06 (0.95---1.17)], suggesting it is a common behavior to the entire assessed population, regardless of gender.
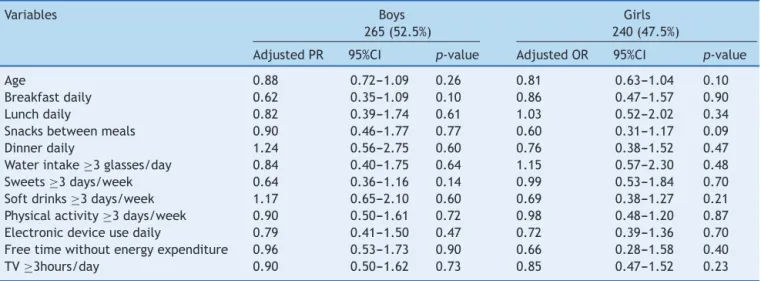
Amultiplelogisticregressionanalysiswascarriedoutto assesstheinfluence of lifestylefactorsanddietary habits onthelikelihoodofBMIalterations.Theresultofthe analy-sisshowedthatthevariablesincludedinthemodeldidnot changethelikelihoodofBMIalteration.Thesubgroup analy-sisconsideringgenderalsoshowednoinfluenceoffoodand behavioralvariablesonBMIalterations,inmaleorfemale students(Table4).
Although significant associations between dietary/behavioral variables and BMI alterations were not observed (Tables 2 and 4), the occurrence of some unhealthyhabitsandbehaviorswasconfirmed,whichwere frequent in thestudied population, apparently related to theroutinelifeofboysandgirlsatthisagegroup(Table4).
Discussion
Theresultsofthisstudyshowedahighprevalenceof over-weightandobesityinelementarystudentsfrompublicstate schools of Ribeirão Preto (SP), providing information on this topic among the population of schoolchildren from the Northwest Region of the state of São Paulo. These data confirm the findings of other studies carried out in otherregions16---18,23,24andalsodisclosedthepresenceofan unhealthylifestyle,suchaspreferenceforfoodswithhigher calorieandlowernutritionalcontent,screentime(TVand computers)abovethatrecommendedbytheWHOandlittle physicalactivity.
Table2 Profileofthestudypopulationregardingdietaryandbehavioralhabits,accordingtoBMI.
Dietaryhabits NormalBMI 349(69.1%)
AlteredBMI 156(30.9%)
PR (95%CI)
p-value
Breakfastdaily 0.183
Yes 158(31.3%) 60(11.9%) 0.92
No 191(37.8%) 96(19.0%) (0.82---1.03)
Lunchdaily 0.754
Yes 281(55.6%) 123(24.4%) 0.93
No 68(13.5%) 33(6.5%) (0.83---1.13)
Snacksbetweenthemainmeals 0.108
Yes 275(54.5%) 112(22.2%) 0.88
No 74(14.6%) 44(8.7%) (0.76---1.03)
Dinnerdaily 0.670
Yes 286(56.6%) 125(24.8%) 0.96
No 63(12.5%) 31(6.1%) (0.82---1.12)
Sweets≥3days/week 0.087
Yes 198(39.2%) 75(14.8%) 0.90
No 151(29.9%) 81(16.0%) (0.8---1.01)
Softdrinks≥3days/week 0.186
Yes 196(38.8%) 77(15.2%) 0.92
No 153(30.3%) 79(16.6%) (0.82---1.03)
Dailywaterintake≥3glasses 0.998
Yes 278(55.1%) 125(24.7%) 1.01
No 71(14.1%) 31(6.1%) (0.87---1.17)
Physicalactivity≥3days/week 0.705
Yes 124(24.5%) 52(10.3%) 0.97
No 225(44.5%) 104(20.6%) (0.86---1.1)
Electronicdeviceusedaily 0.338
Yes 264(52.3%) 111(21.9%) 0.93
No 85(16.8%) 45(8.9%) (0.81---1.07)
Freetimewithoutenergyexpenditure 0.243
Yes 240(47.5%) 116(22.9%) 0.92
No 109(21.6%) 40(7.9%) (0.81---1.04)
TV≥3hours/day 0.167
Yes 208(41.2%) 82(16.2%) 0.91
No 141(27.9%) 74(14.6%) (0.81---1.03)
Thesedata, whenevaluatedtogether,show thatbetween 1970 and2009 in Brazil, theprevalence excess weightin childrenandadolescentsincreasedfour-tofive-fold.16,17
Corroborating the data from official documents on the subject, epidemiological studies carried out in dif-ferent regions of Brazil showed a high prevalence of obesity/overweightintheschoolchildrenpopulation,some withvaluesabovethe national average found by theHBS 2008/2009.Dinizetal.,in2006,studied4210studentsfrom public schools in Pernambuco and found a prevalence of overweightof11.5%and2.4%ofobesity.18
In another study, published in 2008, the same authors observed overweight in 29.1% of boys and 32.6% of girls19 of 694 assessedschoolchildren aged between eight and 11 years, in a municipality in the state of Rio GrandedoSul,prevalencesimilartothatobservedinthis study.
Ramos et al. also found high prevalence rates. The authorsstudied941childrenfrompublic(stateand munic-ipal) and private schools, aged 10---14 years, in the city of Campo Grande(MS) and found that 23.1% of the chil-drenwereoverweight.20Souza,whenstudying1187students from public elementary schools in Divinópolis (MG) aged 6---14 years,found 24.4% of the children withobesity and overweight,with23.5%ingirlsand22.6%inboys.21Cabrera etal.,alsoin2014,observedevenhigherprevalencerates. Whenassessing170childrenand232adolescentsfrom pub-lic schools inthe municipalityof Nantes(SP),the authors observedweightabovetheadequatefortheagein30.59% oftheassessedstudents,22aprevalencerateclosetothat observedinthepresentstudy.
Table3 DistributionoffoodandbehavioralvariablesaccordingtoBMIalterationbygender.
Male265(52.5%) Female240(47.5%)
Normal BMI 180(67.9%)
AlteredBMI 85(32.1%)
PR (95%CI)
Normal BMI 169(70.4%)
Altered BMI 71(29.6%)
PR (95%CI)
Breakfastdaily
Yes 90(33.9%) 33(12.4%) 1.15 68(28.3%) 27(11.25%) 1.03 No 90(33.9%) 52(19.6%) 0.98---1.36 101(42.0%) 44(18.3%) 0.87---1.21
Lunchdaily
Yes 153(57.7%) 70(26.4%) 1.07 128(53.3%) 53(22.0%) 1.02 No 27(10.1%) 15(50.6%) 0.84---1.36 41(17.0%) 18(7.5%) 0.95---1.47
Snacksbetweenthemainmeals
Yes 142(53.5%) 63(23.7%) 1.09 133(55.4%) 49(20.4%) 1.18 No 38(14.3%) 22(8.3%) 0.88---1.35 36(15.0%) 22(9.1%) 0.95---1.47
Dinnerdaily
Yes 151(56.9%) 71(26.7%) 1.01 136(56.6%) 54(22.5%) 1.08 No 29(10.9%) 14(5.2%) 0.80---1.26 33(13.7%) 17(7.0%) 0.87---1.35
Waterintake≥3glasses/day
Yes 150(56.6%) 70(26.4%) 1.02 128(53.3%) 55(22.9%) 0.97 No 30(11.3%) 15(5.6%) 0.82---1.28 41(17.0%) 16(6.6%) 0.81---1.17
Sweets≥3days/week
Yes 91(34.3%) 33(12.4%) 1.16 107(44.5%) 42(17.5%) 1.05 No 89(33.5%) 52(19.6%) 0.99---1.37 62(25.8%) 29(12.0%) 0.89---1.25
Softdrinks≥3days/week
Yes 90(33.9%) 40(15.1%) 1.04 106(44.1%) 37(15.4%) 1.14 No 90(33.9%) 45(16.9%) 0.88---1.23 63(26.2%) 34(14.1%) 0.96---1.36
Physicalactivities3days/week
Yes 85(32.0%) 37(13.9%) 1.05 39(16.2%) 15(6.2%) 1.03 No 95(35.8%) 48(18.1%) 0.89---1.24 130(54.1%) 56(23.3%) 0.85---1.25
Electronicdeviceusedaily
Yes 139(52.4%) 63(23.7%) 1.06 125(52.0%) 48(20.0%) 1.10 No 41(15.4%) 22(8.3%) 0.86---1.30 44(18.3%) 23(9.2%) 0.91---1.34
Freetimewithoutenergyexpenditure
Yes 80(30.1%) 32(12.0%) 1.09 29(12.0%) 8(3.3%) 1.14 No 100(37.7%) 53(20.0%) 0.93---1.29 140(58.3%) 63(26.2%) 0.94---1.38
TV≥3hours/day
Yes 105(39.6%) 43(16.2%) 1.11 103(42.9%) 39(16.2%) 1.08 No 75(28.3%) 42(15.8%) 0.93---1.31 66(27.5%) 32(13.3%) 0.91---1.28
characteristics related to regional/cultural, genetic and behavioralfactors.Additionally,methodologicalissues,such asstudydesign,differentformsofdatacollectionand dif-ferent parameters used for classification of obesity and overweight may also explain the variability in the study results.However,itisnoteworthythehighratesofobesity andoverweightobserved inthepresent study andseveral others.
Excessweightisachronicconditionthatactsasarisk fac-torfor otherchronicdiseases,which,byoccurringatsuch anearlystageoflife,canpredisposeveryyoungindividuals topreventablediseasesandcomplications.Type2diabetes mellitus,systemicarterialhypertension,dyslipidemia, gas-troesophagealrefluxdisease,osteoarthritis,orthopedicand posturalproblems,certaintypesofcancersinlaterphases
of life, social adjustment problems and depression are someofthediseasesassociatedwithchildhoodobesity.24,25 A British cohort study, carried out in late 1990, showed thatbeingoverweightduringchildhoodresulted ina two-fold increase in the risk of death from ischemic heart diseasein adulthood.26 Obesityis alsorelatedto obstruc-tivesleepapnea-hypopneasyndrome,asthmaandexercise intolerance.25
Table4 MultivariateanalysisofthevariablesBMIalterationandbehavioralanddietaryhabitsconsideringgender.
Variables Boys
265(52.5%)
Girls 240(47.5%)
AdjustedPR 95%CI p-value AdjustedOR 95%CI p-value
Age 0.88 0.72---1.09 0.26 0.81 0.63---1.04 0.10
Breakfastdaily 0.62 0.35---1.09 0.10 0.86 0.47---1.57 0.90 Lunchdaily 0.82 0.39---1.74 0.61 1.03 0.52---2.02 0.34 Snacksbetweenmeals 0.90 0.46---1.77 0.77 0.60 0.31---1.17 0.09 Dinnerdaily 1.24 0.56---2.75 0.60 0.76 0.38---1.52 0.47 Waterintake≥3glasses/day 0.84 0.40---1.75 0.64 1.15 0.57---2.30 0.48 Sweets≥3days/week 0.64 0.36---1.16 0.14 0.99 0.53---1.84 0.70 Softdrinks≥3days/week 1.17 0.65---2.10 0.60 0.69 0.38---1.27 0.21 Physicalactivity≥3days/week 0.90 0.50---1.61 0.72 0.98 0.48---1.20 0.87 Electronicdeviceusedaily 0.79 0.41---1.50 0.47 0.72 0.39---1.36 0.70 Freetimewithoutenergyexpenditure 0.96 0.53---1.73 0.90 0.66 0.28---1.58 0.40 TV≥3hours/day 0.90 0.50---1.62 0.73 0.85 0.47---1.52 0.23
largeproportionofthestudypopulation,regardlessofthe weight.
The high consumption of sweets and soft drinks, low waterintakeand littlephysical activity werereportedby moststudents.Additionally, mostof theassessedchildren reportedspendinglongperiodsoftimewatchingTVorusing the computer(screen time),showing that these arevery widespread habits and behaviors in children, not specifi-callyrestrictedtochildrenwithalteredBMI.Theresultsof a study carried out to evaluate the influence of environ-mentalfactorsonthelackofphysicalactivityshowedthat North-Americanchildrenaged8---18yearsspendanaverage of7.5hours/dayinmobilephones,electronicgames, com-putersandtelevision,whichreducestheavailabletimeand motivationto participatein physical activities andactive games.27 But the lack of physical activity seems to have broader implications. Another recent study showed that sedentary children have reduced physical fitness, with a negativeimpact on flexibility, strength of several muscle groupsandmuscleexplosion,whichareevenworseinobese and overweight children.28 Therefore, as physical fitness decreases,exerciseintoleranceincreases,further promot-ingphysicalinactivity.
However,theassessmentofdietaryandbehavioral varia-bles in the bivariate analyses showed that the use of electronicgames is the preferredactivity for boys, while girlsreportedahigherdailyconsumptionofsweetsandsoft drinks,aswellasmoretimespentwithTVandother activi-tieswithnoenergyexpenditure,suggestinggender-related preferences.
Severalstudieshaveconfirmedtheincreasedprevalence of overweight and obesity in schoolchildren of differ-ent age groups, regardless of gender. The causes of this increase are not well known, but, as mentioned before, unhealthydietaryhabitsand lifestyle,aswell asgenetic, metabolic and environmental factors are involved.24,25,27 Approximately 90% of obesity cases are considered idio-pathic and 10% are attributed to hormonal and genetic causes.Thelatestadvancesinresearchindicatethe partic-ipationofleptin,thehypothalamicmelanocortinreceptor4
andmitochondrialuncouplingproteinsinthepathogenesis ofobesity/overweight,whichopensnewpossibilitiesforthe successfultherapeutic management of theseconditions,29 especially in cases of severe obesity and when measures aimedatchanginghabitsandlifestylewerenotsuccessful. Althoughtheassociationbetweenoverweightandintake of foods with high sugar and fat content and insuffi-cient physicalactivity iswell known,23---25,27,28thiswasnot observed in this study, probably because they represent widespread practice among the assessed schoolchildren, regardless of body weight. Moreover, the present study showedtheassociationbetween somedietaryhabits (eat-ing sweets and soft drinks ≥3 times/week, having lunch daily)andsomebehaviorsofdailyliving(physicalactivity≥3 times/week,free hourswithout energyexpenditure)with gender, which could indicate the need for differentiated preventiveinterventionsforboysandgirls.
Childhoodobesityisahealth problemthathasaroused increasinginterestamongpublicadministrators.Amongthe goals of the Strategic Action Plan for Confronting Non-communicableChronicDiseases(NCDs)inBrazilfrom2011 to2022isthereductioninchildhoodobesity rates.30 Food surveillance, regulation and quality control of food and stimulatingphysical activityandincreasedconsumption of healthy foods (fruits and vegetables) are initiatives that, aboveall,ensurebetterhealthforallchildrenand adoles-centsandpromotethedevelopmentofnew,moreadequate habits.
habitsthat wouldcauseembarrassment, asmentionedby otherauthors.10
Inconclusion,wefoundahighprevalenceofoverweight andobesityamongschoolchildrenaged10and16years,who attendedpublicstateschoolsinthecityofRibeirãoPreto. Althoughtheassociationwithoverweightwasnotfound,the weekly timespent withelectronic games andTV, aswell asthefree timedevotedtoactivities thatdonot involve energyexpendituresuggestsaninadequatelifestyleforthis agegroup.As aresult,lowlevelsofphysicalactivitywere identified for the overall assessed population. The same occurredwithfactorsrelatedtodietaryhabits.Theresults disclosedthe frequent intakeof littlenutritious food and highintakeoffoodswithlittlenutritionalvalue(sweetsand softdrinks).Althoughthesefindingsshowednoassociation withobesityoroverweight,itisnoteworthythe dissemina-tionoftheseunhealthyhabitsearlyinlife.Additionally,for theschoolchildrenwithobesityandoverweight,healthcare andguidelinesforthe preventionoffuturediseaseshould be started as soon as possible, respecting the individual differencesandpreferences.
Funding
Fundac¸ão de Apoio ao Ensino e Pesquisa e Assistência (Faepa)doHospitaldasClínicasdaFaculdadedeMedicina deRibeirãoPretodaUniversidadedeSãoPaulo,processn. 1712/2015.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
ToFaepa,theSchoolBoardofRibeirãoPreto,parentsand studentswhoagreedtoparticipateindatacollection.
References
1.Autoria não referida. Obesity: preventing and managing the global epidemic. World Health Organ Tech Rep Ser. 2000;894:1---253.
2.ABESO.ConsensoLatino-AmericanoemObesidade1998. Avail-able from: http://crn1.org.br/images/teses/obesidade.doc [cited30.05.14].
3.AlvesJG,FigueiraF.Doenc¸asdoadultocomraízesnainfância. 2nded.Recife:Medbook;2010.
4.DietzWH, Gortmaker SL. Do we fatten our children at the televisionset? Obesityandtelevisionviewinginchildrenand adolescents.Pediatrics.1985;75:807---12.
5.Tee E.Obesity in Asia: prevalence and issues in assessment methodologies.AsiaPacificJClinNutr.2002;11:S694---701. 6.BradyTM,FivushB,FlynnJT,ParekhR.Abilityofbloodpressure
topredictleftventricularhypertrophyinchildrenwithprimary hypertension.JPediatr.2008;152:73---8.
7.GuillaumeM.Definingobesity inchildhood: currentpractice. AmJClinNutr.1999;70:126S---30S.
8.DeOnisM,Blössner M.Prevalence and trendsofoverweight amongpreschool childrenin developingcountries.AmJClin Nutr.2000;72:1032---9.
9.Victorino SV, Soares LG,Marcon SS, Higarashi IH.Viver com obesidade infantil: a experiência de crianc¸as inscritas em programa de acompanhamento multidisciplinar. Rev Rene. 2014;15:980---9.
10.Schuch I,Castro TG, Vasconcelos FA, DutraCL,Goldani MZ. Excesso de peso em crianc¸as de pré-escolas: prevalência e fatoresassociados.JPediatr(RioJ).2013;89:179---88. 11.SoteloYD,ColugnatiFA,TaddeiJA.Prevalênciadesobrepeso
e obesidade entre escolares da rede pública segundo três critérios de diagnósticoantropométrico. Cad Saúde Pública. 2004;20:233---40.
12.CostaRF,CintraIP,FisbergM.Prevalenceofoverweightand obe-sityinschoolchildrenofSantoscity,Brazil.ArqBrasEndocrinol Metab.2006;50:60---7.
13.Nascimento VG, SchoepsDD, Souza SB, SouzaJM, Leone C. Riskofoverweightandobesityinpreschoolers attending pri-vateandphilanthropicschools.RevAssocMedBras.2011;57: 657---61.
14.StrufaldiMW,SilvaEM,PucciniRF.Sobrepesoeobesidadeem escolarespré-púberes: associac¸ãocom baixopeso aonascer eantecedentes familiaresparadoenc¸acardiovascular. Embu-RegiãoMetropolitanadeSãoPaulo,2006.CiencSaúdeColet. 2011;16:4465---72.
15.UNICEF. Educac¸ão no Brasil melhora, mas desigualdades aindacriambarreiras.Availablefrom:http://www.unicef.org/ brazil/pt/media 14931.htm[cited10.02.15].
16.Brasil---InstitutoBrasileirodeGeografiaeEstatística.Pesquisa de Orc¸amentos Familiares(POF) 2008-2009:antropometria e estadonutricionaldecrianc¸as,adolescenteseadultosnoBrasil. RiodeJaneiro:IBGE;2010.Availablefrom:http://www.ibge. gov.br/home/estatistica/populacao/condicaodevida/pof/2008 2009encaa/comentario.pdf[cited20.02.15].
17.Brasil;MinistériodoPlanejamento,Orc¸amentoeGestão; Insti-tutoBrasileirodeGeografiaeEstatística.PesquisaNacionalde Sáudedo Escolar 2012. Brasília:IBGE;2013. Available from: http://biblioteca.ibge.gov.br/visualizacao/livros/liv64436.pdf 18.Diniz IM,LopesAS, DummelCC,Rieger T.Crescimentofísico eadiposidadecorporalde escolares. RevBrasCineantropom DesempenhoHum.2006;8:32---8.
19.Diniz IM, Lopes AD, Borgatto AF. Crescimento físico e composic¸ãocorporaldeescolaresdediferentesgruposétnicos doEstadodoRioGrandedoSul,Brasil.RevBrasCineantropom DesempenhoHum.2008;10:12---8.
20.SouzaMC,TibúrcioJD,BicalhoJM,RennóHM,DutraJS, Cam-posLG,etal.Factorsassociatedwithobesityandoverweight in school-aged children. Texto Contexto Enferm. 2014;23: 712---9.
21.RamosMD,PontesER,RamosMD,BarrosVR.Sobrepesoe obesi-dadeem escolaresde10a14anos.RevBrasPromocSaude. 2014;26:223---32.
22.CabreraTF,CorreiaIF,SantosDO,PacagnelliFL,PradoMT,Silva TD,etal.Análisedaprevalênciadesobrepesoeobesidadee doníveldeatividadefísicaemcrianc¸aseadolescentesdeuma cidadedosudoestedeSãoPaulo.RevBrasCrescimentoDesenvol Hum.2014;24:67---72.
23.LopesPC,PradoSR,ColomboP.Fatoresderiscoassociadosà obesidadeesobrepesoemcrianc¸asemidadeescolar.RevBras Enferm.2010;63:73---8.
24.XuS,XueY.Pediatricobesity:causes,symptoms,prevention, andtreatment.ExpTherMed.2016;11:15---20.
25.Rettner R. Obesity: causes, complications and treatment. Live Science. Available from: www.livescience.com/34787-obesity-high-bmi-causes-diabetes-heart-disease.html [cited 10.02.16].
27.Han JC, Lawlor DA, Kimm SY. Childhood obesity. Lancet. 2010;375:1737---48.
28.GlazerG.Long-termpharmacotherapyofobesity2000:areview ofefficacyandsafety.ArchInternMed.2001;161:1814---24. 29.Ciesla E, Mleczko E, Bergier J, Markowska M, Nowak-Starz
G. Health-relatedphysical fitness,BMI, physicalactivity and
timespentatacomputerscreenin6and7-year-oldchildren fromruralareasin Poland.AnnAgric EnvironMed.2014;21: 617---21.