w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Mobilization
and
collection
of
CD34
+
cells
for
autologous
transplantation
of
peripheral
blood
hematopoietic
progenitor
cells
in
children:
analysis
of
two
different
granulocyte-colony
stimulating
factor
doses
Kátia
Aparecida
de
Brito
Eid
a,b,∗,
Eliana
Cristina
Martins
Miranda
a,
Simone
dos
Santos
Aguiar
a,baUniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
bCentroInfantilBoldrini,Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received29July2014 Accepted15September2014 Availableonline17February2015
Keywords:
Hematopoieticstemcell mobilization
Leukapheresis
Granulocytecolony-stimulating factor
Autologoustransplantation
a
b
s
t
r
a
c
t
Introduction:Theuseofperipheralhematopoieticprogenitorcells(HPCs)isthecellchoice inautologoustransplantation.Theclassicdoseofgranulocyte-colonystimulatingfactor (G-CSF)formobilizationisasingledailydoseof10g/kgofpatientbodyweight.Thereisa theorythathigherdosesofgranulocyte-colonystimulatingfactorappliedtwicedailycould increasethenumberofCD34+cellscollectedinfewerleukapheresisprocedures.
Objective:Theaimofthisstudywastocompareafractionateddoseof15gG-CSF/kgof bodyweightandtheconventionaldoseofgranulocyte-colonystimulatingfactorinrespect tothenumberofleukapheresisproceduresrequiredtoachieveaminimumcollectionof 3×106CD34+cells/kgbodyweight.
Methods:Patientsweredividedintotwogroups:Group10–patientswhoreceivedasingle dailydoseof10gG-CSF/kgbodyweightandGroup15–patientswhoreceivedafractioned doseof15gG-CSF/kgbodyweightdaily.Theleukapheresisprocedurewascarriedoutinan automatedcellseparator.Theautologoustransplantationwascarriedoutwhenaminimum numberof3×106CD34+cells/kgbodyweightwasachieved.
Results:Group10comprised39patientsandGroup15comprised26patients.Atotalof146 apheresisprocedureswereperformed:110(75.3%)forGroup10and36(24.7%)forGroup 15.For Group10,a medianofthree(range:1–7)leukapheresis proceduresanda mean of8.89×106 CD34+cells/kgbodyweight(±9.59)werecollectedwhereasforGroup15the
correspondingvalueswereone(range:1–3)and5.29×106cells/kgbodyweight(±4.95).A
sta-tisticallysignificantdifferencewasfoundinrelationtothenumberofapheresisprocedures (p-value<0.0001).
∗ Correspondingauthorat:RuaEngArturCanguc¸u,275,apt21,VilaAndradeNeves,130070-293Campinas,SP,Brazil.
E-mailaddress:[email protected](K.A.d.B.Eid). http://dx.doi.org/10.1016/j.bjhh.2015.02.006
Conclusions: Tocollectaminimumtargetof3×106CD34+cells/kgbodyweight,the
admin-istrationofafractionateddoseof15gG-CSF/kgbodyweightsignificantlydecreasedthe numberofleukapheresisproceduresperformed.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
Introduction
Theautologoustransplantationofperipheralhematopoietic progenitorcells (HPCs)iswidelyusedtotreatsolidtumors andlymphomasinchildren,adolescentsandyoungadults.1–3 Since the end of the 1980s the use of leukapheresis has beenthemostusedmethodtoharvestcellsforautologous transplantationasitisconsideredtobeeffectiveandsafe, pro-motingafasterhematopoieticrecoveryandposinglessriskto thepatient(nogeneralanesthesiaandnoanemia).Asa con-sequence,thismethodisassociatedwithlowercostandthere islessriskofcontaminationofthegraftbyneoplasticcells comparedtobonemarrow.4AccordingtotheCenterfor Inter-nationalBloodandMarrowTransplant Research(CIBMTR),5 around32,000transplantswerecarriedoutinthelastdecade with,inmostcases,thecellsourcebeingperipheralHPCs.5In 91%ofcaseswhereabonemarrowtransplantisneededinthe childpopulationoftheUS,peripheralHPCsareharvestedwith themostcommonreasonsfortreatmentbeinglymphomas andsolidtumors.5
Myelosuppressive chemotherapy or high doses of chemotherapy in association with granulocyte-colony stimulating factor (G-CSF) has been successfully used in the mobilization of peripheral HPCs with a reduction of contamination byneoplastic cells.6,7 These treatments are safeandwelltoleratedwithalargecapacityformobilization andactionagainstneoplasticcells.Cyclophosphamide(CY), aloneorincombinationwithotheragents,isthemost com-monlyused chemotherapydrug8 although other regimens suchastheifosfamide,carboplatinandetoposide(ICE)and dexamethasone,adriamycinandcisplatin regimens (DHAP) arealsoemployed.9–11However,themosteffectiveregimen, withthemostsuitableintensityofmobilization,remainsto bedefined.4,12
G-CSFisthemostpotentcytokineavailable4andtheone mostcommonlyusedforthemobilizationofperipheralHPCs.5 G-CSFhaslowtoxicityandiswelltolerated.Themost com-mon side effect ismild bone pain, beginning aftertwo or threeapplications,13 however, few patients needto reduce thedoseordiscontinuetreatment.4Inautologous transplan-tation,theclassicG-CSFdoseformobilizationis10g/kgof patient body weight (bw) via subcutaneous administration onceaday.12,14 Somestudieshaveshownthatlargerdoses of G-CSF and fractionated doses given in two daily appli-cationsincrease the number ofCD34+ cells collected with alowernumber ofleukapheresisprocedures.15,16 Moreover, inpatientswhosemobilizationfailedwiththeconventional dose of G-CSF, an increase in the dose to 12.5–50g/kg bw/daycanbesuccessful.6,17 SubcutaneousG-CSF adminis-trationachievesamaximumserum levelwithin2–8hafter
applicationwithahalf-lifeof3–4h.18Thus,asingledaily appli-cationmaynotbeoptimal.18
Therecognizedmethodofharvesting peripheralHPCsis large-volumeleukapheresis(LVL).5 Withcurrenttechnology, leukapheresiscanbecarriedoutinveryyoungchildrenwith lowweights(<10kg),allowingasufficientnumberofCD34+ cellstobecollectedforcompletebonemarrowrecoveryafter highdosesofsafelyappliedchemotherapy.18–20
Thedeterminationofthetime atwhich tobegin leuka-pheresis isbasedonseveralfactors,suchasthe kineticsof leukocyterecoveryaftermyelosuppressivechemotherapy,the peripheralplateletcount,theabsolutenumberofleukocytes intheperipheralbloodandtheconcentrationofcirculating peripheralCD34+cells.21–23Themostcommonlyapplied crite-riaare anabsoluteleukocyte count≥1×103 cells/Land a CD34+cellconcentration≥10cells/L.22,23
TheincreasedcirculationofperipheralCD34+ cellsafter mobilizationlastsashorttimeandthusitisfundamentalthat apheresisiscarriedoutduringthisperiodinordertocollect asufficientnumberofCD34+cells.ThepeakinCD34+cellsis reachedaftertheleukocytenadirintherecoveryfromaplasia causedbymyelosuppressivechemotherapy.24Themomentat which there isa sufficientquantity ofCD34+ cells for col-lectionbyapheresisiswhentheperipheralleukocytecount reaches≥1×103cells/Lafterrecoveryfromthenadir.25 Con-sequently,it isproposed thattheperipheralHSCcollection shouldbeginwhenthetotalleukocytecountreaches≥1×103 cells/LafterthenadirandtheconcentrationofCD34+cellsin peripheralbloodis≥10cells/L.22,23Oneofthebestindicators ofhematopoieticrecoveryinautologoustransplantationisthe amountofinfusedCD34+cells/kgbw.16Theminimumvalues fortheacceptablenumberofCD34+cellstoachieveafast,safe andeffectiveengraftmentafterautologoustransplantationis between2and5×106/kgbw.4,26,27
InordertoobtaintheidealnumberofCD34+cellscollected forautologoustransplantationinchildren,thisstudy inves-tigates whether the useofG-CSF ata fractionateddoseof
15g/kgbwwouldreducethenumberofleukapheresis
proce-duresrequiredtoachieveaminimumnumberofCD34+cells of3×106/kgbwandcomparestheresultswiththoseobtained usingtheconventionalsingledoseof10g/kgbwG-CSF.
Methods
Table1–Characteristicsofpatientsineachgroup.
Variable Group10
n=39
Group15
n=26
Gender–n(%)
Male 23(59) 13(50)
Female 16(41) 13(50)
Race–n(%)
White 32(82) 20(77)
Non-White–n(%) 7(18) 6(23) Age–median(range) 12(1–20) 6(1–22)
Diagnosis–n(%)
HL 19 2
NHL 6 2
Solidtumor 14 22
PriorCT–median(range) 2(1–3) 2(1–4)
HL: Hodgkin lymphoma; NHL: Non-Hodgkin lymphoma; Solid tumor: Germ cell tumor, Neuroblastoma, Ewing sarcoma and Medulloblastoma;CT:Chemotherapytreatment
andmobilizedwithchemotherapyandG-CSF.Thestudywas approvedbytheappropriateethicscommitteeandinformed consentformsweresignedbythepatientsortheirguardians. Thepatientsweredividedintotwogroups:Group10was comprisedofpatientswhoreceivedasingledailydoseof10g G-CSF/kgbwbetweenDecember1998andDecember2008and Group15wascomprisedofpatientswhoreceiveda fraction-ateddailydose(definedbelowinthesectiononG-CSF)of15g G-CSF/kgbwbetweenAugust2010andApril2013.Thepatient characteristicsaredetailedinTable1.
Mobilization
chemotherapy
The mobilization chemotherapy regimens (MCR) adminis-tered using cyclophosphamide (Regimen A) included CY (cyclophosphamide 4g/m2/day×1 day), Topo/CY (topote-can 0.75mg/m2/day×5 days and cyclophosphamide 250mg/m2/day×5 days), Cy/Vp-16 (cyclophosphamide 4–7g/m2/day×1 day and etoposide 4g/m2/day×1 day), Cy/MTX/VP-16 (cyclophosphamide 4–7g/m2/day×1 day, methotrexate8g/m2/day×1dayandetoposide4g/m2/day×1 day) and Cy/Adria (cyclophosphamide 2.4g/m2/day×2 days and adriamycin 20mg/m2/day×3 days) and those without cyclophosphamide (Regimen B) were ICE (ifos-famide 3g/m2/day×3 days, carboplatin 500mg/m2/day×2 days and etoposide 150mg/m2/day×3 days), TIP (taxol 175mg/m2/day×1 day, ifosfamide 1.2g/m2/day×5 days and cisplatin 20mg/m2/day×5 days), IFO/Vp-16 (ifos-famide 2.5g/m2/day×5 days, cisplatin 40mg/m2/day×4 days, doxorubicin 10mg/m2/day×4 days and etopo-side 125mg/m2/day×4 days), DHAP (dexamethasone 40mg/day×4 days, cytarabine: 400mg/m2/day×1 day and cisplatin100mg/m2/day×1day).
Granulocyte-colonystimulatingfactor
G-CSF(Granulokine®;Roche,SP,Brazil/Leucin®;Bergamo,SP, Brazil/Filgrastine®;Blausiegel,SP,Brazil)isthemostpotent cytokineavailableandisthemostusedinthemobilization
ofperipheralHPCs5,6asithassynergisticactionswithother growthfactorswhichinducemobilization.Inthisstudythe administrationofG-CSF wasstarted onedayafterthe end oftheMCR.TheG-CSFwasadministeredsubcutaneouslyat 6:00a.m.asasingledoseforGroup10(10g/kgbw)andas twodosesforGroup15,10g/kgbwat6:00a.m.and5g/kg bwat6:00p.m.Thiswascontinueddailyforbothgroupsuntil successfulcollectionoftheminimumamountof3×106CD34+ cells/kgbworuntilthecharacterizationoflackofmobilization wasdeterminedbyanunsuccessfulcollection.
Vascularaccess
A non-completely implantable two-way central venous catheterwasintroducedintoallpatientsinordertocarryout theLVL.
Large-volumeleukapheresis
Leukapheresis was carriedout inan automaticcontinuous flow cell separator with the anticoagulant citratedextrose solution (ACD-A– CS3000plus®; Cobe-spectra®; Com.tec®). ThefirstLVLprocedureforGroup15wascarriedoutafterthe MCRwith≥1×103cells/Lofleukocytesand≥10cells/Lof CD34+intheperipheralbloodandforGroup10with≥1×103 cells/Lofleukocytes.Patientswhoweighed<20kgreceived priming withirradiatedand filteredpackedred blood cells (PRBCs) (20mL/kgbw).Duringthe LVLall patientsreceived intravenous(IV)replacementofcalcium,sodium,potassium andmagnesiumandwereundercontinuousmonitoring.Four blood volumeswere processedperleukapheresisprocedure and if symptoms and/or signs of hypocalcemia related to the anticoagulant used in the cell separator system were observed, adose of0.2mL/kgbwof10%calciumgluconate was administered intravenously. All patients who did not reachtheminimumnumberofCD34+cells(3×106/kgbw)in thefirstleukapheresisprocedureweresubmittedtoanother procedureonthefollowingdayregardlessofthenumberof leukocytesandCD34+cellsintheperipheralblood.Alimitof twomoreleukapheresisprocedureswassetforGroup15but withnolimitinthenumberofproceduresforGroup10.
Completebloodcountafterlarge-volumeleukapheresis
A complete blood count was obtained aftereach LVL pro-cedure.Aprophylactic transfusionwascarried outwithan irradiatedandfilteredplateletconcentrate(PC)ifthenumber ofplateletsintheperipheralbloodwas<10×103cells/Land irradiatedandfilteredPRBCtransfusionifthehemoglobin(Hb) was<8.0g/dL.
Peripheralhematopoieticprogenitorcellanalysis
Table2–Mobilizationchemotherapyregimens(MCR).
MCR Group10 Group15 p-value
A 23 22 0.03
B 16 4
Statisticalanalysis
Adescriptiveanalysisofallvariablesinvolvedwascarriedout andthentheChisquaredorFisherexacttestswereapplied asappropriatetothecategoricalvariableswhiletheStudent
t-testwasappliedtothecontinuousvariablestocomparethe meansofGroups10and15.Statisticalsignificancewassetfor
p-values<0.05.TheStatisticalPackagefortheSocialSciences (SPSS)version21.0wasuseinallanalyses.
Results
Fifty-three patients received 10g G-CSF/kg bw between December 1998 and December 2008 (Group 10). Fourteen patientswereexcludedfromtheanalysis:eightmobilizedonly withG-CSF,onewas29yearsofageandmobilizationfailed infivecases.BetweenAugust2010andApril2013,35patients receivedafractionateddoseof15gG-CSF/kgbwdaily(Group 15)withninebeingexcludedfromtheanalysisdueto mobi-lizationfailure.
Ofthe65patientsanalyzed,55.4%weremale,themedian age was ten years (1–22), 80% were white and 55.4% were diagnosed with solid tumors. Themedian number of pre-mobilizationchemotherapycyclesreceivedwastwoforboth groups;varyingfromonetothreeforGroup10andonetofour forGroup15,withnostatisticallysignificantdifference,and withnoinfluenceonthenumberofCD34+cellscollected.
Withregard tothe MCR, Regimen A was used in23/39 (59%) of cases of Group 10 and 22/26 (84%) of cases of Group15resultinginastatisticallysignificantdifference(p -value=0.03)(Table2).However,nodifferenceintheleukocyte recoverytime(≥1×103 cells/L) wasobservedbetweenthe tworegimensandtheMCRdidnotinfluencethenumberof leukapheresisprocedurespergroupandnopatientshad MCR-relatedcomplications.
Regimen A: CY (cyclophosphamide 4g/m2/day×1 day),
Topo/CY(topotecan0.75mg/m2/day×5daysand cyclophos-phamide 250mg/m2/day×5 days), Cy/Vp-16 (cyclophos-phamide 4–7g/m2/day×1 dayand etoposide 4g/m2/day×1 day),Cy/MTX/Vp-16(cyclophosphamide4–7g/m2/day×1day, methotrexate8g/m2/day×1dayandetoposide4g/m2/day×1 day)andCy/Adria(cyclophosphamide 2.4g/m2/day×2days andadriamycin20mg/m2/day×3days).
RegimenB:ICE(ifosfamide3g/m2/day×3days,carboplatin
500mg/m2/day×2 days and etoposide 150mg/m2/day×3 days), TIP (taxol 175mg/m2/day×1 day, ifosfamide 1.2g/m2/day×5 days and cisplatin 20mg/m2/day×5 days/), IFO/Vp-16 (ifosfamide 2.5g/m2/day×5 days, cis-platin40mg/m2/day×4days,doxorubicin 10mg/m2/day×4 days and etoposide 125mg/m2/day×4 days), DHAP (dexa-methasone40mg/day×4days,cytarabine:400mg/m2/day×1 dayandcisplatin100mg/m2/day×1day).
AllpatientsshowedgoodtolerancetoG-CSF administra-tion; no applications were suspendedor reduced ineither groupandonlyfive(13%)patientsofGroup10andtwo(7%) patientsofGroup15reportedmildbonepain.
Themediannumberofpre-leukapheresisleukocyteswas 14.4×103cells/L(range:0.9–50.3)forGroup10and22.3×103 cells/L(range:3.0–73.9)forGroup15.Themedian concen-tration of peripheral CD34+ cells was 27.9 per L (range: 1.10–135.0)forGroup10and29.5cellsperL(range:8.0–90.0) for Group 15, with no statistically significant difference between values. Nopatients had complicationsduring the leukapheresisprocedureineithergroup;nohypovolemiawas observedinchildrenwhoweighed<20kgandonlytwo(5%) patientsinGroup10reportedmildparesthesiarelatedtothe useoftheanticoagulant.Thirty-twopatients,15(38%)from Group 10 and 17(65%) from Group15,had platelet counts <50×103cells/Lduringthepre-leukapheresisperiod. How-ever,notypeofbleedingoccurredandonlyone(3%)patientof Group15receivedpost-leukapheresisirradiatedandfiltered PC.Noneofthepatientsfromeithergroupreceiveda trans-fusion ofirradiatedand filtered PRBCs afterleukapheresis. Three(7%)casesinGroup10and11(42%)casesinGroup15 receivedprimingofirradiatedandfilteredPRBCsduringthe leukapheresisprocedure.
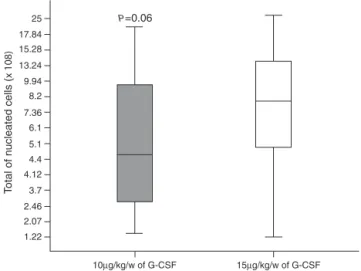
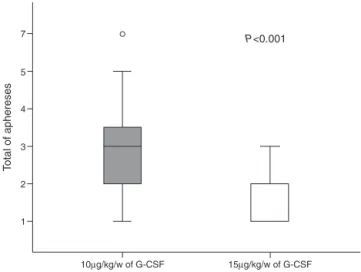
Atotalof146leukapheresisprocedureswerecarriedout, 110inGroup10and36 inGroup15,withanaverage dura-tion of4h(±2);thesecond leukapheresisprocedure ofone patient in Group 15 was interrupted half-way through the procedureduetomalfunctioningofthecellseparator;there was malfunctioningofthe catheterinfour patients. More-over, one patient of Group 10 and one of Group 15 had prolonged LVLtimes and it wasnotpossible tocollect the minimum number of CD34+ cells in two cases of Group 15.Amedianofthree(range:1–7)leukapheresisprocedures were performedforGroup10withmediansof7.22×108/kg bw (range: 1.28–20.70) and 8.89×106/kg bw (range: 0.3–45) ofnucleatedcells(NCs) andCD34+ cells,respectivelybeing collected. In Group 15 there was a median of one leuka-pheresisprocedure(range:1–3)andmediansof10.17×108/kg bw NCs (range:1.22–37.0) and 5.29×106 CD34+ cells/kg bw (range:0.6–27.8)werecollected(Figures1and2).Themedian
10µg/kg/w of G-CSF 15µg/kg/w of G-CSF
P=0.06 25
17.84 15.28
13.24 9.94 8.2
7.36 6.1
5.1 4.4 4.12
3.7
2.46 2.07 1.22
T
otal of n
ucleated cells (
x 108)
P=0.02 30.0
24.0
18.0
12.0
6.0
0.0
T
o
tal of collected CD34+ (x 106)
10µg/kg/w of G-CSF 15µg/kg/w of G-CSF
°
Figure2–TotalnumberofcollectedCD34+cells.
°
75
4
3
2
1
T
o
tal of aphereses
P<0.001
10µg/kg/w of G-CSF 15µg/kg/w of G-CSF
Figure3–Numbersofleukapheresis.
numberofdaysofleukocyterecoverywaseight(range:0–18) forGroup10andten(range:2–13)forGroup15(p-value=0.15). Thus,statisticallysignificantdifferencesbetweengroupswere observedforthenumberofleukapheresisprocedures(p-value <0.0001)(Figure3)andthenumberofCD34+cellscollected (p-value=0.02),whilethetotalNCcountresultedinafavorable tendencytowardGroup15(p-value=0.06).
A statistically significant distribution was observed on comparing groups in respect to pre-apheresis peripheral
Table3–CollectedCD34+cellsversuspre-leukapheresis
peripheralCD34+cellcount.
Collectedcells (×106cells/L/kgbw)
Pre-leukapheresisCD34+count (×106cells/L/kgbw)
p-value
<10 ≥10
<3.0×106 9 22 0.04
≥3.0×106 3 31
Bw:bodyweight.
CD34+ cells (≥10 or<10 cells/L)and thenumber ofCD34+ cellscollected(≥3.0or<3.0×106cells/L)(Table3).
Discussion
Some authors23,29 suggest that the number of pre-MCR receivednegativelyinfluencesthenumberofCD34+cells col-lected,whichwasnotobservedinthisstudy.TheMCRusedin thisstudydidnotcausecomplications,eveninpatients tak-ing highdosesofcyclophosphamide(4–7g/m2).Itisknown thateachpatientrespondsinadistinctwaytomobilization andthatotherparametersmayhaveanegativeeffect,suchas thetimebetweenthediagnosisandharvest,previous irradia-tion,thrombocytopeniaatthetimeofmobilizationandmany otherfactorscitedintheliterature.5,23,28,29 Consequently,in thisstudyitwasnotpossibletodefinethebestmobilization chemotherapyregimenasisreportedintheliterature.4,12
The administration of G-CSF was well tolerated as the onlysideeffectreportedbythepatientswasmildbonepain in 10% of the cases which is the side effect most com-monlyreported.13PrimingwithirradiatedandfilteredPRBCs ofchildrenweighingbelow20kgallowedtheLVLprocedure to be safely carried out without complications. In the two casesofmildanticoagulant-relatedparesthesia,thecondition wasrevertedusingintravenouscalciumgluconate.Problems related tothe non-completely implantedtwo-way catheter werefewwithonlyaround6%ofthecathetersmalfunctioning, alowerratethanreportedintheliterature.22,29
Withtheexceptionofoneleukapheresisprocedure(1/146), whichwasinterruptedhalfwaythrough,thecellseparators functioned acceptablyand therewasnoneedfortechnical adjustmentintheotherleukapheresisprocedures.Thetime ofleukapheresiswaswelltoleratedincludingbyunder 5-year-oldchildrenastherewerenocomplaintsfrompatientswho experiencedprolongedprocessingtimes;thesepatientsdid notshowsignsorsymptomsofanticoagulant-related hypocal-cemia.
Theabsoluteperipheralleukocytecount(≥1×cells/L)and CD34+cellconcentration(≥10cells/L)werefoundtobegood parameters tostart leukapheresis,inparticularthe periph-eralCD34+cellconcentration(≥10cells/L),eventhoughthis parametercannotbeusedforallpatients.
Conclusions
Thisstudydemonstratedthatthemobilizationandcollection ofperipheralHPCsinchildrenisviableandsafe.Theabsolute peripheralleukocytecount(≥1×103cells/L)andCD34+cell concentration(≥10cells/L),whenusedtogether,aregood parameterstoindicatethestartofleukapheresis.The fraction-atedapplication of15gG-CSF/kgbwsignificantlyreduced thenumberofleukapheresisproceduresneededtocollecta minimumof3×106cells/kgbwCD34+cells.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest
r
e
f
e
r
e
n
c
e
s
1. LadensteinR,PötschgerU,HartmanO,PearsonAD,Klingebiel T,CastelV,etal.28yearsofhigh-dosetherapyandSCTfor neuroblastomainEurope:lessonsfrommorethan4000 procedures.BoneMarrowTransplant.2008;41Suppl. 2:S118–27.
2. MatthayKK,ReynoldsCP,SeegerRC,ShimadaH,AdkinsES, Haas-KoganD,etal.Long-termresultsforchildrenwith high-riskneuroblastomatreatedonarandomizedtrialof myeloablativetherapyfollowedby13-cis-retinoicacid:a children’soncologygroupstudy.JClinOncol.
2009;27(7):1007–13.
3. BurkhardtB,ReiterA,LandmannE,LangP,LassayL,
DickerhoffR,etal.Pooroutcomeforchildrenandadolescents withprogressivediseaseorrelapseoflymphoblastic
lymphoma:areportfromtheBerlin-Frankfurt-Munster Group.JClinOncol.2009;27(20):3363–9.
4. CastroCGJr,BrunettoA,etal.Transplanteautogênicode células-troncohematopoiéticasemlinfomasdeHodgkinna infânciaeadolescência.Experiênciadoservic¸odeoncologia pediátricadohospitaldeClínicasdePortoAlegre.RBHH. 2011;33Suppl.1:109.
5. NerviB,LinkDC,DiPersioJF.Cytokinesandhematopoietic stemcellmobilization.JCellBiochem.2006;99(3):690–705. 6. PasquiniMC,WangZ,HorowitzMM,GaleRP.2010reportfrom
theCenterforInternationalBloodandMarrowTransplant Research(CIBMTR):currentusesandoutcomesof hematopoieticcelltransplantsforbloodandbonemarrow disorders.ClinTransplant.2010;8:7–105.
7. RavagnaniF,SienaS,BregniM,SciorelliG,GianniAM, PellegrisG.Large-scalecollectionofcirculating
haematopoieticprogenitorsincancerpatientstreatedwith high-dosecyclophosphamideandrecombinanthuman GM-CSF.EurJCancer.2014;26(5):562–4.
8. BensingerWI,WeaverCH,AppelbaumFR,RowleyS,Demirer T,SandersJ,etal.Transplantationofallogeneicperipheral bloodstemcellsmobilizedbyrecombinanthuman granulocytecolony-stimulatingfactor.Blood. 2014;85(6):1655–8.
9. WatanabeT,KawanoY,KanamaruS,OnishiT,KanekoS, WakataY,etal.Endogenousinterleukin-8(IL-8)surgein granulocytecolony-stimulatingfactor-inducedperipheral bloodstemcellmobilization.Blood.1999;93(4):1157–63. 10.BurtnessBA,PsyrriA,RoseM,D’AndreaE,Staugaard-HahnC,
Henderson-BakasM,etal.AphaseIstudyofpaclitaxelfor mobilizationofperipheralbloodprogenitorcells.Bone MarrowTransplant.1999;23(4):311–5.
11.SuredaA,PetitJ,BrunetS,BoquéC,AventínA,MartinoR, etal.Mini-ICEregimenasmobilizationtherapyforchronic myelogenousleukaemiapatientsatdiagnosis.BoneMarrow Transplant.1999;24(12):1285–90.
12.VelasquezWS,CabanillasF,SalvadorP,McLaughlinP,Fridrik M,TuckerS,etal.Effectivesalvagetherapyforlymphoma withcisplatinincombinationwithhigh-doseAra-Cand dexamethasone(DHAP).Blood.1998;71(1):117–22. 13.CaraccioloD,GavarottiP,AgliettaM,BondesanP,FaldaM,
GalloE,etal.High-dosesequential(HDS)chemotherapywith bloodandmarrowcellautograftassalvagetreatmentinvery poorprognosis,relapsednon-Hodgkin’slymphoma.Bone MarrowTransplant.1993;12(6):621–5.
14.WatanabeH,WatanabeT,SuzuyaH,WakataY,KanekoM, OnishiT,etal.Peripheralbloodstemcellmobilizationby granulocytecolony-stimulatingfactoraloneandengraftment kineticsfollowingautologoustransplantationinchildrenand adolescentswithsolidtumor.BoneMarrowTransplant. 2006;37(7):661–8.
15.AnderliniP,PrzepiorkaD,SeongD,MillerP,SundbergJ, LichtigerB,etal.Clinicaltoxicityandlaboratoryeffectsof granulocyte-colony-stimulatingfactor(filgrastim) mobilizationandbloodstemcellapheresisfromnormal donors,andanalysisofchargesfortheprocedures. Transfusion.1996;36(7):590–5.
16.AkizukiS,MizorogiF,InoueT,SudoK,OhnishiA. Pharmacokineticsandadverseeventsfollowing5-day repeatedadministrationoflenograstim,arecombinant humangranulocytecolony-stimulatingfactor,inhealthy subjects.BoneMarrowTransplant.2000;26(9):939–46. 17.AnderliniP,ChamplinR.Useoffilgrastimforstemcell
mobilisationandtransplantationinhigh-dosecancer chemotherapy.Drugs.2014;62Suppl.1:79–88. 18.EngelhardtM,BertzH,AftingM,WallerCF,FinkeJ.
High-versusstandard-dosefilgrastim(rhG-CSF)for mobilizationofperipheral-bloodprogenitorcellsfrom allogeneicdonorsandCD34(+)immunoselection.JClinOncol. 2014;17(7):2160–72.
19.KrögerN,ZellerW,HassanHT,KrügerW,GutensohnK, LöligerC,etal.StemcellmobilizationwithG-CSFalonein breastcancerpatients:higherprogenitorcellyieldby deliveringdivideddoses(2×5microg/kg)comparedtoa singledose(1×10microg/kg).BoneMarrowTransplant. 1999;23(2):125–9.
20.KobbeG,SöhngenD,BauserU,SchneiderP,GermingU,Thiele KP,etal.FactorsinfluencingG-CSF-mediatedmobilizationof hematopoieticprogenitorcellsduringsteady-state
hematopoiesisinpatientswithmalignantlymphomaand multiplemyeloma.AnnHematol.1999;78(10):456–62. 21.CecynKZ,SeberA,GinaniVC,Gonc¸alvesAV,CaramEM,
OguroT,etal.Large-volumeleukapheresisforperipheral bloodprogenitorcellcollectioninlowbodyweightpediatric patients:asinglecenterexperience.TransfusApherSci. 2005;32(3):269–74.
22.FontanaS,GroebliR,LeibundgutK,PabstT,ZwickyC, TaleghaniBM.Progenitorcellrecruitmentduring
individualizedhigh-flow,very-large-volumeaphaeresisfor autologoustransplantationimprovescollectionefficiency. Transfusion.2006;46(8):1408–16.
23.RavagnaniF,ColucciaP,NottiP,ArientiF,BompadreA,Avella M,etal.Peripheralbloodstemcellcollectioninpediatric patients:feasibilityofleukapheresisunderanesthesiain uncompliantsmallchildrenwithsolidtumors.JClinApher. 2006;21(2):85–91.
24.GinaniV,SeberA,etal.Leucaféresesdegrandevolumepara coletadecélulas-troncohematopoiéticasperiféricas
25.ToLB,RobertsMM,HaylockDN,DysonPG,BranfordAL,Thorp D,etal.Comparisonofhaematologicalrecoverytimesand supportivecarerequirementsofautologousrecoveryphase peripheralbloodstemcelltransplants,autologousbone marrowtransplantsandallogeneicbonemarrowtransplants. BoneMarrowTransplant.1992;9(4):277–84.
26.CagnoniPJ,ShpallEJ.Mobilizationandselectionof CD34-positivehematopoieticprogenitors.BloodRev. 1996;10(1):1–7.
27.MarquesJF.Mobilizac¸ãoecoletadascélulasprogenitoras periféricashemopoiéticasperiféricasparatransplante
autólogoempacientesonco-hematológicos.RevBras HematolHemoter.2000;22(2):135–6.
28.DelamainM.Correlac¸ãoentreaquantidadedecélulasCD34+ circulanteseacoletaporaféresedeCPPempacientes onco-hematológicos.Campinas,SãoPaulo,Brasil:
UniversidadeEstadualdeCampinas;2004.Tesedemestrado. 29.DregerP,KlössM,PetersenB,HaferlachT,LöfflerH,Loeffler