Arq Bras Cardiol 2001; 77: 81-4.
Alessi et al Fibroelastoma of the mitral valve
81 81
Hospital Nossa Senhora das Graças – Curitiba
Mailing address: Alexandre Alessi - Rua Padre Agostinho, 1923/1701 – 80710-000 – Curitiba, PR, Brazil - e-mail: [email protected]
English version by Stela Maris C. e Gandour
Alexandre Alessi, Roberto Gomes de Carvalho, Dalton Bertolin Précoma, Débora Fontoura, Luciano Rodrigo Oliveira, José Zanis Neto, Marcello Zapparoli
Curitiba, PR - Brazil
Fibroelastoma of the Mitral Valve as a Cause of Transient
Ischemic Stroke
Case Report
A 44-year-old woman had a transient ischemic stroke, fibroelastoma of the mitral valve being the source of the em-bolus. The patient evolved with neutropenia induced by ticlopidine after 10 days of treatment. We report the major clinical features, therapeutical options, and medicamen-tous toxicity resulting from the use of antiplatelet drugs.
Less than 5% of all cardiac tumors are primary tumors, which are, therefore, a rare entity; the remaining 95% are me-tastatic tumors to the heart 1-3. Benign cardiac tumors
acco-unt for 75% of primary cardiac tumors, of which the most common are myxomas usually originating in the left atrium. Papillary fibroelastomas are rare benign primary cardiac tu-mors, and for a long time their clinical significance was unk-nown. Currently, they are recognized as a cause of neurolo-gical and cardiac symptoms 3-6.
This study aims to report peculiarities in the clinical findings of this entity in addition to reviewing current his-tologic, anatomicopathological, echocardiographic, and treatment concepts related to papilloma of the mitral valve.
Case report
A 44-year-old female sought neurological assistance on an emergency basis after an episode of transient is-chemic stroke manifested predominantly as left facial hemi-paresis of 15-minute duration. On physical examination at that time, she had no neurologic abnormalities any longer, and magnetic nuclear resonance imaging of the skull was normal. A cardiologic assessment was recommended to evaluate the cause of the transient ischemic stroke.
On the cardiologic assessment 1 week later, a search for the source of the embolism that caused the transient
ischemic stroke was started. The physical examination and the electrocardiography were normal, with no evidence of arterial hypertension, cardiac arrhythmia, or carotid arterial obstruction. The transthoracic echocardiography showed cardiac chambers of normal dimension, with no thrombi insi-de, normal left ventricular percentage systolic shortening and ejection fraction. The mitral valve showed a small mass on its anterior leaflet, and a normal and competent opening. The assessment was complemented with transesophageal echocardiography, in which a pediculate mass could be seen measuring 0.7cm x 0.7cm, with an area of 0.4cm 2 and
circum-ference of 2.4cm (figs. 1 and 2). The sequential investigation excluded the possibility of infectious endocarditis (no fever, normal hemogram, and 3 negative blood cultures), and the diagnosis of cardiac tumor was assumed as the possible embolic source. Ticlopidine was started at the dosage of 250mg twice a day, and surgical removal of the tumor was in-dicated, but refused by the patient at that time.
The patient had been healthy prior to this episode, totally asymptomatic, and was insecure in regard to the ac-tual indication and benefit of an invasive procedure like a cardiac surgery with extracorporeal circulation and associa-ted risks.
After 10 days of treatment with ticlopidine, started fe-ver (40°C), intense asthenia, chills, and nocturnal sudoresis. Her hemogram showed 3,400 leukocytes with 23% of band neutrophils. In the first 24 hours of the infectious period, the patient’s condition progressively worsened, and she was admitted to a general hospital with the diagnosis of internal otitis and bronchopneumonia. However, a hemogram with significant granulocytopenia (900 leukocytes and 12 band neutrophils) attracted attention. The treatment with an antibiotic was started associated with a colony-stimulating factor (Granulokineà). Because ticlopidine-induced granulocytopenia was suspected, this medication was suspended. The treatment proved effective after 14 days, with recovery from the infection and clinical improvement. Based on medical recommendation, the patient used low-molecular-weight heparin (20 mg of enoxaparin)
82 82
Alessi et al
Fibroelastoma of the mitral valve
Arq Bras Cardiol 2001; 77: 81-4.
taneously at home for 2 weeks more. With total clinical reco-very and partial improvement of the drug-induced granulo-cytopenia (4,800 leukocytes, 43% segmented leukocytes, and 6% band leukocytes), the patient sought a large gene-ral hospital for cardiologic and hematologic reassessment. In this new reassessment, the patient was apyretic and in good general condition. Three blood cultures were nega-tive. Her hemogram still showed mild granulocytopenia, which gradually improved during her hospitalization. It is worth noting that from the beginning of the white cell di-sorder the patient never had a low platelet count. The new cardiologic tests performed were considered similar to tho-se performed for investigating the source of the cardiac em-bolism. Surgery was indicated for removal of the benign car-diac tumor located in the mitral valve. By this time, the pa-tient agreed to this type of treatment.
Surgery was performed with access through the ante-rolateral thoracotomy in the 4th right intercostal space.
Installation of the extracorporeal circulation circuit was per-formed through cannulation of the femoral artery and both cava veins with the membrane oxygenator and Bio-Pump.
The heart was protected with anterograde injection of hy-pothermic and blood solution. After incising the left atrium, a small mass on the atrial portion of the anterior leaflet of the mitral valve was identified and easily removed without des-troying the valvar apparatus, therefore avoiding valvar re-pair. The heart was disconnected from the extracorporeal circulation circuit uneventfully. The patient was extubated in the recovery room and referred to the postoperative car-diac unit. Her postoperative evolution was excellent both from the cardiologic and hematologic points of view, and she was discharged from the hospital on the 4th
postopera-tive day.
The anatomicopathological study showed, on gross examination, a papillary fragment measuring 0.5x0.5x0.2cm, of white color, with a granular aspect, and smooth and elastic consistency (fig. 3). The microscopic study of the sections showed an anastomosing and branching papillary proliferation, similar to tendinous cords. The papillae were formed by axes of avascular tissue lined by a single layer of flat endothelial cells, compatible with papillary fibroadeno-ma of the mitral valve. These findings are different from those of the myxoma that may be located on cardiac valves; the presence of dense connective tissue, absence of ves-sels and of myxoid matrix, in addition to the presence of po-lygonal papillae in the papillary axes eliminate this possibi-lity (fig. 4).
Discussion
Primary cardiac tumors are rare and correspond to less than 5% of all cardiac tumors; the remaining 95% are metas-tatic tumors to the heart 1-3. Benign cardiac tumors
corres-pond to 75% of the primary cardiac tumors, myxomas being the most common and usually originating in the left atrium (Table I) 7.
The most frequent clinical findings are the following: asthenia, fever, weight loss, and embolic phenomena. Inci-dental or autopsy finding is, however, known to be more prevalent, as the diagnosis is not made because the clinical
Fig. 1 - Transesophageal echocardiography showing fibroelastoma on the posterior leaflet of the mitral valve.
Fig. 2 – Zoom of the transesophageal echocardiography showing the dimensions of the fibroelastoma.
Arq Bras Cardiol 2001; 77: 81-4.
Alessi et al Fibroelastoma of the mitral valve
83 83
findings are not exuberant, and most patients remain asymptomatic 8.
Papillary fibroelastomas are rare benign primary car-diac tumors. Their nomenclature becomes sometimes con-fusing because several terms (fibroma, cardiac papilloma, valvar papilloma, myxofibroma, fibroelastic hamartoma, and endocardiac papillary fibroma) have been used to name them; papillary fibroelastoma, however, is the most widely accepted name 9,10. They are classified as endocardial
tu-mors, and they may manifest as valvar insufficiency, coro-nary artery obstruction if located on the arterial surface of the aortic valve, or as an embolic complication 2,5,6. Papillary
fibroelastomas are characteristically small avascular soli-tary tumors with multiple spikelets, resembling a sea ane-mone, and adhered to the endocardium by a short pedicle 7.
Histologically, they are formed by a dense central axis of connective tissue surrounded by a layer of loose connecti-ve tissue lined by hyperplastic endothelial cells 2,4,11. They
may originate in any part of the endocardial surface, but their most common location is the valvar endocardium. In reality, papillary fibroelastomas are considered the most fre-quent primary cardiac tumor originating in the valvar endo-cardium 11. The valvar distribution predominates in the left
side of the heart, 29% of cases involving the aortic valve, 25% the mitral valve, 17% the tricuspid valve, and 13% the pulmonary valve 1. In the case of involving the semilunar
valves, the preferred location is the middle part of the valve,
Fig. 4 – Microscopy of the tumor mass showing connective tissue lined by a single layer of flat endothelial cells.
Table I – Primary cardiac tumors
Benign (75% of the cases) Myxoma Rhabdomyoma
Fibroma Lipoma Atrioventricular node tumor
Papillary fibroelastoma Hemangioma Malign (25% of the cases) Angiosarcoma
Rhabdomyosarcoma Fibrosarcoma
protruding into the atrial cavity 1. Their dimensions range
from 0.1 to 5.7cm, most of them having less than 1.5cm3.
These tumors have been reported in people of various ages, from 6-day neonates to 92-year-old patients 10. The
destri-bution is equivalent in males and females. The first surgical description of a papillary fibroelastoma by Lichtenstein et al 9 dates back to 1979. Prior to echocardiography, they were
uncommon findings of autopsy or cardiac surgeries. A re-cent review of the literature lists 198 cases of cardiac papil-lary fibroelastoma 8. Surgical treatment has been
recommen-ded and, despite the benign tissular character, early diag-nosis and treatment may prevent complications 2,8,11.
Papillary fibroelastomas are loose excrescences typi-cally located in cardiac valves. They may be single or multi-ple lesions occurring more frequently on the ventricular surfaces of semilunar valves and on the atrial surface of atrioventricular valves 9,12. Nonvalvar locations are rare and
include the mural and septal endocardium of the left or right ventricles, papillary muscles, tendinous cords, and the inti-mal layer of the coronary ostium. The tricuspid valve is most affected in children, and the mitral and aortic ones in adults 12.
The major differential diagnosis should be made with Lambl’s excrescences, which are acellular deposits lined by a single endothelial layer 3,9. They are found on sites of
en-dothelial lesions of the cardiac valves in more than 70% of the adults.
The clinical significance of muscle fibroelastomas remai-ned unknown for a long time. Currently, they are recognized as a cause of neurological and cardiac symptoms 3,6,11-13.
Embolization of a tumor fragment or of a thrombus on the tumor surface is not infrequent. A favorable situation for deposition of a niche of platelet aggregation is known to exist with posterior embolization of the fragments 14. The
neurological consequences of embolization include transi-ent ischemic strokes, convulsions, syncopes, and infarcts in the following regions: brain, cerebellum, brainstem, spinal cord, and retina 6. In a series of 71 operated upon
fibroelasto-mas, 38 cases of embolization to the central nervous system were observed 8. In reality, the embolic potential of the tumor
results from fragmentation of the papillary spikelets of the tumor or even from thrombi formed by platelets and fibrin, which, frequently adhere to the uneven tumoral surface 8,14.
Hicks et al 12, in a review of the echocardiographic evolution
of patients with papillary fibroelastoma, showed a variety of clinical presentations, the neurological manifestation being the most frequent. In reality, an embolic cerebral stroke in a young individual with no evidence of cerebrovascular di-sease, particularly in the presence of sinus rhythm, should cause suspicion of a cardiac tumor, as well as infectious en-docarditis and mitral valve prolapse 14,15.
As the physical examination of a patient with papillary fibroelastoma is usually normal, a two-dimensional echocar-diography is indicated in young patients with transient is-chemic stroke or cerebral stroke, even in the absence of clinical or electrocardiographic cardiac disease 16.
Comple-mentation of transthoracic echocardiography with
84 84
Alessi et al
Fibroelastoma of the mitral valve
Arq Bras Cardiol 2001; 77: 81-4.
1. Mc Allister HA, Fenoglio JJ. Tumors of the cardiovascular system. In: Mc Allister HA, Fenoglio JJ, editors. Atlas of Tumor Pathology. Washington DC: Armed For-ces Institute of Pathology, 1978: 20-5.
2. Ryan PE Jr, Obeid AI, Parker FB Jr. Primary cardiac valve tumors. J Heart Valve Dis 1995; 4: 222-6.
3. Salcedo EE, Cohen GI, White RD, Davison MB. Cardiac tumors: diagnosis and management. Curr Probl Cardiol 1992; 17: 73-137.
4. Cardiogenic brain embolism. Cerebral Embolism Task Force. Arch Neurol 1986; 43: 71-84.
5. Muir KW, McNeish I, Grosset DG, Metcalfe M. Visualization of cardiac emboli from mitral valve papillary fibroelastoma. Stroke 1996; 27: 1133-4. 6. Graca A, Nunes R, Costeira A, Almeida J, Bastos P. Cardiac papillary fibroelastoma
of a mitral valve chordae revealed by stroke. Rev Port Cardiol 1999; 18: 937-9. 7. Giuliani ER, Gersh BJ, McGoon MD, Hayes DL, Schaff HV. Mayo Clinic Pratice
of Cardiology. Third ed. New York: Mosby, 1996.
8. Grinda JM, Couetil JP, Chauvaud S, et al. Cardiac valve papillary fibroelastoma: surgical excision for revealed or potential embolization. J Thorac Cardiovasc Surg 1999; 117: 106-10.
9. Lichtenstein HL, Lee JC, Stewart S. Papillary tumor of the heart: incidental fin-ding at surgery. Hum Pathol 1979; 10: 473-5.
10. Shahian DM, Labib SB, Chang G. Cardiac papillary fibroelastoma. Ann Thorac Surg 1995; 59: 538-41.
11. Klarich KW, Enriquez-Sarano M, Gura GM, Edwards WD, Tajik AJ, Seward JB. Papillary fibroelastoma: echocardiographic characteristics for diagnosis and pa-thologic correlation. J Am Coll Cardiol 1997; 30: 784-90.
12. Hicks KA, Kovach JA, Frishberg DP, Wiley TM, Gurczak PB, Vernalis MN. Echocardiographic evaluation of papillary fibroelastoma: a case report and re-view of the literature. J Am Soc Echocardiogr 1996; 9: 353-60.
References
13. Mann J, Parker DJ. Papillary fibroelastoma of the mitral valve: a rare cause of tran-sient neurological deficits. Br Heart J 1994; 71: 6.
14. Daniel WG, Mugge A. Transesophageal echocardiography. N Engl J Med 1995; 332: 1268-79.
15. Grote J, Mugge A, Schfers HJ, Daniel WG, Lichtlen PR. Multiplane transoeso-phageal echocardiography detection of a papillary fibroelastoma of the aortic valve causing myocardial infarction. Eur Heart J 1995; 16: 426-9.
16. Giannesini C, Kubis N, N’Guyen A, Wassef M, Mikol J, Woimant F. Cardiac pa-pillary fibroelastoma: A rare cause of ischemic stroke in the young. Cerebrovasc Dis 1999; 9: 45-9.
17. Etienne Y, Jobic Y, Houel JF, et al. Papillary fibroelastoma of the aortic valve with myocardial infarction: echocardiographic diagnosis and surgical excision. Am Heart J 1994; 127: 443-5.
18. Leon MB, Baim DS, Popma JJ, et al. A clinical trial comparing three antithrombo-tic-drug regimens after coronary-artery stenting. Stent Anticoagulation Reste-nosis Study Investigators. N Engl J Med 1998; 339: 1665-71.
19. Yeh SP, Hsueh EJ, Wu H, Wang YC. Ticlopidine-associated aplastic anemia. A case report and review of literature. Ann Hematol 1998; 76: 87-90.
20. Kao TW, Hung CC, Chen YC, Tien HF. Ticlopidine-induced aplastic anemia: re-port of three Chinese patients and review of the literature. Acta Haematol 1997; 98: 211-3.
21. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of is-chaemic events (CAPRIE). CAPRIE Steering Committee. Lancet 1996; 348: 1329-39.
22. Bertrand ME, Rupprecht HJ, Urban P, Gershlick AH, Investigators of Double-blind study of the safety of clopidogrel with and without a loading dose in com-bination with aspirin compared with ticlopidine in comcom-bination with aspirin af-ter coronary stenting: the clopidogrel aspirin stent inaf-ternational cooperative study (CLASSICS) [In Process Citation]. Circulation 2000; 102: 624-9.
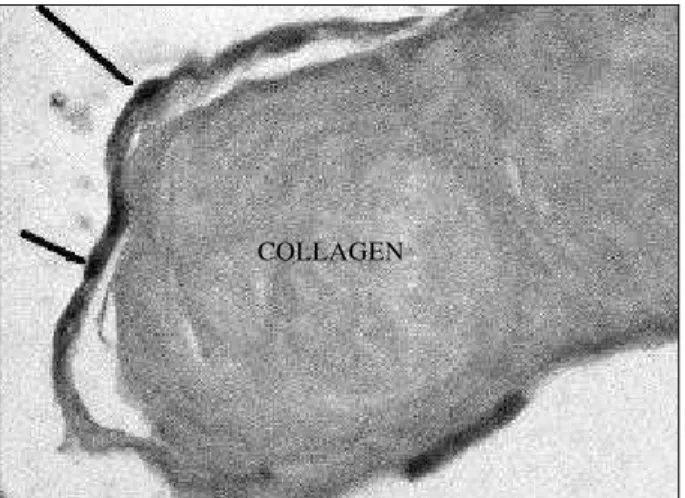
sophageal study increases diagnostic sensitivity 10,14,17.
This latter, with its high resolution, may distinguish the col-lagen center of the tumor from other cardiac structures, due to its shining echocardiographic appearance. This appea-rance helps to differentiate fibroelastomas from other intra-cardiac tumors, especially myxomas, but also from vegeta-tions and mural thrombi. Currently, transthoracic echocar-diography associated with a multiplane transesophageal study is the best examination to establish the diagnosis 10,14.
Due to their potential of systemic embolization, these lesions should always be excised, despite their benign his-tological appearance and small dimension. Reports exist that even lesions of 3mm may account for cerebral emboliza-tion, and should, therefore, be surgically removed in asympto-matic patients, who do not have surgical contraindication 10.
Despite their uncertain evolution, a review of a large case series 8 showed that only 4 patients were free from
symp-toms when the fibroelastoma was discovered. Procedures preserving the valve are recommended in most cases 8.
Re-currence has not been reported; long-term follow-up, howe-ver, is recommended.
The last item to be discussed is the association with the possible ticlopidine-induced granulocytopenia, which our patient had. Important blood dyscrasias, such as thrombocytopenic purpura, aplastic anemia, and granulocytopenia, related to the use of this drug have been reported 18-20. Even though the cause of bone
marrow aggression remains uncertain, direct and im-munological toxic mechanisms have been proposed 18.
Side effects associated with ticlopidine have been re-ported after implantation of coronary stents with a mean 4-week treatment with this drug, the higher frequency of events occurring after 14 days of treatment 18. Drug
withdrawal in selected cases is able to normalize the he-matological disorder. Clopidogrel, an alternative to ti-clopidine due to its similar antiplatelet activity, has also been shown to be safer in regard to its side effects 21,22.