Paulo FrazãoI
Marco A PeresII
Jaime A CuryIII
I Departamento de Prática de Saúde Pública. Faculdade de Saúde Pública. Universidade de São Paulo. São Paulo, SP, Brasil
II Departamento de Saúde Pública. Centro de Ciências da Saúde. Universidade Federal de Santa Catarina. Florianópolis, SC, Brasil
III Departamento de Ciências Fisiológicas. Faculdade de Odontologia de Piracicaba. Universidade Estadual de Campinas, Piracicaba, SP, Brasil
Correspondence: Paulo Frazão
Faculdade de Saúde Pública Universidade de São Paulo Av. Dr. Arnaldo, 715 Cerqueira Cesar
01246-904 São Paulo, SP, Brasil E-mail: [email protected] Received: 8/26/2010 Approved: 1/19/2011
Article available from: www.scielo.br/rsp
Drinking water quality and
fl uoride concentration
ABSTRACT
This paper aimed to analyze the fl uoride concentration in drinking water, taking into account the balance between the benefi ts and risks to health, in order to produce scientifi c backing for the updating of the Brazilian legislation. Systematic reviews studies, offi cial documents and meteorological data were examined. The temperatures in Brazilian state capitals indicate that fl uoride levels should be between 0.6 and 0.9 mg F/l in order to prevent dental caries. Natural fl uoride concentration of 1.5 mg F/l is tolerated for consumption in Brazil if there is no technology with an acceptable cost-benefi t ratio for adjusting/removing the excess. Daily intake of water with a fl uoride concentration > 0.9 mg F/l presents a risk to the dentition among children under the age of eight years, and consumers should be explicitly informed of this risk. In view of the expansion of the Brazilian water fl uoridation program to regions with a typically tropical climate, Ordinance 635/75 relating to fl uoride added to the public water supply should be revised.
DESCRIPTORS: Potable Water. Fluoridation. Water Quality. Review. Dental fl uorosis.
INTRODUCTION
Water is a public asset that is indispensable for life. Its importance for public health is widely recognized, but more than one billion people worldwide do not have access to treated water. Among these people, 19 million live in Brazil.26
Observational studies in the United States in the fi rst half of the 20th century revealed an inverse correlation between the fl uoride content in the water supply and the mean number of decayed teeth among the population. However, it was found that above a certain concentration, the occurrence of caries ceased to signifi cantly diminish, while the prevalence of dental fl uorosis increased signifi cantly. This series of studies was essential for estimating the optimum
fl uoride level that would provide the maximum benefi t of reduction in caries with the minimum risk of dental fl uorosis and for consequently adopting water
fl uoridation as a public health measure.3
Fluoridation of the water in treatment plants has been obligatory in Brazil since 1974, as set forth in Federal Law 6050.a In 1975, Ordinance 635 estab-lished standards for implementing this measure,b which included the recom-mended limits for fl uoride concentration as a ratio of the mean maximum daily
a Brasil. Lei Federal nº 6.050, de 24/05/1974. In: Coleção das Leis de 1974: Atos do Poder Legislativo: leis de abril a junho. Brasília, DF: Departamento de Imprensa Nacional; 1974. v.3, p.107.
b Ministério da Saúde. Portaria 635 de 26 de dezembro de 1975. Aprova normas e padrões sobre a fl uoretação da água de sistemas públicos de abastecimento. Diario Ofi cial Uniao.
temperature. Since then, the coverage of water fl uorida-tion has increased, and it reached approximately half of the country’s population in the fi rst decade of the 21st century. Water fl uoridation has been supported not only through resolutions approved at health and oral health conferences but also by the Brazilian Ministry of Health and by the main professional entities in Brazil within the fi elds of dentistry and public health.21
In 1988, fl uoride was added to a brand of toothpaste widely used in Brazil, and by 1989, more than 90% of the products available to consumers were fl uoridated.8 The use of fl uoride in the water and in toothpaste has been responsible for a signifi cant decline in the levels of dental caries among children and adolescents in Brazil and has been heralded as an important change that may confer a different oral health pattern from that of the present for the coming generations.
Two years after the approval of the federal law relating to fluoridation, the Ministry of Health approved drinking water standards and criteria through Ordinance 56/1977.c Given the presence of both added and natu-rally occurring fl uoride in water for human consump-tion, 1.7 mg F/l was set as the maximum permitted amount. This concentration was subsequently changed in 2000,d with the publication of Ordinance 1469, which defi ned 1.5 mg F/l as the maximum permitted amount. This guidance was maintained in Ordinance 518.e In 2009, the Ministry of Health instituted a working group with the aim of reviewing this ordinance.
Fluoride concentration is an important parameter for the quality assessment of drinking water because of its ability to prevent caries when fl uoride is present at appropriate levels, and for its potential to provoke dental fl uorosis when present at high levels. The estab-lishment of safety levels for fl uoride in drinking water is an essential measure for protecting human health.
The aim of this review was to analyze the potability of drinking water with regard to fl uoride levels within the Brazilian context, while taking into consideration the balance between benefi ts and risks to health. In addi-tion, supporting data were produced with consideration to revision of the national legislation.
METHODOLOGICAL PROCEDURES
To select the material for analysis, we consulted the database of the University of York Centre for Reviews
c Ministério da Saúde. Portaria nº 56/Bsb, de 14 de março de 1977. Aprova normas e o padrão de potabilidade da água a serem observados em todo o território nacional. Diario Ofi cial Uniao. 22 mar. 1977.
d Ministério da Saúde. Portaria 1.469, de 29 dez. 2000. Estabelece os procedimentos e responsabilidades relativos ao controle e vigilância da qualidade da água para consumo humano e seu padrão de potabilidade, e dá outras providências. Diario Ofi cial Uniao. 19 jan 2001; Seção 1:18-22.
e Ministério da Saúde. Portaria 518, de 25 de março de 2004. Estabelece os procedimentos e responsabilidades relativas ao controle e vigilância da qualidade da água para o consumo humano e seu padrão de potabilidade, e dá outras providências. Diario Ofi cial Uniao 16 mar 2004; Seção 1:266-70.
f Australian Government. National Health and Medical Research Council. A systematic review of the effi cacy and safety of fl uoridation. Part A: review of methodology and results. Australian Government, 2007.
and Dissemination, part of the National Institute for Health Research of the United Kingdom, which provides backing for decision makers. This database is updated daily and, among other information, includes studies indexed in PubMed/MEDLINE and those produced by important systematic review centers. The term “fl uoride” was searched. Systematic reviews on the benefi ts and risks of fl uoridated water for denti-tion and for bone health published between the years 2000 and 2009 were included. From this search, 77 systematic review studies were found, of which fi ve covered the questions of interest. Two of them had the aim of investigating possible adverse effects.18,31 The other three dealt with the effects of fl uoride on bone health.13,10,33 In addition, a systematic review commis-sioned by the Australian government on the effi cacy and safety of water fl uoridation was included.f
To determine the optimum fluoride levels in the Brazilian Federal District and state capitals, latitude, longitude, altitude and 2008 temperature data were obtained from the National Institute of Meteorology.
In addition, the electronic sites of government agen-cies and offi cial documents relating to this topic were consulted.
The results from the analysis focused on three issues: the benefi ts of fl uoride in the water, its risks and the standards adopted in different countries.
BENEFITS OF FLUORIDE IN THE WATER
Over the last decades of the 20th century, declines in tooth decay among child populations were described in several developed countries. The expansion of fl uoride use was taken to be the most important cause of this epidemiological event, which was unprecedented.
Fluoride is widely used as a public health measure worldwide. In some countries, widespread use of fl uo-ridated toothpaste is the only population-based strategy for preventing caries. Nonetheless, selecting the best option for ensuring access to fl uoride in public health strategy terms depends on the prevalence and distribu-tion of dental caries along with mobility, educadistribu-tional attainment, economic level and acceptability among the population.
The use of fl uoride as a preventive and therapeutic measure for caries began in 1945 and 1946 in the US and Canada with four pioneering studies that had the main aim of investigating the effectiveness of this measure.3 In 1951, water fl uoridation became an offi cial policy in the US. In 1960, approximately 50 million people in the US were benefi ting from this measure, and by 2006, it had reached nearly 60% of the population of that country. This measure has been considered to be one of ten most important public health achievements of the 20th century.5
In the United Kingdom, the implementation of this measure began in 1960.1 In New Zealand, approxi-mately 65% of the population had received the benefi t by 1968.23 In the Republic of Ireland, by 1996, 66% of the population benefi ted from this measure.23
The fl uoridation of drinking water has been recom-mended by the World Health Organization (WHO), among other important worldwide entities within the fi eld of healthcare. In 1986, at an international conference on “Appropriate Use of Fluorides,” water
fl uoridation was highlighted as an effective, safe and cheap intervention that should be implemented and maintained wherever it is possible.35
In Brazil, fl uoridation in treating the water supply began in 1953 in the municipality of Baixo Guandu. Comparisons of caries rates among schoolchildren aged 6 to 14 years between 1953 and 1963 showed results similar to those observed in the US and Canada. A study conducted in Barretos, Southern Brazil, on a similar population, confi rmed the fi ndings from Baixo Guandu.25 After the federal law on fl uoridation was enacted, use of this measure expanded enormously in the 1980s. By 2006, the benefi ts of fl uoridation had reached approximately 100 million people. Brazil presented a notable reduction in caries experience between 1986 and 2003. The caries rate – mean DMFT - at 12 years of age went down from 6.7 to 2.8 affected teeth.22 Data from 2003 showed that children and adolescents living in cities with water fl uoridation exhibited caries levels approximately one third lower than those living in cities without this benefi t.g
Among nearly 60 countries that adopted water fl uo-ridation as a method for preventing and controlling dental caries, the following countries with the highest coverage can be highlighted: Hong Kong (100%), Singapore (100%), Israel (75%), Colombia (70%), Malaysia (approximately 70%), Ireland (66%), Australia (61%), US (61%), New Zealand (61%), Brunei (56%), Brazil (approximately 50%), Canada (43%) and Chile (40%). At the start of the 21st century, fl uoridation was benefi ting approximately 400 million people.1
One of the reviews consulted18 included two prospective cohort studies, one retrospective cohort study and 23 others that compared caries rates before and after water
fl uoridation. The results from the studies indicated that water fl uoridation was effective in preventing caries and was statistically associated with i) a lower proportion of children with tooth decay, with the median of the mean difference in proportions at 14.6% and ii) lower numbers of teeth that were decayed, missing and fi lled because of caries, equivalent to 40% prevention of new caries. The effect of the water fl uoridation was evident, even if it is assumed that other sources of fl uoride use were present, such as fl uoridated toothpaste. Moreover, if fl uoridation was halted, the differences in caries outcomes between regions with and without fl uorida-tion became smaller.18
A review published in the US31 included eight cross-sectional studies, one non-randomized clinical trial, eight prospective studies and one time series study. The results indicated i) a mean reduction of between 30% and 50% in the caries experience among individuals living in regions with fl uoridated water, as compared with people living in regions without this measure and ii) that halting of fl uoridation gave rise to a 17.9% increase in the experience of caries.
The Australian reviewf took into consideration the previous published papers and added one study conducted in Finland.28 However, inclusion of this study did not modify the conclusions regarding the reduction in caries prevalence resulting from water fl uoridation.
Based on these data, it can be concluded that water
fl uoridation is an effective measure for preventing and controlling dental caries in children and adolescents.
RISKS OF FLUORIDE IN THE WATER
One of the reviews consulted assessed the negative effects of water fl uoridation that have been documented in the scientifi c literature.18 The main association found at levels of less than 4.0 mg F/l was with dental fl uo-rosis. This is a disorder of enamel development that occurs during tooth formation and is characterized by
hypomineralization and greater porosity of the region immediately below the surface of the tooth enamel. At
fl uoride concentrations of more than 1.0 mg/l in the water supply, opaque areas start to become visible on the enamel surface.27
These opacities are symmetrical because the teeth formed at the same time have the same abnormality. Nonetheless, enamel opacities of non-fl uorotic origin that can be manifested symmetrically also exist.7 While non-fluorotic opacities are rounded and delimited (Figure 1), fl uorotic opacities are diffused and trans-versed (Figure 2).
The effect of fl uoride on tooth enamel is dose-depen-dent. In other words, whenever there is fl uoride intake during enamel formation, there will be a certain level of fl uorosis. However, the clinical signifi cance of fl uo-rosis provoked will depend on the various sources to which individuals are exposed and the time for which this exposure lasts.
As the fl uoride dose to which children are exposed increases, the opacities become ever more visible, which may characterize a more severe degree of dental
fl uorosis. Figure 3 presents a case of severe fl uorosis caused by well water containing 3.6 mg F/l, i.e., an amount fi ve times greater than the optimum concentra-tion level for the Brazilian climate.
The critical period for exposure to excessive doses of
fl uoride to the two dentitions is from birth up to the age of 8 years.17
Given the expected effects from water fl uoridation and in the light of the high prevalence rates and severity of dental caries in the 1950s, esthetically acceptable related dental fl uorosis resulting from water fl uoridation was considered to be the price to be paid for the benefi t of caries prevention.
However, it was recognized that this value could vary according to the daily intake of water. Subsequently, it was shown that children living in hotter regions had less caries and more fl uorosis compared to children living in colder regions with the same fl uoride level in the drinking water.12
For this reason, a method for determining the optimum
fl uoride level in the water supply, taking into consider-ation the effect of mean maximum daily temperatures on the water consumed by children, was formulated. Thus, a range of optimum fl uoride concentrations (0.7 to 1.2 mg F/l) was established according to the temperature in different regions of the US (Figure 4), which ranged from 10.9 °C (51.7 °F) to 29.6 °C (85.3 °F).12 Thus, the specifi c optimum fl uoride level for each region came to be defi ned through a mathematical formula that took into account fl uid intake and the ambient temperature.
Adverse dental effects caused by prolonged intake of high levels of naturally occurring fl uoride in the water
Note: When the stains cover between 25% and 50% of the surface, they constitute mild dental fl uorosis (without esthetic or functional signifi cance).
Photo: Prof. Dra. Maria da Luz Rosário de Sousa (FOP-UNICAMP)
Figure 2. Diffuse and transverse stains caused by fl uorotic opacity.
Photo: Prof. Dr. Jaime Cury (FOP-UNICAMP)
Figure 3. Severe dental fl uorosis (with esthetic and functional signifi cance) in a child who had been exposed to water con-taining 3.6 ppm of naturally occurring fl uoride.
Figure 1. Rounded and delimited stains caused by non-fl uorotic opacity.
are also known in Brazil. Tooth enamel defects in schoolchildren exposed to high levels of fl uoride have been documented in Pereira Barreto, Southeastern Brazil, and in Cocal do Sul, Southern Brazil.4,32 Through prohibiting the use of these water sources, the multiple cases of fl uorosis found ceased to occur.
Only some of the cases of dental fl uorosis presented esthetic problems. McDonagh et al.18 reviewed 88
studies that met the inclusion criteria and separated the effects resulting from any degree of dental fl uorosis from the effects associated with fl uorosis of esthetic signifi cance. The prevalence of fl uorosis of esthetic signifi cance was estimated to be 10.0% (95% CI: 5.0; 17.9) and 12.5% (95% CI: 7.0; 21.5) for 0.7 and 1.0 mg F/l, respectively. Regression analyses showed a strong association between the fl uoride level and the propor-tion of the populapropor-tion with any degree of fl uorosis. The effect of exposure to different concentrations of
fl uoride in the water compared with areas of up to 0.4 mg F/l was estimated, and a difference of 15% (95% CI: 4.1; 27.2) was found in areas with 1.0 mg F/l, and a difference of 18.9% (95% CI: 7.2; 30.6) was found in areas with 1.2 mg F/l.
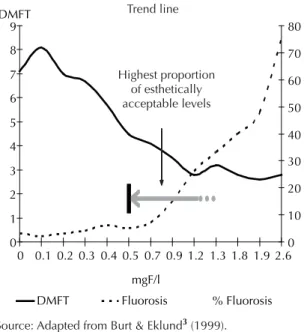
It can be concluded that the proportion of fl uorosis levels of esthetic signifi cance in children and adoles-cents diminishes as the fl uoride concentration in the water comes closer to the range of 0.5 to 0.7 mg F/l. This trend corresponds to a greater proportion of fl uorosis without esthetic impairment and signifi es a safe level of
fl uoride, either in water containing naturally occurring
fl uoride or in artifi cially fl uoridated water (Figure 5).
A review of the literature on esthetic perceptions and dental fl uorosis showed that very mild and mild degrees of dental fl uorosis did not produce any negative impact on quality of life among the populations investigated.6 In Brazil, studies in areas with optimum levels of
fl uoride in the water have not shown any impact of dissatisfaction with the appearance of the teeth.19,20 An investigation among adolescents in Pelotas, Southern Brazil (with water fl uoridated since 1962 and most cases of fl uorosis in the very mild and mild categories) showed a positive association between dental fl uorosis and more favorable quality-of-life scores.24
Bottled water may also carry a risk of fl uorosis. In the United Kingdom, the levels of fl uoride in 12 types of bottled water ranged from 0.1 to 0.8 mg F/l.30 In the Brazilian market, levels higher than 0.7 mg F/l were noted in 10.6% of 104 commercial brands of mineral water,34 indicating a need for greater control over manufactured mineral water products.
Occurrences of cancer and bone fractures were not associated with water fl uoridation.18 Skeletal fl uorosis has been observed in areas with fl uoride concentra-tions greater than 5.6 mg F/l.7 Systematic reviews have shown that i) medical prescriptions of supplements containing fl uoride may increase the bone mineral density of the hip and spine, depending on the duration of use; no evidence was observed in relation to the risk of hip or spine fracture and low doses of fl uoride (20 mg per day or less) were associated with signifi cant reduc-tions in the risk of fracture;33 ii) although fl uoride is capable of increasing the bone mineral density (BMD) of the lumbar spine, it does not cause any reduction
0 1 2 3 4 5 6 7 8 9
0 0.1 0.2 0.3 0.4 0.5 0.7 0.9 1.2 1.3 1.8 1.9 2.6
mgF/l DMFT 0 10 20 30 40 50 60 70 80 % Fluorosis DMFT Fluorosis
Interval of optimum concentration levels according
to the mean maximum daily temperatures in different regions of the US
Figure 4. Caries experience (DMFT-Decayed, Missing and Filled teeth) and dental fl uorosis in adolescents aged 12 to 14 years, according to fl uoride concentration in the water. US, 1930. Trend line.
Source: Adapted from Burt & Eklund3 (1999)
Figure 5. Caries experience (DMFT-Decayed, Missing and Filled teeth) and dental fl uorosis in adolescents aged 12 to 14 years, according to fl uoride concentration in the water. US, 1930. 0 1 2 3 4 5 6 7 8 9
0 0.1 0.2 0.3 0.4 0.5 0.7 0.9 1.2 1.3 1.8 1.9 2.6
mgF/l DMFT 0 10 20 30 40 50 60 70 80 % Fluorosis DMFT Fluorosis Highest proportion of esthetically acceptable levels
Source: Adapted from Burt & Eklund3 (1999).
in occurrences of vertebral fractures; increases in the
fl uoride dose may result in a greater risk of non-spinal fractures and adverse gastrointestinal effects, without any effect on the spinal fracture rate;13 and iii) up to 1.0 mg F/l, there is no adverse effect regarding bone resistance, BMD and fracture incidence.10
Thus, a high fl uoride concentration in water represents a risk of dental fl uorosis for children with dental enamel at the formation stage. The severity of the effect for the population is related to the concentration present in the water. A 15% difference (95% CI: 4.1; 27.2) in the prevalence of functionally signifi cant fl uorosis was found
when comparing areas with 1.0 mg F/l and 0.4 mg F/l in studies mainly involving temperate-climate countries.18
WATER POTABILITY AND FLUORIDE CONCENTRATION
Several countries have specific recommendations relating to the fl uoride parameter. In South America, most countries have taken 1.5 mg F/l as the maximum permitted amount.h In the US, the Environmental Protection Agency has defined 4.0 mg F/l as the maximum concentration level for fl uoride in public water supply systems and as the potability standard. Table. Geographical coordinates of the meteorological stations, annual mean maximum daily temperatures (ºCelsius) and recommended optimum fl uoride content (mg/l). Brazil, 2008.
Cities Latitude (S) Longitude(W) Altitude
(meters)
Annual mean maximum daily temperature
Optimum content (mg F/l)
Aracaju 10º57’ 37º03’ 4.72 29.8 0.696
Belém 01º26’ 48º26’ 10.00 31.9 0.664
Belo Horizonte 19º56’ 43º56’ 915.00 27.3 0.737
Boa Vistaa 02º49’ 60º39’ 90.00 33.8 0.638
Brasília (DF) 15º47’ 47º56’ 1159.54 27.0 0.744
Campo Grande 20º27’ 54º37’ 530.73 29.4 0.702
Cuiabá 15°33’ 56º07’ 151.34 32.5 0.655
Curitiba 25º26’ 49º16’ 923.50 23.3 0.817
Florianópolis 27º35’ 48º34’ 1.84 24.9 0.783
Fortaleza 03º45’ 38º33’ 26.45 31.1 0.676
Goiânia 16º40’ 49º15’ 741.48 31.3 0.673
João Pessoa 07º06’ 34º52’ 7.43 30.0 0.692
Macapá 00º03’ 51º07’ 14.46 31.8 0.665
Maceió 09º40’ 35º42’ 64.50 31.0 0.678
Manaus 03º07’ 59º57’ 67.00 32.1 0.662
Natal 05º55’ 35º12’ 48.60 29.8 0.695
Palmas 10º11’ 48º18’ 280.00 33.6 0.640
Porto Alegre 30º03’ 51º10’ 46.97 25.0 0.780
Porto Velho 08º46´ 63º 55’ 95.00 30.8 0.680
Recife 08º03’ 34º57’ 10.00 29.6 0.699
Rio Branco 09º58’ 67º48’ 160.00 30.9 0.679
Rio de Janeiro 22º53’ 43º11’ 11.10 29.8 0.696
Salvador 13º00’ 38º30’ 51.41 29.4 0.703
São Luís 02º32’ 44º13’ 50.86 31.1 0.676
São Paulo 23º30’ 46º37’ 792.06 25.6 0.769
Teresina 05º05’ 42º49’ 74.36 33.8 0.638
Vitória 20º19’ 40º19’ 36.20 28.9 0.710
Source: National Institute of Meteorology
a Boa Vista: Latitude North.
h Pinto VG. Análise comparativa de legislações relativas à qualidade da água para consumo humano na América do Sul [master’s dissertation]. Belo Horizonte: Universidade Federal de Minas Gerais; 2006.
However, there is a specific recommendation to adopt a limit of 2.0 mg F/l to reduce the risk of dental
fl uorosis.i In Canada, water fl uoridation decisions are made by each municipality. The Federal Commission on Fluoridation recommends an optimum concentration of between 0.8 and 1.0 mg F/l. The Canadian government recommends an amount of 1.5 mg F/l as the maximum acceptable concentration.j In European countries, the maximum permitted fl uoride concentration in the water supply is 1.5 mg F/l. Ireland has adopted specifi c legis-lation that is more restrictive than the European law, limiting the concentration in the water supply to 1.0 mg F/l.k In Australia, up to 1.5 mg F/l is accepted when it occurs naturally.l In Asia, Hong Kong has reduced its optimum levels of fl uoride added to the water supply over recent years. Until 1978, the optimum level was 1.0 mg F/l, when it was reduced to 0.7 mg F/l.11 In 1988, the level was reduced to 0.5 mg F/l.15 It needs to be highlighted that the mean maximum daily temperature in the Hong Kong region is 24.7 °C.
In 1984, WHO defi ned 1.5 mg F/l as the limit for safe potable water. This amount was reassessed in the latest review37 but was not adjusted due to the lack of reason-able evidence. However, the WHO did emphasize that this amount should not be fi xed and it would dependent on the specifi c context.
In Brazil, the fi rst federal standard was published in 1977, and the level of 1.7 mg F/l was adopted as the criterion for the water potability standard. Currently, the level of 1.5 mg F/l is used as the maximum permitted amount throughout the national territory.d This level was established based on technical reports from WHO, which served as the reference for many countries, inde-pendent of their climatic conditions. It is emphasized in the standard that “the recommended levels for the
fl uoride ion concentration should follow the specifi c legislation in force relating to water fl uoridation, while in any case the maximum permitted amount of this Table shall be respected”.d
This text may lead to the interpretation that the expres-sion “in any case” refers both to naturally occurring
fl uoride and fl uoride added to the water for the purpose of dental caries prevention, which is not justifi ed in the context of the presented knowledge. Thus, the maximum permitted amount for fl uoride naturally present in water cannot be used as the limit for fl uoride added during water treatment.
It has been suggested that the optimum fl uoride concen-tration in water should be established by taking into account not the air temperature but the dose to which children are exposed (mg F/day/kg of body weight). Thus, Burt2 suggested in 1992 that a daily dose of 0.07 mg F per kg of body weight should be taken as the upper limit, so that the resultant fl uorosis would not compro-mise the anti-caries benefi ts from fl uoride intake among children within the at-risk age group. However, this limit should be validated by data from a longitudinal dose-effect study, and no association between the dose and the resultant fl uorosis has been found16, requiring more studies about a safety dose.
Based on the mean maximum daily temperatures recorded in Brazilian state capitals only for 2008 (Table), it is possible to calculate the optimum fl uoride concentration levels in accordance with the formula recommended in Ordinance 635/75. This calcula-tion shows a range from approximately 0.6 mg F/l in Boa Vista, Northern Brazil, to 0.8 mg F/l in Curitiba, Southern Brazil. Although records of daily air tempera-tures do not exist for all Brazilian municipalities, it can be seen from the temperature characteristics in the different regions that the appropriate fl uoride levels recommended for most Brazilian municipalities will be around this band (Table).
From consultations in the electronic databases of state and municipal legislation, two states showed comple-mentary legislation. In the State of São Paulo, Resolution SS-65/2005 establishes that the water should contain 0.7 mg F/l, with acceptable variation from 0.6 to 0.8 mg F/l.m In the State of Rio Grande do Sul, Ordinance SSMA 10/99 establishes that the ideal fl uoride concentration in water for human consumption is 0.8 mg F/l, with acceptable variation from 0.6 to 0.9 mg F/l.n
Galagan and Vermillion12 made an important contri-bution towards applying the method through their proposed formula for determining the optimum fl uo-ride level, which considered the correlation between
fl uid intake and the mean air temperature. It should be emphasized that the optimum concentration was calcu-lated based on temperature variations in the US, which has a temperate climate. Hence, their formula may not be applicable to regions with a tropical climate, for which a level of 0.5 mg F/l might be considered appro-priate.36 In the case of Brazil, this is not a concern for the
j Health Canada. Fluoride and human health: it is your health. Ottawa; 2008 [cited 2010 Apr 5]. Available from: http://www.hc-sc.gc.ca/hl-vs/ alt_formats/pacrb-dgapcr/pdf/iyh-vsv/environ/fl uor-eng.pdf
k The Council of The European Union. European Union legislation: Council Directive 98/83/EC (OJ L330, p32, 5/12/1998) of 3 November 1998 on the quality of water intended for human consumption [cited 2011 Apr 10]. Available from: http://www.fsai.ie/uploadedFiles/ Legislation/Food_Legisation_Links/Water/Council_Directive_98_83_EC.pdf
l Australian Government, National Health and Medical Research Council. Australian drinking water guidelines 6. Canberra; 2004 [cited 2010 Apr 5]. Available from: http://www.nhmrc.gov.au/_fi les_nhmrc/fi le/publications/synopses/adwg_11_06.pdf
southern and southeastern regions, where the climate is predominantly subtropical,14 but it may be so for cities in the northern, northeastern and central-western regions, which have genuinely tropical climates.
FINAL REMARKS
Based on the information reviewed here, most countries have adopted the level of 1.5 mg F/l as the maximum permitted amount for naturally occurring fluoride; Ireland, located to the north of the Tropic of Cancer, and Hong Kong, located to the south of it, constitute exceptions. In Australia, a country with climatic variation similar to that of Brazil, the maximum permitted amount of 1.5 mg/l is explicitly adopted for naturally occurring
fl uoride, and 1.0 mg F/l for areas where fl uoride is added.l
In Brazil, the optimum fl uoride levels in treated water (with the maximum anti-caries benefi t and minimum risk of functionally signifi cant dental fl uorosis) for the state capitals and Federal District ranged from 0.6 to 0.8 mg F/l. For some cities in the south of the country, up to 0.9 mg F/l is accepted. As long as other sources of drinking water or technologies of acceptable cost for adjusting or removing fl uoride from water remain unavailable, the maximum permitted amount of 1.5 mg F/l can be accepted as a tolerable level in water for human consumption in which the occurrence of
fl uoride is natural.
However, in compliance with Federal Decree 5440/2005,o when the naturally occurring fl uoride concentration is more than 0.9 mg F/l, the entities responsible for the systems and alternative public water supply solutions must furnish the following information to consumers: “This water should not be consumed daily by children under the age of eight years”, in conformity with the current legislation.
The percentage of the Brazilian population supplied with naturally fl uoridated water is unknown, but a study covering 74% of the municipalities of the State of Piauí (Northeastern Brazil) showed that although the concentration was low in 151 of them (< 0.3 ppm F),
13 had levels of 0.31 to 0.59 mg F/l.29 Only one- third of the municipal sanitation services performed raw water analyses, and such analyses were more common on water from surface catchment areas than on under-ground aquifers.p Although the data available do not allow a panorama for the Brazilian population to be outlined, it is estimated that there are few localities in the country where naturally occurring fl uoride reaches concentrations of 1.0 to 1.5 mg F/l.
The obligation to provide information to the public stimulates public authorities at all levels of government (federal, state and municipal), sanitation companies and other interested parties to ensure that the naturally occurring fl uoride concentrations are close to optimum levels. This changing may occur over the medium to long term, depending on local measures, but in many cases, measures of greater complexity will be needed. These measures will involve agreements between different spheres of government and the sanitation companies. This process, through specifi c legislation, will constitute important support leading towards reviewing and defi ning the quality standards for mineral water commercialized in Brazil.
In relation to fl uoride added to water, greater knowl-edge about the climatic conditions of different regions of Brazil justifi es the need to review Ordinance 635, which was approved in 1975, in view of the expansion of the national program for water fl uoridation to places with a typically tropical climate.
ACKNOWLEDGEMENTS
We extend our appreciation to the National Coordination Offi ce for Oral Health and the Health Surveillance Department of the Ministry of Health, the National Institute of Meteorology and the Ministry of Health’s Collaborative Center for Oral Health Surveillance at the School of Public Health, University of São Paulo, for their support. We thank Prof. Dra. Lívia Tenuta and Prof. Dra. Maria da Luz Rosário de Sousa, both from Universidade Estadual de Campinas, for the images provided.
o Presidência da República. Casa Civil. Decreto nº 5.440 de 4 de maio de 2005. Estabelece defi nições e procedimentos sobre o controle de qualidade da água de sistemas de abastecimento e institui mecanismos e instrumentos para divulgação de informação ao consumidor sobre a qualidade da água para consumo humano [cited 2006 Apr 3]. Available from: http://www.planalto.gov.br/ccivil_03/_Ato2004-2006/2005/ Decreto/D5440.htm
1. British Fluoridation Society; The UK Public Health Association; The British Dental Association; The Faculty of Public Health. One in a million: the facts about water fl uoridation. 2.ed. Manchester: British Fluoridation Society; 2004. Chapter 7, The extent of water fl uoridation; p.55-80.
2. Burt BA. The changing patterns of systemic fl uoride
intake. J Dent Res. 1992;71(5):1228-37. DOI:10.1177/
00220345920710051601
3. Burt BA, Eklund SA. Dentistry, dental practice and the community. 5. ed. Philadelphia: WB Saunders; 1999.
4. Capella LF, Carcereri, DL, Paiva SM, Rosso RA, Paixão RF, Saltori EK, et al. Ocorrência de fl uorose dentária
endêmica. RGO (Porto Alegre). 1989;37(5):371-5.
5. Centers for Disease Control and Prevention. Achievements in public Health, 1900-1999:
fl uoridation of drinking water to prevent dental caries.
MMWRMorb Mortal Wkly Rep. 1999;48(41):933-40.
6. Chankanka O, Levy SM, Warren JJ, Chalmers JM. A literature review of aesthetic perceptions of dental fl uorosis and relationships with psychosocial aspects/
oral health-related quality of life. Community Dent
Oral Epidemiol.2010;38(2):97-109. DOI:10.1111/ j.1600-0528.2009.00507.x
7. Cury JA. Uso do fl úor e controle da cárie como doença. In: Baratieri LN, Monteiro Junior S, Andrada MAC, Vieira LCC, Ritter AV, Cardoso AC. Odontologia restauradora: fundamentos e possibilidades. São Paulo: Editora Santos; 2002. p.31-68.
8. Cury JA, Tabchoury CPM. Determination of appropriate exposure to fl uoride in non-EME countries in the
future. J Appl Oral Sci. 2003;11(2):83-95.
9. Cury JA, Tenuta LM. How to maintain a cariostatic fl uoride concentration in the oral
environment. Adv Dent Res. 2008;20(1):13-6.
DOI:10.1177/154407370802000104
10. Demos LL, Kazda H, Cicuttini FM, Sinclair MI, Fairley CK. Water fl uoridation, osteoporosis, fractures: recent
developments. Aust Dent J. 2001;46(2):80-7.
11. Evans RW, Lo ECM, Lind OP. Changes in dental health in Hong Kong after 25 years of water fl uoridation.
Community Dent Health.1987;4(4):383-94.
12. Galagan DJ, Vermillion JR. Determining optimum
fl uoride concentrations. Public Health Rep.
1957;72(6):491-3.
13. Haguenauer D, Shea B, Tugwell P, Wells GA, Welch V. Fluoride for treating postmenopausal osteoporosis.
Cochrane Database Syst Rev. 2000;(4):CD002825. DOI:10.1002/14651858.CD002825
14. Lima YBO, Cury JA. Ingestão de fl úor por crianças pela
água e dentifrício. Rev Saude Publica.
2001;35(6):576-81. DOI:10.1590/S0034-89102001000600012
15. Lo ECM, Wong AHH. Water fl uoride concentration and
fl uorosis in Hong Kong in 1960-2001 [abstract]. J Dent
Res. 2006;85 Suppl B:a2440.
16. Martins CC, Paiva SM, Lima-Arsati YB, Ramos-Jorge ML, Cury JA. Prospective study of the association between fl uoride intake and dental fl uorosis in
permanent teeth. Caries Res. 2008;42(2):125-33.
DOI:10.1159/000119520
17. Mascarenhas AK. Risk factors for dental fl uorosis:
a review of the recent literature. Pediatr Dent.
2000;22(4):269-77.
18. McDonagh M, Whiting P, Bradley M, Cooper J, Sutton A, Chestnutt I, et al. A systematic review of public water
fl uoridation. New York: NHS Centre for Reviews and
Dissemination, University of York; 2000. (Report 18).
19. Menezes LMB, Sousa MLR, Rodrigues LKA, Cury JA. Autopercepção da fl uorose pela exposição a fl úor pela
água e dentifrício. Rev Saude Publica.
2002;36(6):752-4. DOI:10.1590/S0034-89102002000700015
20. Michel-Crosato E, Biazevic MGH, Crosato E. Relationship between dental fl uorosis and quality
of life: a population based study. Braz Oral Res.
2005;19(2):150-5. DOI:/S1806-83242005000200014
21. Narvai PC. Cárie dentária e fl úor: uma relação do
século XX. Cienc Saude Coletiva. 2000;5(2):381-92.
DOI:10.1590/S1413-81232000000200011
22. Narvai PC, Frazão P, Roncalli AG, Antunes JLF. Cárie dentária no Brasil: declínio, polarização,
iniquidade e exclusão social. Rev Panam Salud
Publica. 2006;19(6):385-93. DOI:10.1590/S1020-49892006000600004
23. Nunn JF, Steele JG. Fluorides and dental caries. In: Murray JJ, Nunn JH, Steele JG, editors. Prevention of oral disease. 4.ed. London: Oxford University Press; 2003. p.35-60.
24. Peres KG, Peres MA, Araújo CLP, Menezes AMB, Hallal PC. Social and dental status along the life course and oral health impacts in adolescents: a population-based
birth cohort. Health Qual Life Outcomes. 2009;7:95.
DOI:10.1186/1477-7525-7-95.
25. Pinto VG. Saúde bucal coletiva. 4.ed. São Paulo: Editora Santos; 2001.
26. Rheingans R, Dreibelbis R, Freeman MC. Beyond the Millennium Development Goals: public health
challenges in water and sanitation. Glob Public Health.
2006;1(1):31-48. DOI:10.1080/17441690500443139
27. Robinson C, Connell S, Kirkham J, Brookes SJ, Shore RC, Smith AM. The effect of fl uoride on the
developing tooth. Caries Res. 2004;38(3):268-76.
DOI:10.1159/000077766
28. Seppä L, Kärkkäinen S, Hausen H. Caries trends 1992-1998 in two low-fl uoride Finnish towns formerly with
and without fl uoridation. Caries Res. 2000;34(6):462-8.
DOI:10.1159/000016624
29. Silva JS, Moreno WG, Forte FDS, Sampaio FC. Natural fl uoride levels from public water supplies in Piauí
State, Brazil. Cienc Saude Coletiva.
2009;14(6):2215-20. DOI:10.1590/S1413-81232009000600030
30. Toumba KJ, Levy S, Curzon MEJ. The fl uoride content
of bottled drinking waters. Br Dent J. 1994;176:266-8.
31. Truman BI, Gooch BF, Sulemana I, Gify HC, Horowitz AM, Evans CA, et al. Reviews of evidence on interventions to prevent dental caries, oral and pharyngeal cancers, and sports-related craniofacial
injuries. Am J Prev Med. 2002;23 (1 Suppl):21-54.
32. Uchôa HW, Saliba NA. Prevalência de fl uorose dental
na cidade de Pereira Barreto. Bol Serv Odontol Sanit.
1970;6(3):11-6.
33. Vestergaard P, Jorgensen NR, Schwarz P, Mosekilde L. Effects of treatment with fl uoride on bone mineral
density and fracture risk: a meta-analysis. Osteoporosis
Int. 2008;19(3):257-68.
DOI:10.1007/s00198-007-0437-6
34. Villena RS, Borges DG, Cury JA. Avaliação da concentração de fl úor de águas minerais
comercializadas no Brasil. Rev Saude Publica.
1996;30(6):512-8. DOI:10.1590/S0034-89101996000600004
35. World Health Organization. Appropriate use of fl uorides for human health. Geneva; 1986.
36. World Health Organization. Fluorides and oral health: report of a WHO Expert Committee on Oral Health Status and Fluoride Use. Geneva; 1994. (WHO Technical Report Series, 846).
37. World Health Organization. Guidelines for
drinking-water quality: recommendations. 3. ed. Geneva; 2004.
v.1.