www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Two-level
septocolumellar
suture
technique
for
correction
of
septal
caudal
dislocation
夽
Nevzat
Demirbilek
a,
Cenk
Evren
a,∗,
Mustafa
Suphi
Elbistanlı
b,
Uzay
Altun
a,
Selda
Sarikaya
Günay
caDepartmentofOtolaryngology,HeadandNeckSurgery,MedilifeBeylikduzuHospital,Istanbul,Turkey
bDepartmentofOtolaryngology,HeadandNeckSurgery,BakirkoyDr.SadiKonukTrainingandResearchHospital,Istanbul,Turkey cDepartmentofOtolaryngology,HeadandNeckSurgery,KemerGovernmentHospital,Antalya,Turkey
Received13May2015;accepted22June2015 Availableonline5November2015
KEYWORDS Septalcaudal dislocation; Septumfixation; Newsuturetechnique
Abstract
Introduction:Caudalseptaldislocationisarespiratoryandcosmeticproblem.Thecorrection ofcaudal septaldislocationis achallengingissue. Althoughdifferent modalitieshave been describedforthetreatment,itisstillcontroversial.
Objectives: Thisstudy aims todescribeatwo-levelsuture techniquewhichcan beused to correctandstabilizetheseptuminthecolumellarpocket.
Methods:Thecaudalseptumwasfixedtothenasalspinewithsuturing,andananterior col-umellarpocketwasformed.Twoseptocolumellarsuturesincludingsuperiorandinferiorwere performed to correct thedislocated caudal septumandto increase the stability ofcaudal septuminthecolumellarpocket.
Results:Anteriorrhinoscopyshowednorecurrentdeviationordislocationinourpatients.
Conclusion: Oursuturetechniqueisaneffectiveandeasy-to-usemethodtocorrectthe cau-dal septaldislocation. Itcan also beused toincrease thestability ofcorrected septumby othertechniques.Atwo-levelsuturetechniqueincreasesthesuccessofcorrectionandreduces theriskofpostoperativeseptalcaudalluxation,stabilizingthesuperiorportionofthecaudal septum,inparticular.Therefore,itwouldreducetherateofredosurgeries.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http://
creativecommons.org/licenses/by/4.0/).
夽 Pleasecitethisarticleas:DemirbilekN,EvrenC,ElbistanlıMS,AltunU,GünaySS.Two-levelseptocolumellarsuturetechnique for correctionofseptalcaudaldislocation.BrazJOtorhinolaryngol.2016;82:403---7.
∗Correspondingauthor.
E-mail:[email protected](C.Evren).
http://dx.doi.org/10.1016/j.bjorl.2015.06.009
404 DemirbilekNetal.
PALAVRAS-CHAVE Desvioseptalcaudal; Fixac¸ãodesepto; Novatécnicade sutura
Técnicadesuturaseptocolumelaremdoisníveisparacorrec¸ãodedesvioseptal caudal
Resumo
Introduc¸ão:Odesvioseptalcaudaléumproblemarespiratórioeestético,easuacorrec¸ãoé tarefadesafiadora.Emboratenhamsidodescritasdiferentesmodalidadesparaotratamento, esseéaindaumtópicocontroverso.
Objetivos: Opresenteestudoobjetivoudescreverumatécnicadesuturaemdoisníveis,que podeserempregadanacorrec¸ãoeestabilizac¸ãodoseptonabolsacolumelar.
Método: Oseptocaudalfoifixadoàespinhanasalcomsuturas,apósarealizac¸ãodeumabolsa columelaranterior.Duassuturasseptocolumelares,superioreinferior,foramaplicadasparaa correc¸ãododesvioseptalcaudale,também,paramaiorestabilidadedoseptocaudalnabolsa columelar.
Resultados: Rinoscopiaanteriornãoresultouemrecorrênciadodesvioouluxac¸ãoemnossos pacientes.
Conclusão:Nossatécnicade suturaé ummétodo efetivoe defáciluso paraacorrec¸ãodo desvioseptalcaudal.A técnicatambémpodeserutilizada paraaumentaraestabilidadede septoscorrigidosporoutrastécnicas.Atécnicadesuturaemdoisníveisaumentaosucesso dacorrec¸ãoediminuioriscodeluxac¸ãoseptalcaudal,estabilizando,emparticular,aparte superiordoseptocaudal.Portanto,nossatécnicadiminuiopercentualdereoperac¸ões. © 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http://
creativecommons.org/licenses/by/4.0/).
Introduction
Correctionofseptalcaudaldislocationisachallenging prob-lem for both the surgeonand thepatient. Septalfixation tothenasal spine is a primarymethodfor stabilizing the caudalseptum. However,itcan becomplicatedfor a sur-geonwith limited experience, while it can be unfeasible forthenasalspineresection,evenforanexperienced sur-geon.Although itis stabilized,fixationcan beinadequate duetodamagedseptalandnasalspineconnections,thereby leadingtopostoperativeluxation-inducedre-deviation.1In addition,insufficientsupportorover-resectionmay cosmet-icallyproducelossoftipprojection,columellarretraction, andsupratipdepression.1
The earliestandmost commonmethod for the correc-tionofseptalcaudaldislocationisMetzenbaum’s‘‘swinging door’’(SD)technique.Usingthistechnique,dislocated cau-dal septum is shifted on the midline and fixed to nasal spine.Inlateryears,Noormanpublishedamodificationof theSDtechniquewhichincludesusingmaxillarycrestasa doorstopaftershiftingofdislocatedseptumtotheopposite sideofdislocation.2Anothermethodwasdescribedby Gold-man,inwhichcartilagescoring,resectionandsuturingsteps were defined. Furthermore, the modified Goldman tech-nique, which includes triangular cartilage resection from dislocated caudalseptal cartilage and suturing steps was describedbyLawson.3
Twodifferentsuturetechniques,whichcanbeusedboth tocorrectthecaudalseptaldislocationandasacomplement toprevious fixation ofcartilage tonasal spine techniques byincreasingthestabilityofcaudalseptumwerepublished intheliterature.Batiogluetal.4describedacaudalseptal suture technique that can be used single or complemen-tary to previous techniques, in which the caudal septum
is sutured to the soft tissue between the medial crura of thelowerlateral cartilagesby incisingthemidpoint of thecolumellaskinfromoutsidewithnon-absorbablesuture material. Kenyon et al.5 also described a technique that includesfixationofthedislocatedcaudalseptuminthe col-umellarpocketwithmidpointmattresssuture.
Inthisstudy,weaimedtodescribean easywayto cor-rect and increase the stability of the caudal septum in columellarpocketbysuturingitintwo-level,thus preven-tingre-dislocationofthecaudalseptum.
Methods
This technique was performed between August 2010 and July2014.Oursuturetechniquewasusedinpatients under-going septoplasty due tomild to moderate septal caudal dislocation withorwithout nasalseptaldeviationofother partsofthenasalseptum.Atotalof71patientswho under-wentseptoplastyusingthecombinedseptocolumellarsuture technique were enrolled.The study wasapproved by the EthicsinResearchCommitteeoftheinstitution,under pro-tocol2014/246.
Patients with septal caudal dislocation have been grouped as mild, moderate and severe depending on the degreeofnarrowingofthenaresbydislocatedcaudalendof nasalseptum.Dislocationsnarrowingthenaresmediallyup to25%wereacceptedasmild,from25%to50%asmoderate, andover50%assevere.
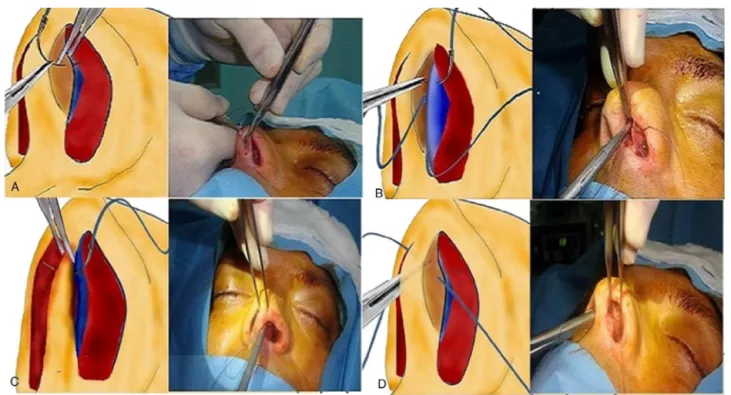
Figure1 Thesequencesofthesuperiorseptocolumellarsuture.
Aunilateralhemi-transfixionincisiontotheanteriorportion ofthenasalseptumwasperformed.The incisionwas per-formed through the dislocated side of the septum and 2---3mm posterior to the cauda. Both mucoperichondrial flapswereelevatedandanappropriatetechniqueforseptal pathology wasapplied.L-strut waspreserved to maintain the structural function of the septum. The anterior sep-tum was freed from all mucosal connections. Deviations of maxillary crest were corrected by excision or medial replacement.Ofnote,excesscartilageinthecaudalseptal baseisresected.Othertechniquesincludingscoring, trian-gular cartilage resectionor shiftingthe caudalseptum to theoppositesideofdislocationwerecarriedout.Atunnel betweenthemedialcrusofthealarcartilageswascreated withangledconversescissorsorcurvedirisscissors.The sep-tumwasinitiallyre-attachedtothemaxillaryspinethrough a4.0absorbablemonofilamentsuture(Vicryl®,EthiconInc.,
USA).
The cartilage wasthen preparedforsuperior septocol-umellarsuturewitha4.0absorbablemonofilamentsuture (Vicryl®,Ethicon Inc.,USA). Firstsuturewasplaced
supe-riorly. The needle first passed through the alar cartilage of incision side from lateral to medial 3mm anterior to the mucoperichondrial incision(Fig. 1A). The needle was advancedthroughtheseptalcartilage(Fig.1B).Theneedle passed through non-deviated, non-incised side mucoperi-chondriumfrommedialtolateral (Fig.1C).Full-thickness was reinforced 2mm posterior of the mucoperichondrial incision,theneedlewasremovedat thecontra mucoperi-chondriumanditwas,then,tied(Fig.1D).
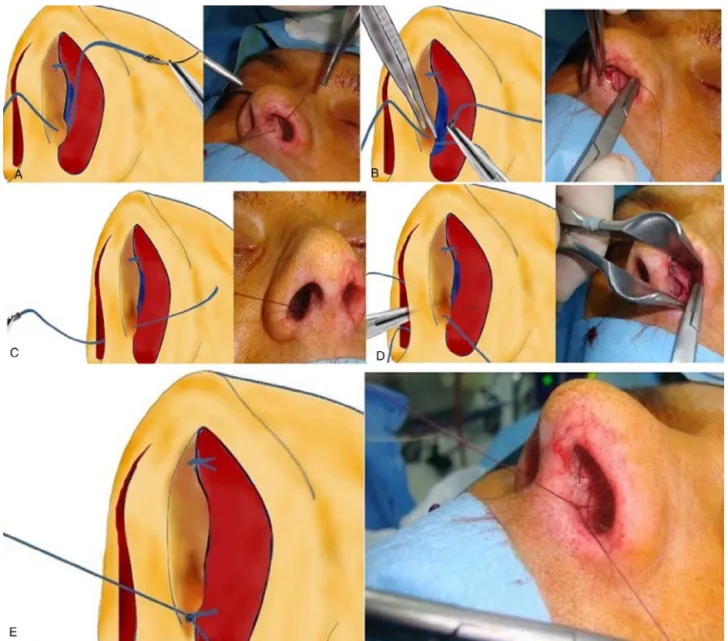
Inferiorseptocolumellarsuturingwasperformed witha 4.0absorbablemonofilamentsuture(Vicryl®,EthiconInc.,
USA). The needle first passed through the alar cartilage of incision side from lateral to medial 3mm anterior to the mucoperichondrial incision(Fig. 2A). The needle was
advancedthroughtheseptalcartilage(Fig.2B).Theneedle passed through non-deviated, non-incised side mucoperi-chondriumfrommedialtolateral(Fig.2C).Full-thickness was reinforced 2mm posterior of the mucoperichondrial incision,theneedlewasremoved atthecontra mucoperi-chondriumanditwas,then,tied(Fig.2DandE).
InternalDoylesiliconsplintswereleftinplacefor2days inallcases.
Results
We performed this suturing technique on 71 septoplasty casesduringfouryears.Amongthem,44(62%)weremales and27(38%)werefemales. Totalfollow-upperiodranged between6and18months.Onepatient(1.4%)had surgery-related bleeding. Anterior packing was replaced in this patient. Two patients (2.8%) had columellar indurations withinthefirstweekfollowingsurgery,resolvedwith antibi-otic pomade. Anterior rhinoscopy showed no recurrent deviation or dislocation. Total follow-up duration was 6 months in 29 patients, one year in 23 patients, and 18 months in 19 patients. Preoperative (Fig. 3A) and sixth month postoperative(Fig. 3B)pictures of apatient oper-atedwithtwolevel septocolumellarsuture technique are seen.
Discussion
406 DemirbilekNetal.
Figure2 Thesequencesoftheinferiorseptocolumellarsuture.
Asthemostinvolvedareaistheanteriorpartofthenose, septumshouldberobustlyfixedduringsuturingattheend of surgery. Anterior septal deformity repair, in particular, is effective in preventing several complications including supratip depression, columellarretraction, andexpansion of the nasal base.1 Although a successful surgery can be performed,insufficientfixationmayyieldundesirable out-comes.Oursuturetechniquedescribesawaytofixcaudal septumbetweentwocolumellarcruras.Itcanbeused addi-tionallytoSDormodifiedSDtechniques.
InMetzenbaum’spopularSDtechnique,dislocatedcaudal septumisshiftedonthemidlineandfixedtonasalspine.In lateryears,NoormanmodifiedSDtechniquebyusing maxil-larycrestasadoorstopaftershiftingofdislocatedseptumto theoppositesideofdislocation.2Bothtechniquesare effec-tivetocorrectcaudaldislocations; however,theymaybe inadequateforselectedcasesorincasesinwhichmaxillary spinemustberemovedandcaudalseptalfixationmaynotbe adequateorsometimesimpossible.Also,upperpartof cau-dalseptumtendstodislocatefollowingtheproceduredue
toinsufficientsupporttothisportion.Inthepresent tech-niquewithatwo-levelfixation,stabilityincreasedandthe riskfordislocationdecreased.InthemodifiedSDtechnique, ontheother hand, caudalseptum partremoved fromthe othersideofmaxillaryspinemaynarrowtheairwaypassage. When combinedwiththeSDtechnique,oursuturing tech-nique mayyield tomidwayposition ofthe caudalseptum andequalairwaypassages.
Figure 3 Preoperative and sixth month postoperative pic-tures.
Finally,thecaudaltipoftheseptumwasknottedinthe col-umellarpocket.A3.0non-absorbablemonofilamentsuture wasused.They describeddimple-shaped shrinkageonthe columellarskin afterthe procedure.Although theyreport thatthisshrinkagedisappearedwithinthefirstmonth and complete epithelization wasachieved,this condition may becomeuncomfortableforthepatient.Inaddition,asthis techniqueincludesamidpointskinincisiontocolumella,it maycausescarring.Anon-absorbablesuturematerialused in thistechniquemay yieldtosuture materialreactionin thelong-term,even.Furthermore,buryingthesuturetosoft tissuebetweenmedialcrurasofthelowerlateralcartilages maybechallenginginunexperiencedhands.Unlessitisnot performedalone,one-levelfixationmaynotbesufficientto preventre-deviation.Ourtechniqueusesabsorbablesuture materials withoutany skinincisions.Sinceit isperformed layerbylayer,itisveryeasytolearnandtoperform. Two-level fixation may overcome the limitations of one-level fixation.
Inanotherstudy,Kenyonetal.5describedmattresssuture techniques in septaldislocation. A mattress suture in the incisionsite wasusedto fixthe septumto open the full-thicknesscolumellarpocketwithaKenyonsuturetechnique. An absorbablesuturesuch as3.0VicrlyRapide® wasused.
In this technique, septum is fixed in one level and mat-tress suture is performed through all threemedial crura, septum,medialcruralayersatoneprick.However,itmay bedifficulttoadjustthepositionofthecaudalseptumin thecolumellarpocket.Inaddition,itcanonlystabilizethe septumverticallyandwhenperformedaloneitmaybe inad-equateforfixation,asitisamattresssutureandperformed atonelevel.Inourtechnique,backwardmovementofthe
needlewasstarted2mmposteriortofirstoutwardincision, thereby,horizontallystabilizing theseptum.Furthermore, two-levelsuturingverticallyfixatesthecaudalseptum.We believethat layeredadvancing of the needlethroughthe cartilagesiseasierevenforinexperiencedsurgeons.
Wedidnotperformnasalspirometry,acousticrhinometry orradiological stagingofnasalseptaldeviations to evalu-atetheseverityofnasalseptaldeviationofthepatients.It isalimitationtothisstudyinobjectivepatientselection. BecauseMladina Classification6 does not give information abouttheseverityof theseptalcaudaldislocation wedid not use it in the selection of patients as mild or moder-ate.Weselectedpatientsasmildormoderatedependingon inferiorappearanceofdislocatedcaudalseptum.We used the degree of narrowing of the nares by the caudal end ofdislocated septum. Patientsaccepted as severe caudal dislocation thoughttobe difficult tobeevaluated byour techniqueandtheywereoperated asopen septoplastyor septorhinoplasty.
Conclusion
In conclusion, we suggest that two-level septocolumellar suturingis an effective and easy-to-use technique in the fixationofmildtomoderatecaudalseptaldeviations, sup-portingthe nasaltipand preservingitssymmetry. It does not require cartilage resection, thus preventingnasal tip supportloss.IncombinationwiththeSD,modifiedSD, Gold-manandmodifiedGoldmantechniquesofferanadvantage. Basedonourcurrentexperience,itcanyieldconsiderable functionalandcosmeticoutcomesinthetreatmentof cau-dalseptaldislocations.Inaddition,itisunlikelytoleadto anyscarorrequireseptalsupportanditpreventsnasaltip complications.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Bloom JD, Kaplan SE, Bleier BS, Goldstein SA. Septoplasty complications: avoidance and management. Otolaryngol Clin NorthAm.2009;42:463---81.
2.PastorekNJ,BeckerDG.Treatingthecaudalseptaldeflection. ArchFacialPlastSurg.2000;2:217---20.
3.LawsonWL,WestreichR.Correctionofcaudaldeflectionsofthe nasalseptum withamodifiedGoldmanseptoplastytechnique: howwedoit.EarNoseThroatJ.2007;86:617---20.
4.Batioglu-KaraaltinA,YigitO,DonmezZ.Anewpersistentsuture techniqueforcorrectionofcaudalseptaldislocation.JCraniofac Surg.2014;25:2169---71.
5.Kenyon GS,Kalan A,Jones NS.Columelloplasty:anewsuture technique to correct caudal septal cartilage dislocation. Clin OtolaryngolAlliedSci.2002;27:188---91.