www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
High
frequency
hearing
thresholds
and
product
distortion
otoacoustic
emissions
in
cystic
fibrosis
patients
夽
,
夽夽
Lucia
Bencke
Geyer
a,b,∗,
Sergio
Saldanha
Menna
Barreto
b,c,
Liese
Loureiro
Weigert
a,b,
Adriane
Ribeiro
Teixeira
d,eaHospitaldeClínicasdePortoAlegre,PortoAlegre,RS,Brazil
bChildandAdolescentHealth,UniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil cTorontoUniversity,Toronto,Canada
dBiomedicalGerontology,PontifíciaUniversidadeCatólicadoRioGrandedoSul(PUC-RS),PortoAlegre,RS,Brazil
eDepartmentofHumanHealthandCommunication,UniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil
Received31March2014;accepted4October2014 Availableonline8September2015
KEYWORDS
Cysticfibrosis; Aminoglycosides; Audiometry
Abstract
Introduction:Thetreatmentofpatientswithcysticfibrosisinvolvestheuseofototoxicdrugs, mainlyaminoglycosideantibiotics.Duetotheuseofthesedrugs,fibrocysticpatientsareatrisk ofdevelopinghearingloss.
Objective: ToevaluatethehearingofpatientswithcysticfibrosisbyHighFrequencyAudiometry andDistortionProductOtoacousticEmissions.
Methods:Cross-sectionalstudy.Thestudygroupconsistedof39patients(7---20yearsofage) withcysticfibrosisandacontrolgroupof36individualsinthesameagegroupwithout oto-logiccomplaints,withnormalaudiometricthresholdsandtypeAtympanometriccurves.High FrequencyAudiometryandDistortionProductOtoacousticEmissionstestswereconducted. Results:Thestudygrouphadsignificantlyhigherthresholdsat250,1000,8000,9000,10,000, 12,500,and16,000Hz (p=0.004)aswellashigherprevalenceofotoacoustic emission alter-ationsat1000and6000Hz(p=0.001),withsignificantlyloweramplitudesat1000,1400,and 6000Hz.TherewasasignificantassociationbetweenalterationsinhearingthresholdsinHigh FrequencyAudiometrywiththenumberofcoursesofaminoglycosidesadministered(p=0.005). Eighty-threepercentofpatientswhocompletedmorethantencoursesofaminoglycosideshad hearinglossinHighFrequencyAudiometry.
夽 Pleasecitethisarticleas:GeyerLB,MennaBarretoSS,WeigertLL,TeixeiraAR.Highfrequencyhearingthresholdsandproductdistortion
otoacousticemissionsincysticfibrosispatients.BrazJOtorhinolaryngol.2015;81:589---97.
夽夽Institution:HospitaldeClínicasdePortoAlegre,PortoAlegre,RS,Brazil. ∗Correspondingauthor.
E-mail:[email protected](L.B.Geyer).
http://dx.doi.org/10.1016/j.bjorl.2015.08.011
Conclusion:Asignificantnumberofpatientswithcysticfibrosiswhoreceivedrepeatedcourses ofaminoglycosidesshowedalterationsinHighFrequencyAudiometryandDistortionProduct OtoacousticEmissions.Theimplementationoftenormoreaminoglycosidecycleswasassociated withalterationsinHighFrequencyAudiometry.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Fibrosecística; Aminoglicosídeos; Audiometria
Limiaresauditivosemaltasfrequênciaseemissõesotoacústicasnafibrosecística
Resumo
Introduc¸ão:Otratamentodospacientescomfibrosecísticaenvolveousodemedicamentos ototóxicos,principalmentedeantibióticosaminoglicosídeos.Devidoaousodestes medicamen-tos,ospacientesfibrocísticosapresentamriscodedesenvolverperdaauditiva.
Objetivo:Avaliaraaudic¸ãodospacientescomfibrosecísticapela AudiometriadeAltas Fre-quências(AAF)eEmissõesOtoacústicasporProdutodeDistorc¸ão(EOAPD).
Método: Estudotransversal.Ogrupodeestudofoi constituídopor39 pacientescomidades entre7e 20anoscomfibrose císticaeo grupocontrolepor36 indivíduos damesmafaixa etária,semqueixasotológicas,comlimiaresaudiométricosnormaisecurvastimpanométricas tipoA.Foramrealizadososexamesdeaudiometriadealtasfrequênciaseemissõesotoacústicas porprodutodedistorc¸ão.
Resultados: Ogrupodeestudoapresentoulimiaressignificativamentemaiselevadosem250; 1000;8.000;9.000;10.000;12.500e16.000Hz;(p=0,004)emaiorprevalênciadealterac¸ões nasemissõesotoacústicasem1.000e6.000Hz(p=0,001);comamplitudessignificativamente maisbaixasem 1.000;1.400 e6.000 Hz.Houve associac¸ão significativaentreasalterac¸ões dos limiares auditivos naAAF como número de ciclosde aminoglicosídeos realizados (p = 0,005).Oitentaetrêsporcentodos pacientesqueforamsubmetidos amaisde3ciclosde aminoglicosídeosapresentaramperdaauditivanaAAF.
Conclusão:Umnúmerosignificativodepacientescomfibrosecísticaquereceberamrepetidos ciclosdeaminoglicosídeosapresentoualterac¸õesnaAAFeEOAPD.Arealizac¸ãode10oumais ciclosdeaminoglicosídeosesteveassociadaàsalterac¸õesnaAAF.
©2015Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Cysticfibrosis (CF) is the most common autosomal reces-sive genetic disease amongwhite patients. It affects the exocrineglands,which,whenproducingabnormallyviscous secretions,causeaseriesofmanifestations,mainly respira-toryanddigestive.1,2CFiscausedbyaseriesofmutationsin
agenethatperformscysticfibrosistransmembrane conduc-tanceregulator(CFTR)encoding.3Malfunctionorabsenceof
CFTRactivitycausesdehydrationofthemucoussecretions andanincreaseinitsviscosity,favoringtheobstructionof theductsandconsequentinflammationandfibrosis.4---6
Among themainagents forcochlear alterationthrough ototoxicityareAG(aminoglycoside)antibiotics,widelyused inthetreatmentofCFtocombatcolonizationbybacteria. Duetothefrequentuseofthistypeofdrug,patientswith cysticfibrosisareathighriskofdevelopinghearingloss.7---10
Thehearingmonitoring ofpatientsexposedtoototoxic agents aimstodetect hearingloss beforethe occurrence ofimpairmentattherangeoffrequenciescorrespondingto speech,withconsequentdamagetocommunication;andto enableanearlyaudiologicalinterventionthroughindividual hearing aids and speech therapy in those cases in which
hearinglossisalreadyevident.11---13Thismonitoringis
espe-ciallycriticalforthepediatricpopulation,forevenhearing loss limited to high frequencies can impair the child’s language development.14 Currently, the most commonly
used procedures to monitor hearing function in cases of ototoxicityare:puretoneaudiometry(PTA),highfrequency audiometry(HFA),andotoacousticemissions(OAE).13
HFAevaluatespuretoneairconductionthresholdsinthe 9---20kHz range, depending on the equipment. This is an importanttestfortheearlydetectionofhearinglosscaused by damagetothe baseof the cochlea,asoccursin cases of ototoxicity, becauseit allows the detection of hearing lossbeforereachingtheconventionallymeasuredfrequency range(250---8000Hz).15,16
TheliteraturepresentssomestudiesonCFpatients eval-uating hearing by HFA. Fausti etal.17 conducted PTA and
HFA in 53 patients after treatment with AG.Hearing loss was detected in 47% of evaluated ears, and HFA alter-ation was primarily detected in 71% of ears. In previous studies, other authors found similar outcomes with high hearing thresholds in HFA following AG treatment in CF patients.18,19However,Mulheranetal.20foundthattherisk
2% for an intravenous antibiotic course. The authors sug-gestedthat the diseasemay attenuate theprogressionof cochleotoxicity,thankstotherapidrenalclearanceofthese drugs. Mulheran et al.21 reinforced this assumption with
HFA,withabsenceofcochleotoxicityaftertreatmentwith tobramycininCFpatients.Theauthorshighlightedthefact thatthecumulativeeffectofAGwasnotassessed,because the aim of their study was toevaluate the cochleotoxic-ityoftobramycinadministeredonetothreetimesperday. Whenassessingtheprevalenceofhearinglossandits rela-tiontotheuseofantibioticsinCF,Chengetal.10observed
hearing loss by PTA in 14% of 50 patients and identified theadministration often or morecoursesof AG asarisk factor.
Examination by OAE does not require that the patient providesresponses,andthistestis verysuitableforsmall childrenandevenforadultsunabletorespondtotestssuch as audiometry.22 In addition, changes in OAE may reflect
cochlear damagethat isnotasyetdetectableby audiom-etry. Decreases in amplitude and in the dynamic area of responses and/or loss of distortion product OAE (DPOAE) responsecanresultifthereisachange inthefunctionof outerhaircells.23
InastudyofCFpatientsandacontrolgroup,Mulheran etal.24observednormalhearingthresholdsinbothgroups;
however, these authors detected a significant increase of the stimulus required to generate DPOAE at 4kHz in CF group. The authors suggested that this rise could repre-sentoneofthefirstalterationsoccurringinouterhaircells, causedbygentamicin.Stavroulakietal.8foundthatDPOAE
is more sensitive than PTA in detecting cochlear changes aftertheuseofgentamicin.UsingDPOAE,otherauthors25,26
alsofoundcochlearalterationsoccurringpriortochangesin hearingthreshold.However,someauthors,intheirstudies withototoxicagents,claimthatHFAismoreeffectivethan OAEtodetecthearingloss.23,27---29
InBrazil,therearefewstudiesonCFpatients’hearing utilizinghigh frequency audiometry.Therefore, thisstudy aimedtoevaluatehearingthresholdstestinghigh frequen-ciesandusingDPOAEinCFpatientsfromthisinstitution.
Methods
This study was approved under No. 120096 by the Ethics Committeeoftheinstitution.
Thiswasanobservational,cross-sectionalstudy.The pop-ulationstudiedwascomposedofastudygroup(SG)with39 childrenandadolescentsreferredfromadultandpediatric cysticfibrosis (CF)outpatientclinicsfromthis institution. The controlgroup(CG)comprised36 childrenand adoles-centsfromtheinstitution’sotorhinolaryngologyoutpatient clinic,trainees,andchildrenofemployeesoftheinstitution andstudentsofastateelementaryschool.
The inclusion criteriafor the study group were as fol-lows:individualswithaconfirmeddiagnosisofCF,aged7---20 years,treatedattheCFoutpatientclinic,withtypeA tym-panometriccurve30 compatiblewithamiddle earwithout
otological abnormalities. For the control group, inclusion criteriawereindividualsaged7---20yearswithoutotological andauditorycomplaintsandwithanAtypetympanometric curve.30
Exclusion criteria for study and control groups were as follows: individuals with illnesses associated with ear repercussion (e.g., meningitis, acoustic trauma, tinni-tus, otorrhea, history of recurrent otitis media in early childhood),familyhistoryofhearingloss,typeBorC tym-panometric curve,30 and/or refusal to sign the informed
consent(AppendixI).Thehistoryofdiseasesassociatedwith earrepercussionwasverifiedbyreviewingmedicalrecords.
Instrumentsandmeasures
Theprotocolfollowedtocarryoutthetestswasthesame usedintheotorhinolaryngologyandspeechtherapy outpa-tientclinicfromtheinstitution.Thetestswereperformed bytwotrainedspeechtherapists.
Initially, the subject was submitted to an ear evalua-tion by an otorhinolaryngologist. Then, tests of acoustic impedance,puretoneaudiometry,highfrequency audiom-etry, and product-distortion otoacoustic emissions were conducted.Afterthetests,thepatient’smedicalrecordwas analyzedinordertocollectdatarelevanttothestudy.
The impedancemetry examinations were performed withtheAZ26Impedancemeter(Interacoustics---Denmark), withtympanometryanda surveyof contralateralacoustic reflexes. The pure tone and high frequency audiometry testswereperformedwiththeSiemensUnityPC audiome-ter (Germany), calibrated in dB HL according to ANSI standard3.6-1989 withtheuse of HDA2000 airand bone conductionB-71phones. Pure toneaudiometryby airand bone conduction was performed at 250---16,000Hz and at 500---4000Hz, respectively. All audiological tests were performedbytwotrainedspeechtherapistsusingthesame evaluationprotocol.
Thecriteriaofnormalityusedforpuretoneaudiometry weretheInternationalBureauforAudiophonology(Bureau International d’Audiophonologie [BIAP]) classification, in whichthe averageof the frequenciesof 500,1000, 2000, and4000Hz<20dBHLisconsideredasnormalhearing.For highfrequencies (9000---16,000Hz),thresholds up to25dB HLwereusedasacriterionofnormality,asdocumentedin previousstudiesofnormalhearingindividuals.31---34
The distortion-product otoacoustic emissions test was conductedinanacousticallytreatedroomwiththeILO292 system(Otodynamics---England).Theexaminationwas per-formedinthefrequenciesof1000,1500,2000,3000,4000, and6000Hz. Aprobe wasinserted into the patient’s ear, withan audiblestimulussimultaneously generatedby two pure tonesof differentfrequencies (F1 and F2),in which F1=65dB, F2=55dB, and F2/F1=1.22. The test was ana-lyzedby a DP-gram chart,and presence of response was consideredasthefindingofamplitudesequaltoorgreater than3dBSPLabovethenoiselevel.35
Statisticalanalysis
Tocomparemeansbetweengroups,Student’st-testfor independentsampleswasapplied.Inthecaseofasymmetry, theMann---Whitneytestwasused.
Inthecomparisonofproportions,Fisher’sexacttestwas used.
Thesignificancelevelwassetat5%(p≤0.05)and analy-seswereperformedusingSPSSsoftware,version18.0.
Results
The sample consisted of 75subjects: SG=39 and CG=36. Themeanagewas13.0(±3.2)and12.3(±4.1)yearsforthe SGandCG, respectively. The participants’age range was 7---20years.Twenty-twosubjectsintheSG(56.4%)and12 intheCG(33.3%)weremale.Table1shows theresultsof thedescriptiveanalysisofageandgendervariablesforeach group,geneticmutationsinCF,andnumberofintravenous AGcyclesreceivedbySGparticipants.
There was nostatistically significant difference in age andgendervariablesbetweentheSGandCG,indicatingthat thesubjectsweresimilarintheseaspects.Therefore,the samplewasanalyzedwithoutreferencetothesevariables. Intheanalysisofauditorythresholdsbetweenrightandleft ear,a statisticallysignificantdifferencewasnotedonlyin thefrequencyof250HzintheSG;inotherfrequenciesand intheCGtherewasnosuchadifference. Forthisreason, theearswereanalyzedwiththeuseoftheirmeansateach frequency.
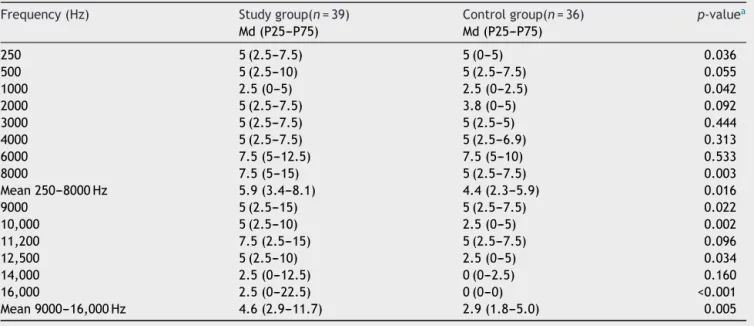
When auditory thresholds were compared between groups, the SG had significantly higher thresholds at 250Hz, 1000Hz, 8000Hz, 9000Hz, 10,000Hz, 12,500Hz, and 16,000Hz. The mean values at 250---8000Hz and at 9000---16,000HzweresignificantlyhigherintheSG(Table2). TheSGshowedahigherprevalenceofhearinglossbyHFA (p=0.004)(Fig.1).UsingPTAintherangeof250---8000Hz, neithergroupexhibitedabnormalities.
Table1 Samplecharacterization.
Variable Studygroup (n=39)
Controlgroup (n=36)
p-Value
Age(years), mean± SD
13.0±3.2 12.3±4.1 0.420a
Agegroup,n(%) 0.223b
<12years 11(28.2) 16(44.4) 12---17years 24(61.5) 15(41.7) >18years 4(10.3) 5(13.9)
Gender,n(%) 0.076b
Male 22(56.4) 12(33.3) Female 17(43.6) 24(66.7)
Mutation,n(%)
---DeltaF508 23(92.0) ---R553X 1(4.0) ---L543XandA561E 1(4.0)
---AGcourses,n(%)
---<10 33(84.6) --->10 6(15.4)
---SD,standarddeviation;AG,aminoglycosides. a Student’st-test.
b Chi-squaredtest(Pearson).
TheSGshowedasignificantlyhigherprevalenceofDPOAE alterationwhencomparedtothe CG(p=0.001),asshown inFig.2.
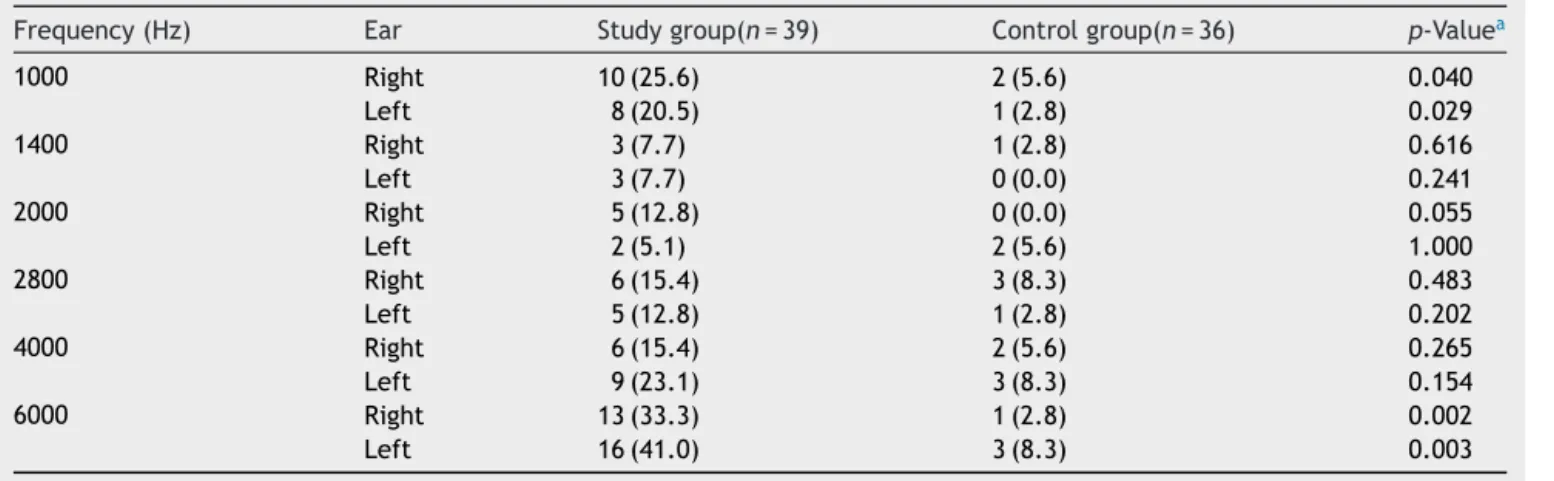
TheSGpresentedmoreDPOAEalterationsat1000Hzand 6000Hzinbothears(Table3),whencomparingrightandleft ears ateach frequency andfor each group.Nosignificant differencebetweentheearswasnoted(p>0.20).
WhencomparingDPOAEamplitudesbetweengroups,the SGhadloweramplitudes at1000Hz,1400Hz,and6000Hz (Table4).Whencomparingleftandrightearswithrespect
Table2 Comparisonofhearingthresholds(dBHL)betweengroups.
Frequency(Hz) Studygroup(n=39) Controlgroup(n=36) p-valuea
Md(P25---P75) Md(P25---P75)
250 5(2.5---7.5) 5(0---5) 0.036
500 5(2.5---10) 5(2.5---7.5) 0.055
1000 2.5(0---5) 2.5(0---2.5) 0.042
2000 5(2.5---7.5) 3.8(0---5) 0.092
3000 5(2.5---7.5) 5(2.5---5) 0.444
4000 5(2.5---7.5) 5(2.5---6.9) 0.313
6000 7.5(5---12.5) 7.5(5---10) 0.533
8000 7.5(5---15) 5(2.5---7.5) 0.003
Mean250---8000Hz 5.9(3.4---8.1) 4.4(2.3---5.9) 0.016
9000 5(2.5---15) 5(2.5---7.5) 0.022
10,000 5(2.5---10) 2.5(0---5) 0.002
11,200 7.5(2.5---15) 5(2.5---7.5) 0.096
12,500 5(2.5---10) 2.5(0---5) 0.034
14,000 2.5(0---12.5) 0(0---2.5) 0.160
16,000 2.5(0---22.5) 0(0---0) <0.001 Mean9000---16,000Hz 4.6(2.9---11.7) 2.9(1.8---5.0) 0.005
40
30.8
2.8 35
30 25
Prevalence (%)
20
15
HFA alteration (9.000 - 16.000 Hz) 10
5
0
Study group Control group
Figure1 AlterationsinHFAinstudyandcontrolgroups.HFA, highfrequencyaudiometry.
toDPOAEamplitude,therewassignificant differenceonly at4000HzintheSG(p=0.037).
WefoundthatDPOAEalterationsoccurredwhentesting highfrequencies,bothinthestudygroupwithnormalHFA (66.7%)andinthegroupwithHFAalterations(91.7%),albeit more oftenin the latter. However,the statistical analysis
40
25.6
Study group Control group
Prevalence (%)
66.7
74.4
33.3 50
60 70 80
30
20 10
Normal DPOAE DPOAE alteration
0
Figure 2 DPOAE in study and control groups. DPOAE, distortion-productotoacousticemissions.
showedthattherewasnoassociation betweenchangesin HFAandinDPOAEforSGparticipants(p=0.131)(Fig.3).
Therewasasignificant associationbetween changesin hearingthresholdsbyHFAwithnumberofAGcourses admin-istered (p=0.005). The administration of more than ten
Table3 ComparisonofalterationsinDPOAEbyfrequencyandbyearbetweengroups.
Frequency(Hz) Ear Studygroup(n=39) Controlgroup(n=36) p-Valuea
1000 Right 10(25.6) 2(5.6) 0.040
Left 8(20.5) 1(2.8) 0.029
1400 Right 3(7.7) 1(2.8) 0.616
Left 3(7.7) 0(0.0) 0.241
2000 Right 5(12.8) 0(0.0) 0.055
Left 2(5.1) 2(5.6) 1.000
2800 Right 6(15.4) 3(8.3) 0.483
Left 5(12.8) 1(2.8) 0.202
4000 Right 6(15.4) 2(5.6) 0.265
Left 9(23.1) 3(8.3) 0.154
6000 Right 13(33.3) 1(2.8) 0.002
Left 16(41.0) 3(8.3) 0.003
a Fisher’sexacttest.
Table4 Comparisonofamplitudes(dBSPL)ofDPOAEbetweengroups.
Frequency(Hz) Ear Studygroup(n=39) Controlgroup(n=36) p-Valuea
Md(P25---P75) Md(P25---P75)
1000 Right 10.1(5.5---15.3) 11.2(8.9---17.6) 0.168 Left 9.2(5.5---15.2) 13.3(9.6---7.2) 0.028 1400 Right 16.0(6.8---19.0) 15.6(13.2---19.1) 0.528 Left 14.5(6.9---18.2) 16.2(13.0---20.2) 0.041 2000 Right 12.6(6.5---16.9) 14.2(8.5---18.8) 0.233 Left 10.8(6.4---16.0) 14.1(7.8---18.8) 0.051 2800 Right 11.2(6.7---15.3) 12.4(5.4---16.1) 0.451 Left 10.2(4.5---13.8) 11.0(7.4---15.7) 0.148 4000 Right 9.2(2.0---14.8) 14.4(4.7---17.6) 0.166 Left 10.2(1.4---13.8) 11.2(7.4---16.6) 0.072 6000 Right 5.6(−3.2to12.2) 8.7(2.0---12.7) 0.102 Left 3.6(−4.1to10.2) 9.7(4.4---14.3) 0.007
40 60
Prevalence (%)
100
80
20
0
Normal DPOAE DPOAE alteration Normal HFA (n=27)
33.3 66.7
8.3 91.7
HFA alteration (n=12)
Figure 3 Association between HFA and DPOAE alterations inthestudy group.HFA,high frequencyaudiometry; DPOAE, distortion-productotoacousticemissions.
40
30
>10 AG courses
AAF normal AAF alteration 16.7
83.3
78.7
21.2
<10 AG courses 50
60
Prevalence (%)
100
80
70 90
20
10 0
Figure4 AssociationbetweennumberofAGcyclesandHFA alteration.AG,aminoglycosides;HFA,highfrequency audiome-try.
courses of intravenous AG was associated with a higher prevalenceofHFAalterations(Fig.4).
Discussion
HFA is described as the most effective method for early detectionof cochlear alterationsdue toototoxicity.23,29,36
Its use is still limited, due to lack of standardization of calibration and of normality parameters,16 particularly in
thepediatricpopulation,becauseoflowtest reliabilityin childrenunder7yearsofage.37
Conversely,evokedotoacousticemissionsisaquickand objectivetest,showingagreatadvantageforbothpediatric and adult population, who often fail to respond appro-priately to audiometry tests, due to the disease and its treatment.22,38 Consideringthefactthatotoacoustic
emis-sionsmayexhibitalterationseveninindividualswithnormal thresholds in the face of an early impairment of outer hair cells, this procedure is widely used in ototoxicity monitoring.11,39
Consideringthatoneofthemajorcausesofototoxicity istheuseofaminoglycosides,andthatCFpatientsreceive repeatedcoursesofthistypeofdrug,thispopulationisat highriskofdevelopingcochlearalterations.7---10
By analyzing the sample, there was nosignificant dif-ference in male versus female thresholds, as Abujamra etal.alsofound.29Althoughtheseauthorshavestudiedthe
effectsofothertypeofototoxicdrug(cisplatin),theyalso verifiednosignificantdifferences.
Neither was a significant difference detected in right
vs.leftearthresholds,andforthisreasontheears’mean wasusedtorepresentsuchthresholds.Instudieswith nor-malhearingindividuals,Sahyebetal.32 andSáetal.33also
detectednodifferencebetweentheearsusingPTAandHFA. When comparing hearing thresholds obtained by PTA (250---8000Hz) andHFA (9000---16,000Hz) between groups, significantly higherthresholds wereobserved in the study group,withthelargestdifferencesoccurringinHFA. Hear-inglosswasnotobservedinPTA;however,HFAdetectedhigh prevalenceofhearinglossinthestudygroup.Thesefindings demonstratetheimportanceofusingHFAinmonitoringCF patients.19,40
These results differ from those obtained by Martins etal.,41whoobservedhearinglossatconventional
frequen-cies and at high frequencies in their patients. However, Al-Malkyetal.42foundhearinglossonlyat8000---20,000Hz
byHFAandreducedamplitudesusingDPOAE,whichagrees withthepresentfindings.Inthatstudy,theauthorshighlight thefactthatalthoughthehearinglossisassociatedwithhigh AGexposure,itonlyoccurredin21%oftheexposedgroup. Facedwiththisfact,theauthorssuggestthattheremaybe otherfactorsresponsibleforhearingloss.
In the present study, higher number of alterations by frequencyandalsoloweramplitudesinDPOAEwerenoted in theSGvs.CG, evenwithnormalhearingthresholds up to 8000Hz. This findingsupports the study of Stavroulaki etal.,8whofounddecreased amplitudes ofDPOAEat
fre-quenciesabove3000HzinchildrenwithCFaftertreatment withgentamicin.Mulheranetal.,24 Katbamnaetal.,43 and
Katbamna et al.44 obtained similar outcomes, but these
authorsuseddifferentassessmentmethodsofDPOAE. Whentryingtoestablishapotentialassociationbetween alterationsinDPOAEandalterationsinHFA,sincethe alter-ationsinDPOAEoccurredmorefrequentlyinindividualswith alterationsinHFA,thisassociationwasnotfound.Thisresult mayberelatedtothesizeofthesample.This finding dis-agreed with that of Arnold et al.,45 who concluded that
hearing athigh frequencies significantly influencesDPOAE at lowerfrequencies. However,that study wasconducted withhealthy,normal-hearingyoungadults.
Withrespect to AG effects, it is known that repeated courses of treatment and its duration arefactors related toincreasedriskofototoxicity.46,47Inthepresentstudywe
observed asignificant associationbetween receivingmore thantenintravenousAGcoursesandHFAalterations.Some authorsfound similarresults,10,19,24 whilein anotherstudy
thefindingsweredifferent.40Intheirstudy,Mulheranetal.20
concludedthatthereispossiblyanincreasedriskof ototox-icity related tothe numberof AG coursestaken, but the authorspointoutthatthisrelationshipisnotlinear.Dueto thelow prevalenceof ototoxicityfound inCFpatients vs.
individualswithoutthediseasewhoweretreatedwithAG, someauthors20,48suggestthatCFitselfisaprotectivefactor
forototoxicity.Theseauthorssuggest thatsuchprotection maybe duetoalteredpharmacokinetics and/orunderlies changesinCFTR,butthatmoreresearchisneeded inthis area.Furthermore, itis knownthat CF resultsin afaster renalclearanceofdrugs,includingAG,49,50andthismayalso
A significantly higher prevalence of DPOAE alterations in SG, withthepresence of morealterations at 1000 and 6000Hz in both ears and withlower amplitudes at 1000, 1400,and6000Hz,suggestthatthistestshouldalsobe con-ductedinCFpatients,eveninthosewithnormalhearing. Thesignificantlyelevatedhearingthresholdsat250;1000, 8000,9000,10,000,12,500,and16,000Hzandtheexclusive presenceofHFAalterationsin30.8%oftheSGsuggestthat this assessment should be incorporated into the auditory monitoringofCFpatients.
Conclusion
ThisstudyshowedthatasignificantnumberofCFpatients who received repeated AG courses demonstrated HFA and DPOAE alterations, and that there was a significant association between administration of more than ten
intravenousAGcoursesandahigherprevalenceofHFA alter-ations.
Funding
ThisstudywasfundedbyCNPq.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Theauthorswouldliketoacknowledgethefinancialsupport providedbyCNPq.
Appendix
I.
Freeandinformedconsentform---StudyGroup
Weareinvitingyouand/oryourchildtoparticipateinthestudy‘‘Highfrequencyhearingthresholdsandproduct-distortion otoacousticemissionsincysticfibrosispatients.’’Thisstudyaimstostudyhearingteststhatcanshowifhearinglossoccursin patientswithcysticfibrosis,eveniftheirhearingdifficultyisnotperceived.
Youand/oryourchildarebeinginvitedtoparticipateintheresearchstudygroup,thatis,thegroupofparticipantswhohavecystic fibrosis.
Routineexaminationswillbeconducted:puretoneaudiometry,impedancemetry,andotoacousticemissions.Thetotaldurationof thethreetestsisapproximately40minutes.
Comparedtoroutineaudiometry,thedifferenceintheaudiometrythatwillbecarriedoutisthatawiderrangeofsoundswillbe evaluated.Wewillevaluatehigher-pitchsounds(veryhightones),makingitamorecomprehensiveexamination.Themainbenefit ofthisprocedureistoestablishanearlydiagnosisofhearinglossbeforethefrequenciesusedinthecommunication,i.e.,the frequenciesofspeech,areaffected.Toperformthistest,thepatientisplacedinsideasoundproofboothwithheadphonesintheir ears;thepatientwillhearwhistlesandshouldtelltheaudiologistwhentheyarehearingthesound.Theexaminationhasanaverage durationof30minutes.
Intheimpedancemetrytest,aheadphoneisplacedinoneofthepatient’sears,andintheotherearaprobeisplaced,causingslight pressureandsendingsomewhistles.Theaveragedurationofthistestisfiveminutes.
Intheotoacousticemissionstest,asmallprobeisplacedintheear;theprobesendssomesounds.Theaveragedurationofthistest isfiveminutes.
Thesethreetestsarepainlessandwelltoleratedbymostpatients,butifthereareanyunpleasantsensations,anyofthemmaybe discontinuedatonce.
Theparticipantand/orguardianhastherighttorequestinformationaboutthestudybeforeitisperformedandduringits
realization.Theparticipantand/orguardianalsohastherighttorefusetoparticipateorwithdrawtheirconsentatanystageofthe study,withoutanypenaltyandwithnoprejudicetotheparticipant’scare.
Theparticipant’sprivacywillalwaysbepreserved,aswellashis/hersensitivedata.Ifthestudyispublished,theparticipant’sname willnotberevealed.
Therewillbenocosttotheparticipantand/orguardianofhis/herparticipation. Acopyofthisdocumentwillbedeliveredtotheparticipantand/orguardian. Headresearcher:
Physician,PulmonologyDepartmentofinstitution. Contactphonenumber:(51)3359-8943
Participatingresearchers:
SpeechtherapistattheOtorhinolaryngologyDepartmentoftheinstitution,zone19. Contactphonenumber:(51)33598228
Participatingresearchers:
SpeechtherapistattheOtorhinolaryngologyDepartmentoftheinstitution,zone19. Contactphonenumber:(51)33598228
EthicsandResearchCommitteeoftheinstitution(forquestionsaboutethicalissuesonly) Phone:(51)33598304
Date: / / Participantname: Nameofparent/guardian: Parent/guardiansignature: Researchername:
References
1.Rubio T, Amaro G, Martínez G. Atención multidisciplinaria a pacientes con fibrosis quística. Rev Cubana Pediatr. 1999;71:228---32.
2.LubambaB,DhoogheB,NoelS,LealT.Cysticfibrosis:insight intoCFTRpathophysiologyandpharmacotherapy.ClinBiochem. 2012;45:1132---44.
3.DalcinPTR.FibroseCística.In:Menna-BarretoSS,editor. Pneu-mologianoconsultório.PortoAlegre:Artmed;2009.p.279---91. 4.Knowles MR,StuttsMJ,YankaskasJR,GatzyJT,Boucher RC. Abnormalrespiratoryepithelialiontransportincysticfibrosis. ClinChestMed.1986;7:285---97.
5.Wilschanski M, Zielenski J, Markiewicz D,Tsui LC, CoreyM, LevisonH,etal.Correlationofsweatchlorideconcentration withclassesofthecysticfibrosistransmembraneconductance regulatorgene-mutations.JPediatr.1995;127:705---10. 6.Proesmans M,Vermeulen F,De BoeckK. What’s new in
cys-ticfibrosis?Fromtreatingsymptomstocorrectionofthebasic defect.EurJPediatr.2008;167:839---49.
7.MulherinD,FahyJ,GrantW,KeoganM,KavanaghB,FitzGerald M.Aminoglycosideinducedototoxicityinpatientswithcystic fibrosis.IrJMedSci.1991;160:173---5.
8.Stavroulaki P, Vossinakis IC, Dinopoulou D, Doudounakis S, Adamopoulos G, Apostolopoulos N. Otoacoustic emissions for monitoring aminoglycoside-induced ototoxicity in chil-dren withcystic fibrosis. Arch Otolaryngol Head Neck Surg. 2002;128:150---5.
9.PiltcherOB,TeixeiraVN,deOliveiraMW,ScattolinI,Piltcher SL.Theprevalenceofneurosensorialhearinglossamongcystic fibrosispatientsfromHospitaldeClinicasdePortoAlegre.IntJ PediatrOtorhinolaryngol.2003;67:939---41.
10.ChengAG,JohnstonPR,LuzJ,UluerA,FligorB,LicameliGR, etal.Sensorineuralhearinglossinpatientswithcysticfibrosis. OtolaryngolHeadNeckSurg.2009;141:86---90.
11.Jacob LCB, Aguiar FP, Tomiasi AA, Tschoeke SN,Bittencourt RF.Auditorymonitoringinototoxicity.BrazJOtorhinolaryngol. 2006;72:836---44.
12.Konrad-MartinD,WilmingtonDJ,GordonJS,ReavisKM,Fausti SA.Audiologicalmanagementofpatientsreceiving aminoglyco-sideantibiotics.VoltaRev.2005;105:229---50.
13.AmericanAcademyofAudiology[Internet].Positionstatement and clinical practice guidelines; 2009. Available at: http:// www.audiology.org/resources/documentlibrary/documents/ otomonpositionguideline.pdf[quotedOctober2009].
14.DavisJM,ElfenbeinJ, SchumR, Bentler RA. Effectsof mild and moderate hearing impairments on language, education and psychosocialbehaviorofchildren.JSpeechHear Disord. 1986;51:53---62.
15.Fausti SA, Rappaport BZ, Schechter MA, Frey RH, Ward TT, BrummettRE.Detectionofaminoglycosideototoxicityby high-frequency auditoryevaluation: selected cases studies. Am J Otolaryngol.1984;5:177---82.
16.KlagenbergKF,OlivaFC,Gonc¸alvesCGO,LacerdaABM,Garofani VG,ZeigelboimBS.Audiometriadealtasfrequênciasno diag-nósticocomplementaremaudiologia:umarevisãodaliteratura nacional.RevSocBrasFonoaudiol.2011;16:109---14.
17.FaustiSA,HenryJA,SchafferHI,OlsonDJ,FreyRH,McDonald WJ.High-frequencyaudiometricmonitoringforearlydetection ofaminoglycosideototoxicity.JInfectDis.1992;165:1026---32. 18.PedersenSS,JensenT,OsterhammelD,OsterhammelP.
Cumu-lative and acute toxicity of repeated high-dose tobramycin treatment in cystic fibrosis. Antimicrob Agents Chemother. 1987;31:594---9.
19.McRorieTI,BossoJ,RandolphL.Aminoglycosideototoxicityin cysticfibrosis.AmJDisChild.1989;143:1328---32.
20.MulheranM,DeggC,BurrS,MorganDW,StableforthDE. Occur-rence and risk of cochleotoxicity in cystic fibrosis patients
receivingrepeatedhigh-doseaminoglycosidetherapy. Antimi-crobAgentsChemother.2001;45:2502---9.
21.MulheranM,Hyman-TaylorP,TanKH,LewisS,StableforthD, KnoxA,etal.Absenceofcochleotoxicitymeasuredbystandard and high-frequency pure tone audiometryin a trial ofonce versusthree-times-dailytobramycinincysticfibrosispatients. AntimicrobAgentsChemother.2006;50:2293---9.
22.Toral-Marti˜nón R, Shkurovich-Bialik P, Collado-Corona MA, Mora-Maga˜na I, Goldgrub-Listopad S, Shkurovich-Zaslavsky M. Distortion product otoacoustic emissions test is useful in children undergoing cisplatin treatment. Arch Med Res. 2003;34:205---8.
23.KnightKR, KraemerDF,WinterC,Neuwelt EA.Earlychanges in auditory function as a result of platinum chemotherapy: useof extended high-frequency audiometry and evoked dis-tortionproductotoacousticemissions.JClinOncol.2007;25: 1190---5.
24.MulheranM,DeggC.ComparisonofdistortionproductOAE gen-erationbetweenapatientgrouprequiringfrequentgentamicin therapyandcontrolsubjects.BrJAudiol.1997;31:5---9. 25.OzturanO,JergerJ,LewH,LynchGR.Monitoringofcisplatin
ototoxicitybydistortion-productotoacousticemissions.Auris NasusLarynx.1996;23:147---51.
26.LittmanTA,MagruderA,StrotherDR.Monitoringandpredicting ototoxic damage using distortion-product otoacoustic emis-sions:pediatriccasestudy.JAmAcadAudiol.1998;9:257---62. 27.GarciaAP,Iório MCM, PetrilliAS. Monitoramento daaudic¸ão
de pacientes expostos à cisplatina. Braz J Otorhinolaryngol. 2003;69:215---21.
28.Reavis KM, Phillips DS, Fausti SA, Gordon JS,Helt WJ, Wil-mington D, et al. Factors affecting sensitivity of distortion productotoacousticemissionstoototoxichearingloss.EarHear. 2008;29:875---93.
29.Abujamra AL, Escosteguy JR, Dall’Igna C, Manica D, Cigana LF, Coradini P, et al. The use of high-frequency audiome-try increases the diagnosis of asymptomatic hearing loss in pediatricpatientstreatedwithcisplatin-basedchemotherapy. PediatrBloodCancer.2013;60:474---8.
30.JergerJ.Clinicalexperiencewithimpedanceaudiometry.Arch Otolaryngol.1970;92:311---24.
31.PedaliniMEB,SanchezTG,D’AntonioA,D’AntonioW,Balbani A,HachiyaA,etal.Médiadoslimiarestonaisnaaudiometriade altafrequênciaemindivíduosnormaisde4a60anos.Pró-Fono. 2000;12:17---20.
32.SahyebDR,CostaFilhoOA,AlvarengaKF.Audiometriadealta frequência:estudocomindivíduosaudiologicamentenormais. BrazJOtorhinolaryngol.2003;69:93---9.
33.SáLCB,LimaMAMT,TomitaS,FrotaSMMC,SantosGA,Garcia TR.Avaliac¸ãodoslimiaresdeaudibilidadedasaltas frequên-ciasemindivíduosentre18e29semqueixasotológicas.BrazJ Otorhinolaryngol.2007;73:215---25.
34.CarvalloRMM,KogaMC,CarvalhoM,IshidaIM.Limiares audi-tivosparaaltasfrequênciasemadultossem queixaauditiva. ActaORL.2007;25:62---6.
35.AzevedoMF.Emissõesotoacústicas.In:FigueiredoMS,editor. Conhecimentosessenciaisparaentenderbememissões otoacús-ticaseBERA.SãoJosédosCampos:Pulso;2003.p.35---84. 36.Chauhan RS, Saxena RK, Varshey S. The role of
ultrahigh-frequency audiometry in the early detection of systemic drug-induced hearing loss. Ear Nose Throat J. 2011;90: 218---22.
37.BeahanN,KeiJ,DriscollC,CharlesB,KhanA.High-frequency pure-toneaudiometryinchildren:atest---retestreliabilitystudy relativeototoxiccriteria.EarHear.2012;33:104---11.
39.Leigh-Paffenroth E, Reavis KM, Gordon JS, Dunckley KT, Fausti SA, Konrad-Martin D. Objective measures of oto-toxicity. Perspect Hear Hear Disord Res Diagn. 2005;9: 10---6.
40.WeigertLL,PiltcherOB,ProcianoyEFA,BussCH,Menna-Barreto SS. Avaliac¸ão do uso da audiometria em frequências ultra-altasempacientessubmetidosaousodeototóxicos.BrasMed. 2013;50:264---73.
41.Martins LMN, Camargos PAM, Becker HMG, Becker CG, GuimarãesHMG.Hearingloss incysticfibrosis. IntJPediatr Otorhinolaryngol.2010;74:469---73.
42.Al-MalkyG,SuriR,DawsonSJ,SirimannaT,KempD. Aminogly-cosideantibioticscochleotoxicity inpaediatriccysticfibrosis (CF)patients:astudyusingextendedhigh-frequency audiome-tryanddistortionproductotoacousticemissions.IntJAudiol. 2011;50:112---22.
43.KatbamnaB, Homnick DN, Marks JH. Contralateral suppres-sion of distortion product otoacoustic emissions in children withcysticfibrosis:effectsoftobramycin.JAmAcadAudiol. 1998;9:172---8.
44.Katbamna B, Homnick DN, Marks JH. Effects of chronic tobramycin treatment on distortion product emissions. Ear Hear.1999;20:393---402.
45.ArnoldDJ,Lonsbury-MartinBL,MartinGK.High-frequency hear-inginfluenceslower-frequencydistortion-productotoacoustic emissions.ArchOtolaryngolHeadNeckSurg.1999;125:215---22. 46.MooreRD,SmithCR,LietmanPS.Riskfactorsforthe develop-mentofauditorytoxicityinpatientsreceivingaminoglycosides. JInfectDis.1984;149:23---30.
47.GovaertsPJ,ClaesJ,VanDeHeyningPH,JorensPG,MarquetG, DeBroeME.Aminoglycoside-inducedototoxicity.ToxicolLett. 1990;52:227---51.
48.TanKHV,MulheranM,KnoxAJ,SmythAR.Aminoglycoside pre-scribingandsurveillanceincysticfibrosis.AmJRespirCritCare Med.2003;167:819---23.
49.de Groot R, Smith AL. Antibiotic pharmacokinetics incystic fibrosis differences and clinical significance. Clin Pharma-cokinet.1987;13:228---53.