www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
A
prospective
study
of
138
arthroscopies
of
the
temporomandibular
joint
夽
,
夽夽
Paulo
Alexandre
da
Silva
a,∗,
Maria
Teresa
de
Fatima
Fernandes
Lopes
b,
Fernando
Silva
Freire
baDepartmentofOralandMaxillofacialSurgeryandTraumatology(OMFST),MedicalCenter,HospitalVivalleSãoJosédosCampos,
SãoJosédosCampos,SP,Brazil
bDepartamentofOralandMaxillofacialSurgeryandTraumatology,InstitutoEducacionaldeCiênciasdaSaúde(IECS
Facsete/Ciodonto),SeteLagoas,MG,Brazil
Received25August2013;accepted31August2014 Availableonline9June2015
KEYWORDS
Arthroscopy; Temporomandibular joint;
Temporomandibular jointdisorders; Temporomandibular jointdysfunction syndrome;
Temporomandibular articulardisk
Abstract
Introduction:Internalderangements(ID)ofthetemporomandibular joint(TMJ)havea mul-tifactorial etiology and are most often treated conservatively by splints, physical therapy andmedications. Onlyin2---5%ofcasesarethetreatmentsurgical,eitherbyarthroscopyor arthrotomy.
Objective:Toevaluateimprovementofmouthopening,painreliefduringfunction,positionof thearticulardiskandcomplicationsfollowingArthroscopicLyseandLavage(ALL).
Methods:Aprospectivestudyof78patients(138TMJs)withTMJID,5malesand73females, meanage29.7years,treatedbetweenJanuary2010andApril2013,whowererefractoryto conservativetreatment,hadlimitedmouthopeningandpainlocalizedtotheTMJduring func-tion,andwhoweresubmittedtoTMJALLandfollowedforaperiodof12months,withperiodic reviews.
Results:ALLwaseffectivein93.6%ofcases,with85.3%experiencingimprovementinmouth openingand91.2%inpainreductionduringfunction,63%improvementindiskpositionanda rateofcomplicationsof6.2%.
Conclusion:InthisstudytheALLexhibitedahighrateofsuccesswithlowmorbidityininternal derangementsoftheTMJ.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:daSilvaPA,LopesMTFF,FreireFS.Aprospectivestudyof138arthroscopiesofthetemporomandibularjoint.
BrazJOtorhinolaryngol.2015;81:352---7.
夽夽Institution:IECSInstitutoEducacionaldeCiênciasdaSaúde,SeteLagoas,MG,Brazil.
∗Correspondingauthor.
E-mail:[email protected](P.A.daSilva).
http://dx.doi.org/10.1016/j.bjorl.2014.08.021
PALAVRAS-CHAVE
Artroscopia; Articulac¸ão
temporomandibular; Transtornosda articulac¸ão
temporomandibular; Discodaarticulac¸ão temporomandibular; Síndromeda disfunc¸ãoda articulac¸ão
temporomandibular
Estudoprospectivode138artroscopiasdaarticulac¸ãotemporomandibular
Resumo
Introduc¸ão: Osdesarranjos internos (DI)daarticulac¸ão temporomandibular (ATM),possuem etiologiamultifatorial, sendotratados namaioriadas vezesde formaconservadora através splints,fisioterapiaemedicamentos.Apenas2%a5%doscasostemindicac¸ãocirúrgica,seja atravésdeartroscopiaouartrotomia.
Objetivo: Avaliarmelhoradaaberturabucal,melhoradador,posicionamentododiscoarticular ecomplicac¸õespósLiseeLavagemArtroscópica(ALL).
Método: Estudoprospectivocomumaseriede78pacientes(138ATMs)comDIdaATM,sendo5 homense73mulheres,commédiaetáriade29,7anos,atendidosentrejaneirode2010eabril de2013,refratáriosaotratamentoconservador,apresentandolimitac¸ãodeaberturabucale dorlocalizadaem ATMem func¸ão,sendosubmetidos àALL daATMeacompanhadosporum períodode12meses,comavaliac¸õesperiódicas.
Resultados: AALLfoieficienteem93,6%doscasosestudados,com85,3%melhoranaabertura bucale91,2%nareduc¸ãodadoremfunc¸ão,63%demelhoranaposic¸ãodiscalemRMdecontrole eíndice6,2%decomplicac¸ões.
Conclusão:NopresenteestudoaALLmostrou-seumtratamentocomumaltoíndicedesucesso, combaixamorbidade,nosdesarranjosinternosdaATM.
©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Internaldisorders(ID)ofthetemporomandibularjoint(TMJ) haveamultifactorial etiology,andtheirtreatment consti-tutesasignificantchallengeforcliniciansandsurgeons.For years,thesedisordersweretreatedconservatively,mostly by the use of splints and anti-inflammatory agents. Sur-gical treatment is indicated in only 2---5% of cases, and in most cases it is performed by arthrotomy. In 1975, Ohnishi1 was the first surgeon to use an arthroscope in
TMJ,when thisauthorstudied itsmovements and arthro-scopicanatomy. Inthe80s, severalauthors2---5 contributed
tothedevelopmentof TMJarthroscopy, withdescriptions of various techniques and an understanding of the inter-nal changes viewedarthroscopically.Fromthe end of the 80stonow, therehasbeen greatprogress inarthroscopy, mainly due to a better quality of magnetic resonance imaging (MRI) studies and also to an understanding of the pathophysiology of ID. Bronstein and Merrill6
corre-latedthestagesofWilkes7withtheirarthroscopicfindings;
NitzanandEtsion8reportedontheinterrelationshipofthe
lubricationprocessandarticulardiskdisplacement;others developedandintroducedseveralarthroscopictechniques, withexcellent results,such asdisksuture,9,10 co-ablation
withradiofrequency,11,12 laserablation,12 druginjection,12
diskfixation,13andeminectomy.14
Arthroscopic Lyseand Lavage(ALL) wasfirstdescribed in theliterature as‘‘Lysis’’by Sanders4 in 1986. In1992,
inamulticenterUSstudy,resultsof4861TJMarthroscopic procedureswerecollected,andamongalltechniques per-formed,85%wereALL.Thus,ALLwasnotedtobethemost frequentlyperformedprocedureinTMJarthroscopyandwas reported tohave a global improvement indexof 91.3%.15
With this technique, fibrosis and adhesions are disrupted by instrumentation through the working cannula, while
maintainingacontinuousflowof0.9%salineorRinger’s solu-tion.Thus,theproductofthebreakdownofadhesionsand alsoitsinflammatorycomponentsareeliminated,promoting abetteranatomicalandphysiologicalconditionand allow-ingbettermobilizationofTMJanddecreasedpain.16Theaim
ofthisstudywastoevaluatethesuccessrateofthe arthro-scopiclysisandlavage(ALL)procedureinpatientswithTMJ internaldisorders,inrelationtoimprovingtheoralopening, decreasingpainsymptoms,articulardiskpositioninginthe post-proceduralMRI,andcomplicationsofthetechnique.
Methods
Table1 RelationshipbetweenpatientsandaffectedTMJs.
Patients Unilateral Bilateral TotalofTMJs
78 24 58 138
Table2 RelationshipbetweenTMJsandWilkesstage.
TMJs WilkesII WilkesIII WilkesIV WilkesV
138 42 57 31 8
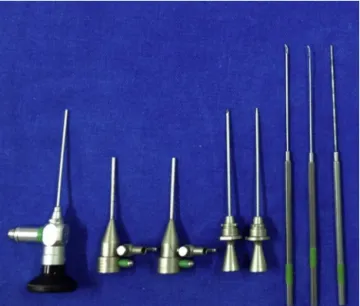
accountinformationobtainedfromhistory,toruleout pos-sibleinvolvementof systemicfactors,suchasrheumatoid arthritisandfemalehormonaldysfunction,amongothers.At theinitialclinicalexamination,patientshadanaverageof 21.2mmofmouthopeningand/orlocalizedpaininfunction (meanVASof6.75,andpositiveforajointloadtest).Among 138ATMsstudied,42wereinWilkesstageII,57inWilkesIII, 31inWilkesIV,and8inWilkesV(Table2).Allpatients under-wentgeneralanesthesiawithnasalintubation.Inallcases, patientsreceivedantibioticprophylaxiswithcephalothin2g atinductionofanesthesia.Inallprocedures,1.9mm, zero-degreeopticaldevice,sleeves,sharpandbluntperforators, adhesionknives,an exploratoryprobe,andabipolar elec-trode(Karl StorzEndoscopy, Tuttlingen,Germany)(Fig.1) were used. ALL was performed with a puncture, sweep and triangulation technique described by McCain et al.17
under irrigation with Ringer’s. Instrumentation was per-formedforremovalofadhesions,synovitiscauterizationand mobilizationofthearticulardisk(Figs.2---5).Attheendof theprocedure,sodiumhyaluronateinfiltration,20mg(TBR Polireumin®Pharma,SãoPaulo,SP,Brazil),wasperformed.
All arthroscopicprocedures were performed by the same professional.Patientswere discharged after 12---24h, and naproxensodium500mg12/12hfor3dayswasprescribed. Patientswereinstructedtomaintainasoftdietfor30days, use a Michigan myorelaxant plate, limit mouth opening, and perform laterality and mandibular protrusion passive exercises during the first 15 days, and return to physical
Figure1 OpticsandinstrumentsusedinALL.
Figure2 ALLbeingperformedwiththeopticaldevicein posi-tion,refluxneedleandtriangulationforinstrumentation.
therapy after this period. Physical therapy and plate use weremaintainedfor6monthspostoperatively.Allpatients were evaluated postoperatively at 24h, 72h, 7 days, 15 days,21daysand30days,andthenmonthly.During follow-up, pain improvement in function (VAS and load testing) andimprovedmouthopeningamplitudewereevaluated.All complications arising fromALL werealso evaluated, with the exceptionof: painat the puncturesite; discrete pos-terioropenbite,andtransientlimitationofmouthopening (sucheventsareexpectedintheearlydays,beinginherent
Figure4 Instrumentationwithknife,withremovalof adhe-sionsintheintermediatezone(betweeneminenceandarticular disk).
Figure5 StraightprobeintoposteriorrecessofTMJ mobiliz-ingthedisktoitsanatomicalposition,afteradhesionremoval.
tothe procedure). A control magnetic resonance imaging (MRI)studyafter6monthswasobtainedfordisk position-ingassessmentinrelationtotheinitialMRI.At6months,in thecaseofpersistenceorworseningoftheclinicalpicture, arthrotomywasindicated.The totalfollow-up ofpatients was12months.
Results
Of 78 enrolled patients, after 6 months of follow-up, 5 (6.4%)didnotobtaina favorableresult,duetopersistent limitation of mouth opening. This represented 9 ATMs (3 WilkesVand6WilkesIV),i.e.,6.52%forall138joints stud-ied.Inthesecases,discopexywithuseofmini-anchorswas
Wilkes II Wilkes III Wilkes IV Wilkes V 0
25 50 75 100
Mouth opening improvement Pain relief
Figure 6 Relationship between means (in percentage) of mouth opening improvement and pain relief, compared to WilkesstagesfoundduringTMJarthroscopy.
performed,obtainingtheresolutionoftheclinicalpicture, withsignificantimprovementinmouthopening.Thesuccess rateofALLwas93.59%consideringall78patientsenrolled; and93.48%when considering all138ATMs treated. Inthe item ‘‘mouth opening improvement’’ and considering all 78 patients, the overall index was85.3%, withvariations inthemeansobtained:68.7%forWilkesVpatients;83.2% forWilkesIV;92.5%forWilkesIII,and96.8% forWilkesII. Thesmallestandthelargestlengthswere36mmand52mm, respectively,withaglobalmeanof45mm.Stillconsidering the78patientsstudied,‘‘improvementofpaininfunction’’ occurredin91.2%, withvariationsinthe meansobtained: 81.9%forWilkesVpatients;89.2%for WilkesIV;95.4%for WilkesIII, and98.3%for WilkesII.The lowest andhighest VASscoreswere6and10,respectively,withaglobalmean of9.2(Fig.6).Aftersixmonths,controlMRIsshowedthat in 63% of cases, there wasimprovement in articular disk position,with itslocation between 11 and 12h (at rest), comparedwithinitialMRIs,wherethediscsweredisplaced. Eleven cases (7.9%) of post-ALL complications in our 138 ATMsoccurred,asfollows:5casesoffluidaccumulationin thesite(3.6%),3casesofhearingfullnessand/orloss(2.2%), 2casesofearcanallacerations(1.4%),and1caseof paral-ysisofthetemporalbranchoffacialnerve(0.7%)(Table3). Allcomplications were transient, not requiring additional treatment.
Discussion
Arthroscopic lysis and lavage has been successfully employedininternaldisorders(ID)ofTMJrefractoryto con-servativetherapywithocclusalsplintsandphysiotherapy.In thisstudy,allpatientswerepreviouslytreatedwithsplints and physiotherapy, and were referred for the procedure because there was persistence of limited mouth opening and/orintra-articularpain.
In the literature, the success rate for improving oral openingandpainsymptomsvary.SandersandBuoncristiani18
describedtheirclinicalexperienceusingALLandobtained excellentresultsin82% oftheirpatients witha maximum inter-incisalopening(MIO)ofnotlessthan40mm,andlittle ornoTMJpain.Indresano19obtaineda73%successrateina
Table3 Post-ALLcomplications.
TMJs Localfluid accumulation
Hearingfullness Earcanallaceration Paralysisofthetemporal branchoffacialnerve
Total
138 3.6% 2.2% 1.4% 0.7% 11(7.9%)
recommendedmovementswithcannulaandblunttrocarin theanterior-posteriordirection, andobtainedareduction ofpainin92%of237patientsundergoingALL;theseauthors alsoreportedimprovementinmouthopeningtogreaterthan 40mmwithMIOin78%.Perrotetal.21 observeddecreased
painandincreasedjointmobilityinaprospectivestudyof76 jointstreatedwithALL; thewholegroupwastreatedwith corticosteroidinjection.Clarketal.22observedareduction
of painin 57% of patients and improvement in the range of mandibular movement in 83%. In a follow-up study of 63patients over4 years,Moore23 concludedthat ALLwas
beneficialin87%ofpatients.Kuritaetal.24reportedan
over-allresponse rate of 86% whenusing ALLfor treatingTMJ internaldisorders.InpatientsundergoingALL,Dimitroulis25
reportedgoodresultsin66%,slightimprovementin18%,and noimprovementin16%.GonzalezGarciaetal.26showedthat
ALLwasaseffectiveassurgicalarthroscopywithrespectto postoperativepainreductionormouthopeningincreaseat anystageofthefollow-upperiod.Kondohetal.27 reported
a80%successratewiththeuseofALLforTMJinternal dis-order.SorelandPiecuch28 reportedalong-termbeneficial
effectofALLforthetreatmentofchronicTMJpain,noting that95%oftheirpatientswhowerefollowedfor4.4years hadnosignificantcomplaintsandhadasignificantincrease inmouthopening.Someauthorsobservedthatthesuccess rateofALLdependsontheWilkesstagefortheTMJ. Bron-steinandMerrill6observed96%ofsuccessfor stageII,83%
forstageIII,88%for stageIV,and63%for stageV.Smolka andIizuka29observedaaveragesuccessrateof86.7%,
ran-gingfrom75% to92.3%according tothestage intowhich theTMJwas.Thesevariationsinresultswerealsoobserved inthepresentstudy,withvariationsaccordingtotheWilkes stage,butglobalmeansthatwereconsistentwiththe stud-iesreviewedduringthestudyperiod.Inthepresentstudy, we didnot recommendrepeatedarthroscopy for patients whose ALL failed by the clinical criteria, because of the largedisplacementandmoreadvancedprocessof degenera-tionofthediscs(WilkesIVandV).Instead,weoptedforan arthrotomyanddiscopexywithmini-anchors,although we agreethat,insomecases,oneshouldconsiderundertaking arepeatarthroscopybeforethisarthrotomy,assuggestedin thestudybyAbd-Ul-Salametal.30Inourstudy,weobserved
in the control RMs a new disk positioning, closer to its anatomicalposition.Thisnewarticulardiskpositionafter theALLprocedurewasalsoobservedbyClarketal.31;Moses
andTopper32believethatthisnewarticulardiskpositionis
notrelatedtoitsrepositioning,butsecondarytodisk mobi-lizationandtotheremovalofadhesionsandinflammatory degenerativeproducts.
Withrespecttocomplications,Tsuyamaetal.33
experi-enced10.3%in301casesofALL; 8.6%ofthesecaseswere otologiccomplicationsand1.7%werelesionsofthe trigem-inalandfacialcranialnerves.Theseauthorsconcludedthat ahighlevelofunderstanding oftheregionalanatomywill
help in reducing complications associated with the com-pletion of ALL. Based on10 yearsof clinical experience, Carlsetal.34 reportedacomplicationrateof 1.77%in451
TMJarthroscopiesin373patients.Thesecomplicationswere transient and mainly related to V and VII cranial nerves. Ina studyof2034 patients,Zhangetal.35 observeda low
rate of complications, namely: 5 bleedings, 5 neuroprax-ias,3instrumentbreakage,2foreignbodyreactionsand2 tympanicmembraneperforations.Gonzalez-Garciaetal.36
observed1.34%ofcomplications,asfollows:earcanal lac-eration, auriculotemporalnerve paresthesias,facialnerve paralysis and impaired visual acuity --- all of them being transient complications. Severalother complicationshave beenreportedintheliterature,suchasinfections,37
arteri-ovenousfistulas,38pseudoaneurysms,39bradycardias40,41and
asystoles,42 all being very rare. In this study, our rate of
complicationswassituatedwithintherangeobservedinthe literature,andalloccurrencesweretransient,notrequiring additionaltreatment.
Conclusion
Lysisandarthroscopiclavage(ALL) isa minimallyinvasive treatment,withefficientresultsinpatientswithTMJ inter-naldisordersrefractorytoconservativetherapy.ALLresults in asignificant improvement inthe rangeof mouth open-ing,decreasespaininfunctionandimprovesarticulardisk position.Inaddition,thisprocedurecarriesalow complica-tionrate.Therefore,ALLisasafeprocedureinthehandsof surgeonswhohavemasteredthetechnique.Furtherstudies areneeded,includingalong-termfollow-up,toconsolidate theresults.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.OhnishiM.Arthroscopyofthetemporomandibularjoint.JJpn Stomatol.1975;42:203---7.
2.Murakami K, Ito I. Arthroscopy of the temporomandibular joint.Arthroscopicanatomyandarthroscopicapproachesinthe humancadaver.Arthroscopy.1981;6:1---13.
3.MurakamiK,HoshinoK.Regionalanatomic nomenclatureand arthroscopic terminology in the human temporomandibular joints.OkamimasFoliaAnatJpn.1982;58:745---60.
4.Sanders B. Arthroscopic surgery of the temporomandibular joint:treatmentofinternalderangementwithpersistentclosed lock.OralSurgOralMedOralPathol.1986;62:361---72. 5.McCainJP.Arthroscopyofthehumantemporomandibularjoint.
6.Bronstein SL, Merrill RG. Clinical staging for TMJ internal derangement:applicationtoarthroscopy.JCraniomandib Dis-ord.1992;6:7.
7.WilkesCH. Internalderangementsofthetemporomandibular joint.Pathologicalvariations.ArchOtolaryngolHeadNeckSurg. 1989;115:469---77.
8.NitzanDW,EtsionI.Adhesiveforce:theunderlyingcauseofthe discanchoragetothefossaand/oreminenceinthe temporo-mandibularjoint---anewconcept.IntJOralMaxillofacSurg. 2002;31:94---9.
9.McCainJP,PodraskyAE,ZabiegalskiNA.Arthroscopicdisc repo-sitioningandsuturing:apreliminaryreport.JOralMaxillofac Surg.1992;50:568---79.
10.Yang C, Cai XY, Chen MJ, Zhang SY. New arthroscopic disc repositioningandsuturingtechniquefortreatingananteriorly displaceddiscofthetemporomandibularjoint:PartI--- Tech-niqueintrodution.IntJOralMaxillofacSurg.2012;41:1058---63. 11.Chen MJ, Yang C, Zhang SY, Cai XY. Use of coblation in arthroscopic surgeryof thetemporomandibularjoint. JOral MaxillofacSurg.2010;68:2085---91.
12.McCainJP,HossameldinRH.Advancedarthroscopyofthe tem-poromandibularjoint.AtlasOralMaxillofacSurgClinNorthAm. 2011;19:145---67.
13.Goizueta-AdameCC,Pastor-ZuazagaD,OrtsBa˜nónJE. Arthro-scopicdisc fixation to thecondylar head. Useof resorbable pinsforinternalderangementofthetemporomandibularjoint (stageII---IV).Preliminaryreportof34joints.JCraniomaxillofac Surg.2013,http://dx.doi.org/10.1016/j.jcms.2013.05.023. 14.Undt G. Temporomandibular joint eminectomy for
recur-rent dislocation. Atlas Oral Maxillofac Surg Clin North Am. 2011;19:189---206.
15.McCain JP, Sanders B, Koslin M. Temporomandibular joint arthroscopy:a6yearsmulticenterretrospectivestudyof4.831 joints.JOralMaxillofacSurg.1992;50:926.
16.González-GarcíaR,Gil-Díez UsandizagaJL,Rodríguez-Campo FJ.Anatomy and lysisand lavage of thetemporomandibular joint.AtlasOralMaxillofacSurgClinNorthAm.2011;19:131---44. 17.McCainJP,delaRuaH,LeBlancWG.Puncturetechniqueand portalsofentryfordiagnosticandoperativearthroscopyofthe temporomandibularjoint.Arthroscopy.1991;7:221---32. 18.SandersB,BuoncristianiR.Diagnosticandsurgicalarthroscopy
ofthetemporomandibularjoint:clinicalexperiencewith137 procedures over a 2-year period. J Craniomandib Disord. 1987;1:202---13.
19.IndresanoAT.Arthroscopicsurgeryofthetemporomandibular joint:reportof64patientswithlong-termfollow-up.JOral MaxillofacSurg.1989;47:439---41.
20.MosesJJ,SartorisD,GlassR,TanakaT, PokerI.Theeffects of arthroscopic lysis and lavage of the superior joint space on TMJ disc position and mobility. J Oral Maxillofac Surg. 1989;47:674---8.
21.PerrotDH,AlborziA,KabanLB.Aprospectiveevaluationofthe effectivenessoftemporomandibularjoint arthroscopy.JOral MaxillofacSurg.1990;48:1029---32.
22.ClarkGT,SandersB,BertolamiCH.Advancesindiagnosticand surgicalarthroscopyofthetemporomandibularjoint. Philadel-phia:WBSaunders;1993.
23.MooreLJ.Arthroscopicsurgeryforthetreatmentofrestrictive temporomandibularjoint disease. A prospective longitudinal study.In:ClarkG,SandersB,BertolaniC,editors.Advancesin diagnosticandsurgicalarthroscopyofthetemporomandibular joint.Philadelphia:WBSaunders;1993.p.35---40.
24.KuritaK, Goss AN, Ogi N. Correlation between preoperative mouthopeningandsurgicaloutcomeafterarthroscopiclysisand lavageinpatientswithdiscdisplacementwithoutreduction.J OralMaxillofacSurg.1998;56:1394---7.
25.DimitroulisG.Areviewof56casesofchronicclosedlocktreated withtemporomandibular joint arthroscopy.J OralMaxillofac Surg.2002;60:519---24.
26.González-Garcia R, Rodríguez-Campo FJ. Arthroscopic lysis and lavage versus operative arthroscopy in the outcome of temporomandibular joint internal derangement: a compara-tive study based on Wilkes stages. J Oral Maxillofac Surg. 2011;69:2513---24.
27.Kondoh T, Dolwick MF, Hamada Y, Seto K. Visually guided irrigationforpatientswithsymptomaticinternalderangement ofthetemporomandibularjoint:apreliminaryreport.OralSurg OralMedOralPatholOralRadiolEndodontol.2003;95:544---51. 28.SorelB,PiecuchJF. Long-termevaluationfollowing temporo-mandibularjointarthroscopywithlysisandlavage.IntJOral MaxillofacSurg.2000;29:259---63.
29.Smolka W, Iizuka T. Arthroscopic lysis and lavage in differ-entstagesofinternalderangementofthetemporomandibular joint: correlation of preoperative staging to arthroscopic findings and treatment outcome. J Oral Maxillofac Surg. 2005;63:471---8.
30.Abd-Ul-Salam H, Weinberg S, Kryshtalskyj B. The incidence of reoperation after temporomandibular joint arthroscopy surgery:aretrospectivestudyof450consecutivejoints.Oral Surg OralMed OralPathol OralRadiol Endodontol. 2002;93: 408.
31.ClarkGT,SandersB,BertolaniCH.Advancesindiagnosticand surgicalarthroscopyofthetemporomandibularjoint. Philadel-phia:WBSaunders;1993.
32.MosesJJ,TopperDC.Afunctionalapproachtothetreatment of temporomandibular joint internal derangement. J Cran-iomandibDisord.1991;5:19---27.
33.TsuyamaM,KondobT,SetoK,FukudaJ.Complicationsof tem-poromandibularjointarthroscopy:aretrospective analysisof 301lysisandlavageproceduresperformedusingthe triangula-tiontechnique.JOralMaxillofacSurg.2000;58:500---5. 34.CarlsFR,EngelkeW, LocherMC,SailerHF.Complications
fol-lowingarthroscopy ofthe temporomandibularjoint: analysis coveringa10-yearperiod(451arthroscopies).J Craniomaxillo-facSurg.1996;24:12---5.
35.ZhangS,YangC,CaiX,LiuX,HuangD,XieQ,etal. Preven-tionandtreatmentfortherarecomplicationsofarthroscopic surgeryinthetemporomandibularjoint.JOralMaxillofacSurg. 2011;69:347---53.
36.González-García R, Rodríguez-Campo FJ, Escorial-Hernández V, Mu˜noz-Guerra MF, Sastre-Pérez J, Naval-Gías L, et al. Complicationsoftemporomandibularjointarthroscopy:a ret-rospectiveanalyticstudyof670arthroscopicprocedures.JOral MaxillofacSurg.2006;64:1587---91.
37.McCain JP, Zabiegalski NA, Levine RL. Joint infection as a complicationoftemporomandibularjointarthroscopy: acase report.JOralMaxillofacSurg.1993;51:1389---92.
38.MosesJJ,TopperDC.Arteriovenousfistula:anunusual compli-cation associatedwitharthroscopic temporomandibularjoint surgery.JOralMaxillofacSurg.1990;48:1220---2.
39.KornbrotA,ShawAS,TooheyMR.Pseudoaneurysmasa compli-cation ofarthroscopy: acasereport.JOralMaxillofac Surg. 1991;49:1226---8.
40.RobertsRS,BestJA,ShapiroRD.Trigeminocardiacreflexduring temporomandibularjointarthroscopy:reportofacase.JOral MaxillofacSurg.1999;57:854---6.
41.Gomes TM, Van Gilder JW. Reflex bradycardia during TMJ arthroscopy: case report. J Oral Maxillofac Surg. 1991;49:543---4.