REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
The
effect
of
different
doses
of
esmolol
on
hemodynamic,
bispectral
index
and
movement
response
during
orotracheal
intubation:
prospective,
randomized,
double-blind
study
Mensure
Yılmaz
C
¸akırgöz
a,∗,
Aydın
Tas
¸dö˘
gen
b,
C
¸imen
Olguner
b,
Hülya
Korkmaz
b,
Ertu˘
grul
Ö˘
gün
b,
Burak
Küc
¸ükebe
b,
Esra
Duran
baDepartmentofAnesthesiologyandReanimation,OkmeydaniTrainingandResearchHospital,Istanbul,Turkey bDepartmentofAnesthesiologyandReanimation,DokuzEylülUniversity,SchoolofMedicine,Izmir,Turkey
Received12August2013;accepted2September2013 Availableonline30October2013
KEYWORDS
Depthofanesthesia; Propofol;
Intubation; Bispectralindex; Esmolol
Abstract
Objective: Aprospective,randomizedanddouble-blindstudywasplannedtoidentifythe
opti-mum dose of esmolol infusionto suppress the increase in bispectralindex values andthe
movementandhemodynamicresponsestotrachealintubation.
Materialsandmethods: Onehundredandtwentypatientswererandomlyallocatedtooneof
threegroupsinadouble-blindfashion.2.5mgkg−1propofolwasadministeredforanesthesia
induction.Afterlossofconsciousness,andbefore administrationof0.6mgkg−1rocuronium,
atourniquetwasappliedtoonearmandinflatedto50mmHggreaterthansystolicpressure.
Thepatientsweredividedinto3groups;1mgkg−1h−1esmololwasgivenastheloadingdose
and inGroup Es50 50gkg−1min−1,in Group Es150 150gkg−1min−1,and inGroup Es250
250gkg−1min−1esmololinfusionwasstarted.Fiveminutesaftertheesmololhasbeenbegun,
thetracheawasintubated;grossmovementwithinthefirstminuteafterorotrachealintubation
wasrecorded.
Results:IncidenceofmovementresponseandtheBISmaxvalueswerecomparableinGroup
Es250andGroupEs150,butthesevaluesweresignificantlyhigherinGroupEs50thaninthe
othertwogroups.Inallthreegroupsinthe1stminuteaftertrachealintubationheartrateand
mean arterialpressure weresignificantlyhighercompared tovaluesfrombefore intubation
(p<0.05).Inthestudyperiodtherewasnosignificantdifferencebetweenthegroupsinterms
ofheartrateandmeanarterialpressure.
Conclusion: Inclinicalpractisewebelievethatafter1mgkg−1loadingdose,150gkg−1min−1
ivesmololdoseissufficienttosuppressresponsestotrachealintubationwithoutincreasingside
effects.
© 2013SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights
reserved.
∗Correspondingauthor.
E-mail:[email protected](M.Y.C¸akırgöz).
0104-0014/$–seefrontmatter©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Profundidadeda anestesia; Propofol; Intubac¸ão; Índicebispectral; Esmolol
Efeitodediferentesdosesdeesmololsobrearespostahemodinâmica,BISeresposta demovimentoduranteaintubac¸ãoorotraqueal:estudoprospectivo,randômicoe duplo-cego
Resumo
Objetivo:Estudoprospectivo,randômicoeduplo-cegoplanejadoparaidentificaradoseideal
deperfusãodeesmololparasuprimiroaumentodosvaloresdoBISeosmovimentoserespostas
hemodinâmicasàintubac¸ãotraqueal.
Materiaisemétodos:120 pacientes foram randomicamente alocados um dos três grupos,
usandoométododuplo-cego.Propofol(2,5mgkg−1)foiadministradoparainduc¸ãodaanestesia.
Apósaperdadaconsciênciaeantesdaadministrac¸ãoderocurônio(0,6mgkg−1),umtorniquete
foiaplicadoaumbrac¸oeinsufladoa50mmHgacimadapressãosistólica.Ospacientesforam
divididosemtrêsgrupos;umadosede1mgkg−1h−1deesmololfoiadministradacomocarga
eperfusão de50gkg−1min−1 deesmololfoi iniciada noGrupo ES50,150gkg−1min−1 no
GrupoEs150e250gkg−1min−1noGrupoES250.Cincominutosapósoiníciodaperfusão,a
traqueiafoiintubada;ototaldemovimentosnoprimeirominutoapósaintubac¸ãoorotraqueal
foiregistrado.
Resultados: AincidênciadarespostademovimentoseosvaloresmáximosdeBISforam
com-paráveisnosgruposES250eEs150,masessesvaloresforamsignificativamentemaiselevados
noGrupoES50quenosoutrosdoisgrupos.Nostrêsgrupos,osvaloresdefrequênciacardíaca
epressãoarterialmédiaforamsignificativamentemaioresnoprimeirominutopós-intubac¸ão,
comparados aosvalores pré-intubac¸ão(p<0,05). Nãohouvediferenc¸a significativaentreos
gruposemrelac¸ãoàfrequênciacardíacaepressãoarterialmédiaduranteoperíododeestudo.
Conclusão:Napráticaclínica,acreditamosqueapósumadosecomcargade1mgkg−1,uma
dose de 150gkg−1min−1 de esmolol IV ésuficiente para suprimir a respostaà intubac¸ão
traquealsemaumentarosefeitoscolaterais.
©2013SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos
direitosreservados.
Introduction
Duringanesthesiainductiontrachealintubationisoneofthe mostintensivenoxiousstimuliandcaninducehemodynamic andmovementresponsesandincreasethebispectralindex (BIS).1---3Hemodynamicchangesduetotrachealintubation,
similartochangesduetoothersurgery-relatedstimulisuch asanesthesiaandskin incisions,areoftentransient. How-ever,inpatientswithcoronaryarterydisease,hypertension (HT)orwithahistoryofcerebrovasculardisease,apossible increaseinhemodynamicparametersmaycausemyocardial ischemia,arrhythmia,infarctionorcerebralbleeding.1,2The
closerelationshipoftachycardiacheartrate(HR)to myocar-dialischemiahassuggestedtheuseof-adrenergicreceptor blockersfor thesuppressionofthehemodynamicresponse totrachealintubation.3---5
DuringanesthesiaprimarilyforthetreatmentofHTand tachycardia 1 adrenoreceptor antagonists are indicated,
whichhave been proven in clinical studies tohave a role inpain modulation.6---13 Whilethe mechanism is unknown,
esmololinfusionisknowntosuppresstheBISincreaseand movementresponselinkedtotrachealintubationcompared toplacebo.14,15 Howevernostudy was found onthe
rela-tionshipbetweentheeffectsofesmololatdifferentinfusion doses.Thehypothesisofthisstudyisthattheresponsesto trachealintubationofincreasedmovementandBISwillbe suppressedduetotheantinociceptiveeffectofesmololina dose-linkedfashion,causingareductioninBISincreaseand movementaftertrachealintubation.Totestthishypothesis
and identify the optimum infusion dose to suppress BIS increaseandmovementresponse,alongwithhemodynamic response,totrachealintubation,aprospective,randomized anddouble-blindstudywasdesigned.
Methods
AfterreceivingDokuzEylülUniversity,FacultyofMedicine ClinicalTrialsLocalEthicsCommitteeapprovalandinformed patientconsentthisprospective,randomized,double-blind study was completed. One hundred and twenty adult patientsinASAI---IIriskgroups,betweentheagesof18and 65,undergoingelectivesurgery,apartfromhead,neckand cardiacsurgery,wereenrolledinthestudy.
Patients with predicted difficult intubation or airway management, body mass index>30kg/m2, HR<60beats
min−1, systolic arterial pressure (SAP)<100mmHg,
car-diacdiseases,diabetesmellitus,renalfailure,liverfailure, COPD,asthma, reactive airwaydisease, symptomatic gas-troesophageal reflux, patients with neuropsychiatric or neurological diseases, pregnant and lactating patients, patients with a history of use of opioids, tricyclic antidepressants, benzodiazepines, anticonvulsants, cloni-dine,-adrenergicreceptorblockers,oralcoholabuse,and patientswithahistoryofallergicreactiontothestudydrugs wereexcluded.
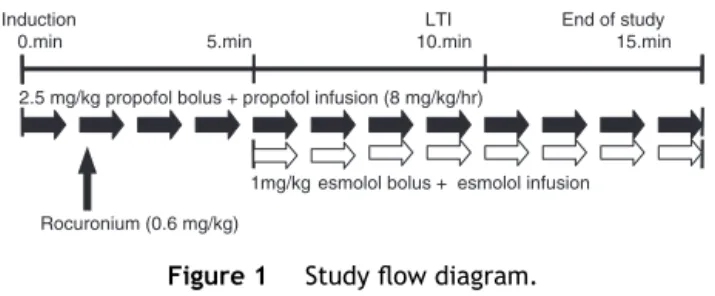
Induction LTI End of study 0.min 5.min 10.min 15.min
2.5 mg/kg propofol bolus + propofol infusion (8 mg/kg/hr)
1mg/kg esmolol bolus + esmolol infusion
Rocuronium (0.6 mg/kg)
Figure1 Studyflowdiagram.
accesscannulaopening.Afterbeingtakentotheoperating table6L/minoxygenwasadministeredthroughamask. In allpatients,non-invasivebloodpressure,electrocardiogram (ECG), pulse oximetry, andesophageal temperature after intubation were monitored. Baseline values for HR, non-invasivemeanarterialpressure(MAP)andperipheraloxygen saturation (SpO2) were recorded.After standard
monitor-ing,patientsweremonitoredwiththeA-2000BISXPdevice (AspectMedicalSystems,Newton,MA,USA).Measured con-trol BIS values were recorded after contact testing was completed.
After pre-oxygenationtoinduce anesthesia2.5mgkg−1
propofol(1%PropofolR,Fresenius,Austria)wasappliedfor 20s and8mgkg−1h−1 propofol infusionwasstarted. After
loss of eyelash reflex in patients, manual end-tidal CO2
(ETCO2)35---40mmHgwasmaintainedbyinhalationof100%
O2throughthemask(Fig.1).Movementresponsetotracheal
intubationwasassessedbytheisolatedforearmtechnique. Forthispurpose,afterlossofconsciousness,thecuffonthe armwithout theIVwasinflated. Aftersystolicblood pres-sureof50mmHgwasreached,rocuronium0.6mgkg−1dose
wasgivenformusclerelaxation.16After5minofinfusionof
propofol,allpatientsweregiven1mgkg−1 esmolol
(Brevi-blocREczacıbas¸ı,Baxter, USA) loadingdosein 15mL total volume0.9%NaClsolution.Patientswererandomly(sealed envelopemethod)allocatedtothreegroupsandafter1min, study medicationwasadministered byan anesthesiologist awareofthemedicationamount.The dosewascalculated for each patient by a 50mL syringe(10mg/mL)perfusor; Group Es50(n=40) 50mgkg−1min−1 esmolol;Group Es150
(n=40)150mgkg−1min−1esmolol;andGroupEs250(n=40)
250mgkg−1min−1infusionofesmolol.After5minofesmolol
infusion, an anesthesia assistant blind to the amount of studydrugadministeredintubatedthepatients.Five min-utesafterintubationesmololinfusionwasterminated.Inthe studyperiod,anesthesiawasmaintainedwith8mgkg−1h−1
infusionofpropofoland50%air---O2mixture.Attheendof
thestudyperiodanestheticmanagementresponsibleforthe operatingtheater andawareof the amount of anesthetic drugsappliedtothepatientslefttheteam.
Before induction by an anesthesiologist blind to the amountofstudydrug(control),at1st,3rdand5thminute after the start of propofol infusion, and from the start of esmolol infusion to 5min after intubation at minute intervals, HR, MAP, BIS, and SpO2 values were recorded.
After the painful stimulus BIS (difference between BIS
value pre-tracheal intubation and after 5st minute post-trachealintubation)andBISmax(differencebetweenBIS
valuespre-tracheal intubation andmaximum value within 5thminutepost-trachealintubation)valueswererecorded afterintubation.16 The timebetweentheopening ofeach
patient’s mouth andwhen the trachealtube cuffinflated
was defined as the intubation time and was recorded. Repeatedintubationattemptsandpatientsrequiringmore than 30s intubation time were removed from the study. Within1minafterintubationmovementofthepatient’sarm thecuffwasplacedonwasacceptedasapositivevalueand theairsleevewasdepressurized.
During the study period, for hypotension (MAP<60mmHg) first the intravenous infusion of fluid wasincreased and if no improvement within 5min, 5mg of ephedrine (Ephedrine, Haver, Istanbul, Turkey) was administered.Forbradycardia (HR<50beatsmin−1)0.5mg
atropine (atropine sulfate, Haver, Istanbul, Turkey) was implemented. Side effects including hypotension, brady-cardia, arrhythmia, cough, hiccups, increased airway resistance,bronchospasm,etc.,wererecorded.
After1hintherecoveryunitpatientswereasked ques-tionssuchas‘‘Doyourememberanyeventfrombeginning orendoftheoperation?’’todetermineawarenessof intra-operativeeventsandresponseswererecorded.
Poweranalysis
InthestudybyMenigauxetal.14consideringchangeinBIS
values,toreach80%power(˛=0.05)eachgroupshould
con-tainat least 19 patients; Guignard etal.17 revealed that
21patientswererequiredaccordingtomovementresponse findings.Thethreegroupsinthisstudycontainedatotalof 120patients(n=40).
Statistics
DatawerecompiledusingSPSS11.0forWindowsprogram. Todeterminewhether parametershadnormaldistribution the Kolmogorov---Smirnov test and box-plot graphics were completed.Tocomparemeanvaluesbetweenthe3groups one-wayanalysisofvariance(one-wayANOVA)andposthoc Tukey were used.Variations withingroups were analyzed usingthepaired-samplest-test.Non-parametricdatawere analyzedwiththechi-squaretest.p<0.05wasconsidered statisticallysignificant.
Results
Betweenthegroupstherewasnodifferenceintermsofage, bodyweight, height,sex, ASA risk class andthe tracheal intubationduration.Trachealintubationwasperformed in 9---14s(Table1).TwopatientsingroupEs250wereexcluded fromthestudybecauseofHR<60beatsmin−1 after
induc-tion,and1patientwasexcludedduetodifficultintubation. Thedatafromatotalof117patientswereanalyzed.
Table1 DemographicdataandLTIduration(mean±standarddeviation).
Group GroupEs250
(n=38)
GroupEs150
(n=39)
GroupEs50
(n=40)
Age(year) 36.63±10.55 40.12±9.66 37.20±9.01
Weight(kg) 67.16±10.55 68.39±12.23 66.90±10.84
Height(cm) 168.37±7.64 168.36±8.47 166.75±8.62
ASA(I/II) 37/1 39/0 40/0
Sex(F/M) 27/11 27/12 30/10
LTIduration(s) 10.47±1.47 10.89±1.13 10.30±1.02
90
85
80
75
70
65
Baseline Pre e nt
Prp.1.min Prp.3.minPrp.5.minEsm 1.minEsm 2.minEsm 3.minEsm 4.minEsm 5.minEmb 1.minEmb 2.minEmb 3.minEmb 4.minEmb 5.min
Periods
HR (be ats/min)
Group Es250 Group Es150
#: p<0.05 (compared to basal values in Group Es50)
+: p<0.05 (compared to basal values in Group Es150)
*: p<0.05 (compared to basal values in Group Es250)
Group Es50
+
+ + + + * * * *
#
# # # #
# # #
Figure2 ChangesinmeanHRinthegroups.
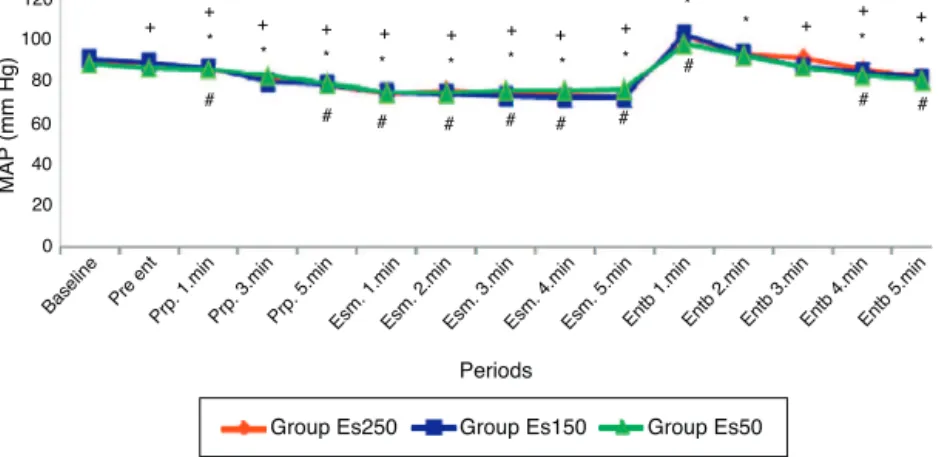
reducedcomparedtobasalvaluesintheperiodbefore tra-chealintubation(p<0.05).Inthe1stminuteaftertracheal intubationinallthreegroups MAPwassignificantlyhigher comparedtovaluesbeforeintubation(p<0.001)(Fig.3).In
thestudyperiodtherewasnosignificantdifferencebetween thegroupsintermsofHRandMAP.
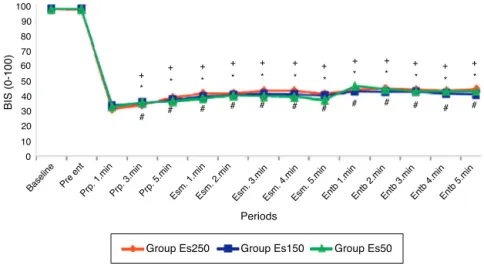
BISvaluesin thefirstminute after induction of propo-fol reached the minimum value (Fig. 4). After tracheal
120
100
80
60
40
20
0
Bas eline
Pre ent
Prp. 1.minPrp. 3.minPrp. 5.min Esm. 1.minEsm. 2.minEsm. 3.minEsm. 4.minEsm. 5.minEntb 1.minEntb 2.minEntb 3.minEntb 4.minEntb 5.min
Periods
MAP
(mm Hg)
Group Es250 Group Es150 Group Es50
+ + + + + + + + + + + +
* * * * * *
*
* *
# # #
# # # # # # #
* * *
#: p<0.05 (compared to basal values in Group Es50) +: p<0.05 (compared to basal values in Group Es150) *: p<0.05 (compared to basal values in Group Es250)
Baseline Pre ent
Prp. 1.minPrp. 3.minPrp. 5.min Esm. 1.minEsm. 2.min Esm. 3.minEsm. 4.minEsm. 5.minEntb 1.minEntb 2.minEntb 3.minEntb 4.minEntb 5.min Periods
Group Es250 Group Es150 Group Es50
100 90 80 70 60 50 40 30 20 10 0
BIS (0-100)
+ + +
+ + + + + + + + +
# # # # # # # # # # # #
* * *
* * * * * * * * *
#: p<0.05 (compared to values after 1st minute propofol in Group Es50) +: p<0.05 (compared to values after 1st minute propofol in Group Es150) *: p<0.05 (compared to values after 1st minute propofol in Group Es250)
Figure4 ChangesinmeanBISvaluesinthegroups.
intubation in the 1st and 2nd minutes BIS values in all three groups showed a significant increase compared to values from before tracheal intubation (p<0.05). There wasno significant difference between all threegroups in terms of BIS values during the study period. When the Groups are compared based on the average value BIS
andBISmaxtherewasnosignificant differencebetween
GroupsEs250andEs150,butboth groups hadsignificantly lowervaluesthanGroupEs50(p<0.05)(Table2). Compar-ingthegroupsinterms ofmovementresponsetotracheal intubation, there was no significant difference between Group Es250(50%) andGroup Es150(56%)but Group Es50 (87.5%)wassignificantlyhigherthantheothertwogroups (Table3).
Nohypotension,bradycardia,arrhythmia,cough,hiccup, bronchospasm,orincreasedairwayresistancewasobserved inanypatient.Noneofthepatientsindicatedany intraop-erativeawarenessinthepostoperativeperiod.BIS,HRand MAPduringthepre-inductionperiodwerealsosimilarinall 3groups.
Discussion
Thisstudyshowsthatinpatientsanesthetizedwithpropofol, esmolol suppressed awareness reactions, shown by move-ment and BIS, to tracheal intubation, in a dose-linked fashion.
Duetothe shortactiveduration ofesmolol, bolus and infusionprotocol, constant plasma concentrationand tra-cheal intubation with anesthetic agents were chosen to assess more clearly the effect on BIS values, hemody-namicandmovementresponse.GroupEs250weregivenan infusion dose known in the literature to suppress the BIS response;14,15GroupEs150weregivenadosethathasbeen
showntobe effectivein thetreatment of intra-operative HTandtachycardia18,19andGroupEs50weregiventhe
low-est infusion dose proposed to suppress the hemodynamic response.2,20
In induction, comparisons have been made on the suppressionofthehemodynamicresponsetotracheal intu-bationbetween different doses ofesmolol, as infusion or
Table2 AveragechangeinBIS.
Group GroupEs250(n=38) GroupEs150(n=39) GroupEs50(n=40)
BIS 2.86±2.64a 2.89±3.53a 9.25±4.84
BISmax 4.73±4.37a 6.17±6.85a 10.80±5.48
a p<0.05(comparedtoGroupEs50)
Table3 Motionresponseinthegroups.
Group GroupEs250(n=38) GroupEs150(n=39) GroupEs50(n=40)
Movement 19(50%)a 22(56.4%)a 35(87.5%)
Nomovement 19(50%)a 17(43.6%)a 5(12.5%)
bolus, placeboor withdifferent druggroups (nicardipine, lidocaine, alfentanil, fentanyl, etc.).18,21---27 Additionally,
no consensus has been reached on the optimum dose, administration method and timing.2,3 In a meta-analysis
studyevaluatingthe effectivenessof esmolol on hemody-namicchangesinducedbytrachealintubationbyFigueredo and Garcia-Fuentes,2 esmolol suppressed the adrenergic
response to tracheal intubation independent of dose and it was reported that after a loading dose of 500gkg−1,
within4min200---300gkg−1min−1continuousinfusiondose
wasthemostefficientprotocol.Johansenetal.12
adminis-teredpropofol/N2O/morphineanesthesiawithesmololand,
reportedadose-independentslightincreaseinHRandblood pressure after tracheal intubation. In this study, similar toprevious studies, after tracheal intubation in all three groupsanincreaseinHRandMAPindependentofdosewas found compared to values before intubation in all three groups.2,12,14
A short-termeffective 1 adrenergic receptor blocker,
ONO-1101 in increasing infusion doses, significantly sup-pressed the SAP increase linked to tracheal intubation, however it was reported that it increased the incidence ofhypotension.28 Similarly,FigueredoandGarcia-Fuentes2
inameta-analysisstudy,foundesmolol administeredwith induction agents and especially opioids, caused a dose-linked increase in hypotension and bradycardia incidence beforetrachealintubation.Togetherwiththisintheperiod beforeintubation in the placebo group therewas a 2.6% reduction in MAP while the esmolol group had a 10.1% decreaseinMAP.Similarlyinourstudy,inallthreegroups, thedeclineinMAPfromthebeginningofpropofolinfusion continuedafteradditionofesmololinfusionuntiltheperiod priortotracheal intubation.Although thereis no statisti-callysignificantdifferencebetweengroups;comparedwith baselineinall 3groups beforetrachealintubation (Group Es250:17%,GroupEs150:15%,andGroupEs50:11.2%)there was a significant decrease in MAP. However hypotension (MAP<60mmHg) or bradycardia (HR<50beatsmin−1) was
notobservedinanypatient.
Many studies on the effect of esmolol on the hemo-dynamic response to tracheal intubation have used succinylcholine as a muscle relaxant.21---27 Administration
of propofol with succinylcholine has caused significant bradycardia29andfasciculationsduetosuccinylcholinehave
been suggested to have an adverse affect on monitoring BIS.30 Forthesereasonswechoserocuroniuminourstudy.
Rocuronium’s vagolytic effect31 may have prevented the
expectedbradycardiaandhypotensionduetopropofoland esmololadministrationand contributedtoensuringstable hemodynamics. This situation we believe is additionally affectedbynotusingopioidsforinduction.
As described by Prys Roberts and Kissin, to determine the depth of anesthesia, voluntary movement response to a specific type of painful stimulus is the most appro-priate concept. Anesthesia depth is a pharmacodynamic measurementthatincludestheinteractionofthetwo med-ication groups (hypnotic and analgesic agents) that form thebasisofclinicalanesthesia.32Inhibitionofthecerebral
cortex by hypnotics results in clinical loss of conscious-ness and reduction in BIS values (or on EEG). The basic effectof analgesics is inhibition of the subcortical struc-tures and spinal cord weakening the communication of
painful stimuli to the cortex. As a result clinical con-sciousnesslevelsandmovement responsereduce. Inspite of the sedative effects of opioids suppressing thecortex, ‘‘unconsciousness’’isonlyformedbyhypnoticsatthe corti-callevel.‘‘Lackofresponse’’isformedbytheinteractions ofanalgesicsandhypnoticsatbothcorticalandsubcortical levels.32
Guignard et al.17 in patients under propofol
anesthe-sia in steady-state conditions found that in the absence ofpainfulstimuliremifentanylinfusiondidnotchangeBIS valuesbeforetrachealintubation;howeveritreducedthe increaseinBISvalues(BIS),hemodynamicandmovement
responses totracheal intubation in adose-linked manner. For this reason in evaluating the analgesic component of anesthesiaafterpainfulstimulitheyconcludedBISvalues
maybeassensitiveashemodynamicchanges.Berkenstadt et al.33 reported that bolus administrationof esmolol did
not change BIS values in the absence of painful stimuli. Menigaux et al.14 in patients anesthetized with propofol
andOdaetal.15inanesthesiawith1MACsevofluranewith
esmololinfusion,similartoopioids,foundtherewasno sig-nificanteffectontheBISvaluesbeforetrachealintubation, howeverincreaseinBISvalueslinkedtotracheal
intuba-tionandhemodynamicresponseandmovementdecreased. Kawaguchi et al.34 studied short-term effect landiolol, a 1 adrenoreceptor antagonist, during steady state
condi-tions of propofol anesthesia, and similartoremifentanyl, reported a suppressionin the increased entropyresponse (responseentropy=REandsituationentropy=SE,reflective of nociceptiveand hypnotic levels in general anesthesia) totrachealintubationintheformofnociceptiveresponse REand RE---SEresponsereductions.In ourstudysimilarto previousstudies,14,15intheabsenceofpainfulstimuliafter
esmololinfusionandbeforeintubationtherewasno reduc-tion in BIS values in all three groups. This result shows that in the absence of painful stimuli esmolol does not affect BIS during general anesthesia. Thus it can be said that esmolol alone has no anesthetic effect. In contrast, a steady-state conditions study by Johansen35 on
addi-tionof esmololinfusion topropofol/alfentanilanesthesia, showedBIS decreased whilecerebral cortical activitywas suppressedandburstsuppressionwascaused.Howeverthis studydidnotexaminesurgicalstimuliandalsoopioidswere used.
After esmolol infusion cortical EEG suppression and MACreductionshowsthatesmololinfusionshavedifferent pharmacologiceffects during anesthesia, becausecortical suppressionandMACareanatomicallyseparateinanimals.35
AftertrachealintubationinGroupEs250andGroupEs150,
BIS values and incidence of movement response were
significantly reduced compared to Group Es50. Johansen etal.inastudyonpropofol/N2Oanesthesiawithmorphine
premedication reported propofol’s Cp50 values (minimum
effectiveplasmaconcentrationtosuppressmovement due toskinincisionin 50%ofpatients) reducedlinkedtodose of esmololinfusion.12 In thesamegroup, esmololinfusion
affect movement responsewereused,and themovement response to the more submaximal painful stimuli of skin incision, comparedtotrachealintubation,wasevaluated. It is not possible to definitively comment on the effect of esmolol on the movement response to painful stimuli based on these two studies. The results of the present studyareinaccordancewiththoseofpreviousstudies,14,15
thoughtheeffectofesmololonBISandmovementresponse is shown to be dose linked. During propofol anesthesia in the absence of painful stimuli esmolol does not affect BISandinthepresenceof painfulstimulisuppressesBIS
values and movement response in a dose-linked manner, affecting BIS value increases and movement response to tracheal intubation in a similar manner to esmolol and opioids.14,15,17
The mechanism behind the effect of esmolol on BIS and movement response is not clear. The first mecha-nism proposed to explain this effect is that esmolol has acentralanti-nociceptiveeffect.Anothermechanismmay bepharmacokineticinteractionswithpropofoland/or opi-oids.
Painful stimuli travel through the spinal cord to the brain stem, reticular formation and thalamus and from therearetransmittedtothecerebralcortexwheretheEEG responseforms.8,14-Adrenergicreceptorsareknownin
var-ious regions of the reticular activating system and basal forebrain,especiallyinthemedialseptal.Inthisregion, -adrenoceptoragonistinfusionincreasesEEGactivityandthe behavioralsymptomsofwakefulnessinanimals;incontrast
-adrenoceptor antagonist infusion is shown to suppress the EEG response.14 Specific 
1-adrenoceptor antagonist,
ONO-1101,wasreportedtoreducethepainbehaviorafter intrathecal injections of formalin.14 Clinical studies show
esmololchangesEEGresponsetopainfulstimuliandreduces the increase in BIS.14,15 This brings to mind the
possibil-ity that esmolol’s effects on BIS may be similar to the reduction in -adrenoceptor block due to pain response increasingcentral catecholamine concentration.However, thefactthatshort-actingesmololishydrophilicandcannot passtheblood---brainbarrierdoesnotfullysupportthisidea. Therefore,furtherstudiesareneededontheroleofesmolol incentralmodulationofpain.
Theothermechanismtoexplaintheeffectofesmololon BISandmovementresponseispharmacokineticinteractions withpropofoland/oropioids.11,12Johansen,insteady-state
conditionspropofol/alfentanilanesthesia,foundthatwhile esmolol infusion didnotaffect the plasmaconcentrations of propofol and alfentanil or pharmacokinetics, BIS val-uesdecreasedandreversibleburstsuppressionsoccurred.35
Orme etal.36 found esmolol infusion did not significantly
reduce propofols Cp50-awake value or change the plasma
concentration of propofol. We did not use opioidsin our study.Howeveraspropofolconcentrationwasnotmeasured wecannoteliminatepotentialpharmacokineticinteractions with esmolol. In light of these data the mechanism for esmolol’seffectsonBISandthemovementresponseisnot fullyunderstood.
In conclusion, in patients anesthetized with propofol 250and 150gkg−1min−1esmolol infusion after1mgkg−1
loading dose reduce the increase in BIS values and the movementresponselinkedtotrachealintubationina dose-linked manner compared to 50gkg−1min−1 iv infusion.
Consideringtheresultsofthisstudy,itisconcludedthatin clinicalpractisetosuppresstheresponsestotracheal intu-bation1mgkg−1loadingdosefollowedby150gkg−1min−1
iv esmolol infusion may be used without increasing dose-linkedsideeffects.37
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.StanskiDR.Complicationsshorttermintubation.In:MillerRD, editor.Anesthesia.NewYork:ChurchillLivingstoneInc.;2005. p.1646---50.
2.FigueredoE,Garcia-FuentesEM.Assessmentoftheefficacyof esmololonthehaemodynamicchangesinducedbylaryngoscopy and tracheal intubation: a meta-analysis. Acta Anaesthesiol Scand.2001;45:1011---22.
3.Yu SK,TaitG, KarkoutiK, etal. Thesafetyofperioperative esmolol:asystematicreviewandmeta-analysisofrandomized controlledtrials.AnesthAnalg.2011;112:267---81.
4.StanskiDR.Drugsaffectingadrenergictransmission.In:Miller RD,editor. Anesthesia.New York:Churchill Livingstone Inc.; 2005.
5.London JM, Zaugg M, Schaub MC, et al. Perioperative  -adrenergicreceptorblockade.Anesthesiology.2004;100:170---5.
6.ZauggM,ThomasT,ElianaL,etal.Beneficialeffectsfrom -adrenergicblockadeinelderlypatientsundergoingnoncardiac surgery.Anesthesiology.1999;91:1674---86.
7.Coloma M,ChiuJW, White PF, et al. The use ofesmolol as analternativetoremifentanilduringdesfluraneanesthesiafor fast-trackoutpatientgynecologiclaparoscopicsurgery.Anesth Analg.2001;92:352---7.
8.DavidsonEM,DoursoutMF,SzmukP,etal.Antinociceptiveand cardiovascularpropertiesofesmololfollowingformalin injec-tioninrats.CanJAnaesth.2001;48:59---64.
9.ChiaYY,ChanMH,KoNH,etal.Roleof-blockadein anaesthe-siaandpostoperativepainmanagementafterhysterectomy.Br JAnaesth.2004;17:1---7.
10.WhiteFP,WangB,TangJ,etal.Theeffectofintraoperative useofesmololand nicardipineonrecovery afterambulatory surgery.AnesthAnalg.2003;97:1633---8.
11.JohansenJW,SchneiderG,WindsorAM,etal.Esmolol poten-tiatesreductionofminimumalveolarisofluraneconcentration byalfentanil.AnesthAnalg.1998;87:671---6.
12.Johansen JW, Flaishon R, Sebel PS. Esmolol reduces anes-thetic requirement for skin incision during propofol/nitrous oxide/morphine anesthesia. Anesthesiology. 1997;86: 364---71.
13.WilsonES, McKinlayS,Crawford JM,et al. The influenceof esmololonthedoseofpropofolrequiredforinductionof anaes-thesia.Anaesthesia.2004;59:122---6.
14.MenigauxC,GuignardB,AdamF,etal.Esmololprevents move-mentandattenuatestheBISresponsetoorotrachealintubation. BrJAnaesth.2002;89:857---62.
15.Oda Y, Nishikawa K, Hase I, et al. The short-acting 1 -adrenoceptor antagonistsesmolol and landiolol suppressthe bispectralindexresponsetotrachealintubationduring sevoflu-rane.AnesthAnalg.2005;100:733---7.
16.SlavovV,MotamedC,MassouN,etal.Systolicbloodpressure, notBIS,isassociatedwithmovementduringlaryngoscopyand intubation.CanJAnesth.2002;49:918---21.
responses after orotracheal intubation. Anesth Analg. 2000;90:161---7.
18.GoldIM,Sacks JD,GrosnoffBD. Useofesmolol during anes-thesia to treat tachycardia and hypertension.Anesth Analg. 1989;68:101---4.
19.Reves JG, Groughwell ND, Hawkins E, et al. Esmolol for treatmentintraoperativetachycardiaand/or hypertensionin patientshavingcardiacoperation.JThoracCardiovasc Surg. 1990;100:221---7.
20.Mooss NA, Hilleman ED, Mohiuddin MS. Safety of esmolol in patients with acute myocardial infarction treated with thrombolytic therapy who had relative contraindications to beta-blockertherapy.AnnPharmacother.1994;28:701---70.
21.Helfman MS, Gold IM, DeLisser AE. Which drug prevents tachycardia and hypertension associated withtracheal intu-bation:lidocaine,fentanyloresmolol.AnesthAnalg.1991;72: 482---6.
22.EbertJP,PearsonDJ,GelmanS.Circulatoryresponsesto laryn-goscopy: the comparative effects of placebo, fentanyl and esmolol.CanJAnaesth.1989;36:301---6.
23.ChungSK,SinatraSR.comparisonoffentanyl,esmolol,andtheir combinationforbluntingthehaemodynamicresponsesduring rapid-sequenceinduction.CanJAnaesth.1992;39:774---9.
24.TanPH,YangLC,ShihHC.Combineduseofesmololand nicardi-pinetobluntthehaemodynamicchangesfollowinglaryngoscopy andtrachealintubation.Anaesthesia.2002;57:1195---212.
25.OxornD,KnoxJWD.Bolusdosesofesmololfortheprevention ofperioperativehypertensionandtachycardia.CanJAnaesth. 1990;37:206---9.
26.Kanitz DD, Ebert JT, Kampine PJ. Intraoperative use of bolus dosesof esmololto treat tachycardia.JClinAnaesth. 1990;2:238---42.
27.Atlee JL, Dhamee MS,Olund TL, et al. The useof esmolol, nicardipineortheircombinationtoblunthemodynamicchanges
after laryngoscopy and tracheal intubation. Anesth Analg. 2000;90:280---5.
28.KitamuraA,SakamotoA, OgawaR.Efficacyofan ultrashort-acting beta-adrenoceptorblocker (ONO-1101) in attenuating cardiovascularresponsestoendotrachealintubation.EurJClin Pharmacol.1997;51:467---71.
29.ReisnerLS,LinD.Anesthesiaforcesareansection.In: Chest-nutDH,editor.Obstetricanesthesia.Philadelphia,PA:Mosby Elsevier;1999.p.465---92.
30.SieMY,GohPK,Chan L, et al.Bispectral indexduring mod-ifiedrapidsequenceinductionusing thiopentoneor propofol androcuronium.AnaesthIntensiveCare.2004;32:28---30.
31.SavareseJJ.Neuromuscular blocking agents. In: Morgan GE, MikhailMS,editors.Clinicalanesthesiology.USA:McGraw-Hill Medical;2002.p.178---99.
32.StanskiDR.Monitoringdepthofanesthesia.In:MorganGE, edi-tor.Anesthesia.NewYork:ChurchillLivingstoneInc.;2005.p. 1087---116.
33.BerkenstadtH,LoebsteinR,FaibishenkoI,etal.Effectsofa singledoseofesmololonthebispectralindexscale(BIS)during propofol/fentanylanaethesia.BrJAnaesth.2002;89:509---11.
34.KawaguchiM,TakamatsuI,MasuiK,etal.Effectoflandiolol on bispectral index and spectral entropy responses to tra-cheal intubation during propofol anaesthesia. Br J Anaesth. 2008;101:273---8.
35.JohansenJW.Esmololpromoteselectroencephalographicburst suppression during propofol/alfentanil anesthesia. Anesth Analg.2001;93:1526---31.
36.OrmeR,LeslieK,UmranikarA,etal.Esmololandanesthetic requirementforlossofresponsivenessduringpropofol anesthe-sia.AnesthAnalg.2002;93:112---6.