208 PAHO BULLETIN l vol. 19, no. 2, 1985
In 1975 a national average of 47 bacilloscopies were performed per 1,000 consultations, the cor- responding figures for 1978 and 1983 being 48.7 and 47.2 per 1,000, respectively. Susceptibility studies carried out in Chile, mainly for epide- miologic purposes, have shown that primary re- sistance dropped from 12.8% in 1970 to 10.1% in 1975 and 7.9% in 1981. Similarly, secondary resistance has greatly decreased, from 48.5% in
1971 to 32.2% in 1975 and 28.2% in 1979. Radiology as a case-finding method was not included in the guidelines of the tuberculosis control program initially, but was officially in- corporated in 1983 for persons over 40 years of age with respiratory symptoms, since they run a greater risk of dying from tuberculosis than do the lower age groups. The results obtained with this method will be evahlated in coming years.
Treatment
Since 1975, treatment has been evaluated on the basis of cohorts of patients diagnosed and followed up until final discharge. Abandonment of treatment has dropped from 25% to 12%, and the number of patients discharged as inactive cases has risen from 55% to 70%. Introduction of the shortened rifampicin treatment has led to a drop in the case-fatality rate from 6% to 3%.
More than 80% of the cases currently receive full follow-up outpatient treatment; less than 20% of the patients commence their treatment with a short period of hospitalization.
Source: Chile, Ministerio de Salud, Bolerin de vigilancia epidemiol&ica 1 l(S), 1984; and World Health Organiza- tion, Weekly Epidemiological Record 60(9):66-67, 1985.
MEASLES SURVEILLANCE IN PANAMA Measles in the Republic of Panama occurs in
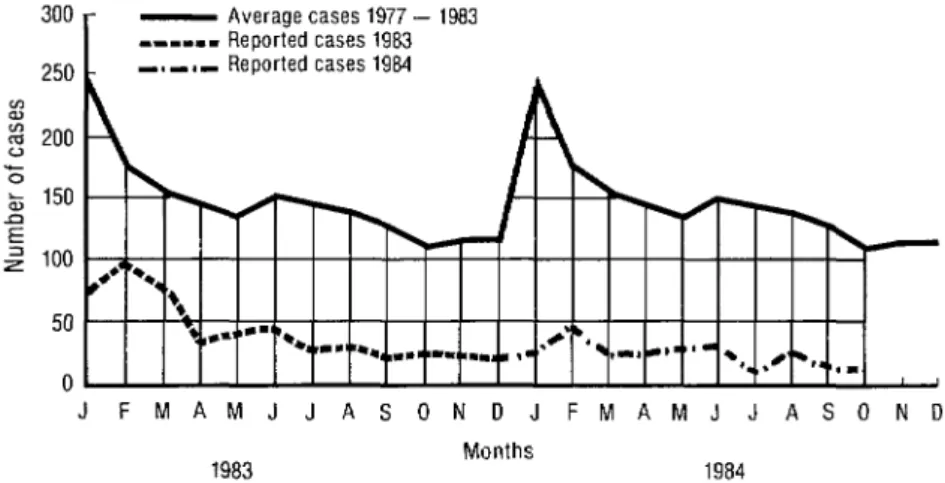
a pattern that makes it possible to predict epi- demics every two or three years, especially be- tween November and March. Specifically, on the basis of data obtained from monitoring the De- cember 1981-March 1982 epidemic in Panama, it was predicted that the last trimester of 1984 would be a high-risk period for measles.
Because of this finding, vaccination and sur- veillance activities were intensified at the local and regional levels, and individual case investi- gations were conducted to determine people’s previous vaccination status and to help ensure the vaccination of all susceptible children.
During the course of these case investigations, cases of measles were defined using the clinical criteria proposed by the United States Centers for Disease Control in Atlanta, these being (a) a fever of 38.3’C or more, (b) a generalized rash lasting three days or more, and (c) at least one of the following: coryza, conjunctivitis, or coughing.
Many suspected cases were found not to be measles cases on the basis of these criteria- especially suspected cases in infants under six months of age and in persons over six years of age.
As of October 1984, a total of 338 measles cases had been reported in the Republic of Panama. This represents a reduction of 36% compared with the same period in 1983.
0 ABSTRACTS AND REPORTS 209
250
Figure 1. Measles cases by year and month, 1983-1984, Panama.
- Average cases 1977 - 1983 --111 Reported cases 1983 -,-,- Reported cases 1984
JFMAMJJASONOJFMAMJJASOND
Months
1982 and Bocas de1 Toro in 1983 managed to -
avoid epidemics by means of exhaustive vacci- Source: Panama, Caja de Seguro Social, Boletin epide- nation efforts by regional and local teams. Their mioldgico 8( 1O):l , 1984; and Pan American Health Organi- zation, EPI Newsletter 7(1):6-X, 1985.
experience shows that measles can be controlled in Panama.)
YELLOW FEVER IN THE AMERICAS
The total number of jungle yellow fever cases resented the end of an epidemic that had taken in the Americas in 1983 was one of the lowest in place in the Santa Cruz region of Bolivia in 198 1 recent years. Only the usual endemo-sporadic and 1982, and the end of an epidemic outbreak cases were reported in Bolivia, Brazil, Colom- in Brazil that had advanced from the State of bia, Ecuador, and Peru (Table 1, Figure 1). The Goias in 1980 (21 cases) southwards to the State two outstanding occurrences during the year rep- of Mato Gross0 in 1981 (10 cases) and the State of Mato Gross0 do Sul in 1982 (12 cases). This
Table 1. Reported numbers of jungle yellow fever cases and deaths in South America, 1982-1983.
1982 1983
COUIltry Reported Reported Reported Reported cases deaths cases deaths
Bolivia 95 35 11 9
Brazil 24 24 6 6
Colombia 2 2 1 1
Ecuador - - 5 1
Peru 19 19 27 26
Total 140 80 50 43
latter was the most recent of the periodic spreads of yellow fever that occur about every 10 years in Brazil. The small number of cases, compared with previous epidemics, was the result of an increasing number of vaccinations in the affected regions. Previous outbreaks in Brazil took place in 1934, 1944, 1957, 1964, and 1973.