Available
online
at
www.sciencedirect.com
j ourna l h o me p a g e :h t t p : / / w w w . e l s e v i e r . c o m / l o c a t e / r p o r
Case
report
Entire
hemithorax
irradiation
for
Masaoka
stage
IVa
thymomas
André
Soares
a,∗,
Luís
Vasco
Louro
a,
Marta
Almeida
b,
Olga
Sousa
aaRadiotherapyDepartment,InstitutoPortuguêsdeOncologiadoPortoFranciscoGentil,E.P.E,Portugal
bOncologyDepartment,HospitalEscala,Braga,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received9January2012 Receivedinrevisedform 19April2012
Accepted27May2012
Keywords: Thymoma StageIVa Hemithoracic Radiotherapy
a
b
s
t
r
a
c
t
Thymomasarerareneoplasmsthathaveanindolentgrowthwithapreferentially intra-thoracicdisseminationpattern.Surgeryiscurrentlythestandardtreatmentofthymomas; howeverradiotherapyisoftenusedinanadjuvantsettingduetoahighsensitivityofthese tumorstosuchtreatment.Postoperativeentirehemithoracicirradiationhasbeenusedin selectedMasaokastageIVacasesaftercompletesurgicalexcisionofmetastaticlesions.
Inthepresentarticle,theauthorsreportthreecasesofMasaokastageIVathymomathat underwententirehemithoraxirradiationaftersurgicalexcisionofmetastaticlesions.The firsttwopatientspresentedasstageIVathymomas.Thethirdcaseconsistedofapleural recurrenceofathymoma.
Hemithoracicirradiationwithlowdoseshasbeenusedbydifferentauthors;theavailable datashowsthatitisawell-toleratedtreatmentthatcouldpotentiallyleadtobetter loco-regionalcontrolandincreasedoverallsurvival.
©2012GreaterPolandCancerCentre.PublishedbyElsevierUrban&PartnerSp.zo.o.All rightsreserved.
1.
Background
Thymomasarearareentitywithanincidenceof1.5newcases permillionperyear,representing20–50%ofallanterior medi-astinaltumorsinadultsand15%inchildren.1–4 Theyoccur
withequalfrequencyinmenandwomenandthereisno pref-erenceforaparticularraceorgeographicdistribution.1–4Ithas
abimodaldistributionregardingageatpresentation;thefirst peakoccursinthe4thdecadeandisassociatedwith myas-theniagravis,andthesecondoneoccursinthe7thdecade.5–8
These are malignant tumors that originate from the thymic epithelium and usually have an exuberant lym-phoidcomponent.8–11TheWorldHealthOrganization’s(WHO)
∗ Correspondingauthor.Tel.:+351919806156.
E-mailaddress:andrecoki@hotmail.com(A.Soares).
histological classification is the most widely used one in current clinical practice. It is based on cell morphology and the ratiobetweenlymphocytes and epithelialcells.9–12
Thymomasareclassifiedaccordingtotheshapeofthe neo-plastic cells as: type A (spindle or oval), type B (dendritic or epithelioid) and typeC (thymiccarcinoma). Type B thy-momas are furtherdividedaccording tothe atypiaofcells and proportion of thymocytes relative to lymphocytes: B1 thymomas are the richest in lymphocytes and B3 have a marked cellular atypia and rare lymphocytes.9–12 Thymic
carcinomas(typeC)aredesignatedaccordingtotheir differen-tiationas:squamouscell,neuroendocrine,mucoepidermoid, basaloid, lymphoepithelioma, sarcomatoid, clear cell and papillary.9,10
1507-1367/$–seefrontmatter©2012GreaterPolandCancerCentre.PublishedbyElsevierUrban&PartnerSp.zo.o.Allrightsreserved.
Thymomas have an indolent growth, 33% of patients areasymptomaticatpresentation.Oftheremaining (symp-tomatic) cases, 30–65% are associated with myasthenia gravis.1,8,10
Themostwidelyadoptedstagingsystemistheone pro-posedbyMasaoka.Lesionsarestagedaccordingtothedegree ofspreadasfollows:stageI,completelyencapsulatedlesions; stageII,lesionswithmicroormacroscopiccapsularinvasion; stageIII, lesionsthatinvadeadjacentorgans (greatvessels, lung,pericardium)andstageIV,disseminateddisease,which issubdividedintoIVa(pleuralorpericardialimplants)andIVb (embolicmetastases).1,8,10–12
Surgeryiscurrentlythetreatmentofchoiceforthymomas. Thecriteriathatneedtobetakenintoaccountwhen decid-ing ifand which adjuvanttherapies are neededare:stage, histologicalgradeandsurgicalmargins.Adjuvantirradiation oftumorbedseemstobebeneficialinstageIpatientswith incompleteresections,andallstagesIIandIIIpatients,due tohighrecurrencerates evenaftercomplete resection.13–20
Themethodbywhichradiationisdeliveredisalsoimportant (favoringhighenergyphotons),asithasbeendemonstrated thatitisanindependentprognosticfactorforoverallsurvival (OS).21
Inthemeta-analysisbyKorstandcolleagues14theaddition
ofadjuvant radiotherapytosurgicaltreatment reducedthe percentageofrecurrenceinstageII,from0–62%to0–25%and instageIII,from13–80%to0–64%.
Asdocumentedintheliterature,themostcommonsitesof diseaserecurrenceare:thepleuralmembranes,thelung,the pericardiumandthediaphragm.19,20,22–25
StageIVa thymomas and regional (intra-thoracic) recur-rence are challenging in terms of treatment approach. Althoughconsideredadisseminateddisease,pleuraland peri-cardiallesionsareoftenresectableandhighsurvivalratesare achievable.20,22–24 Severalauthorshavemanagedcaseswith
extensivepleuraldiseasetreatedwithpleurectomyfollowed bytotalhemithoraciclowdoseirradiation,withgoodresults andlowmorbidity.20,22–26
Threeclinicalcasesarepresentedinthefollowingsection: twopatientswithstageIVathymomaatdiagnosisand one withpleuralrecurrence.Allpatientsunderwentsurgical exci-sionofpleuralimplantsandtotalhemithoracicirradiation.
2.
Case
1
Forty-one-year-oldfemale,diagnosedwithmyastheniagravis afterthestudyofapersistentfatigueandasthenia.The com-puterizedtomography(CT)acquiredinApril2009revealeda 4cm×3.5cm anterior mediastinallesion suggestiveof thy-momaaswellasareasofthickeningoftheleftpleura.
In June 2009, the patient underwent thoracoscopical resectionofthethymoma.Thehistologicalresultsrevealeda predominantlylymphocyticthymomawithanepithelial com-ponent,typeB1.Biopsieswerealsotakenofthe suspicious pleurallesionsthatwerediagnosedasmetastasisofthymoma typeB1.ThisyieldedaMasaokastageIVa.
An octreotide scan and a 18FDG-PET/CT were also per-formed; the first did not show any anomalous uptake of the radionuclide, whilethe other revealed multiplefoci of
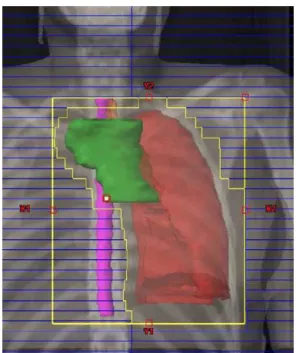
Fig.1–Entirelefthemithoraxandmediastinumvolume.
increased metabolism along the left posterior pleura and twofoci inthe baseofthe ipsilateral lung.The multidisci-plinarytumorboardproposed5cyclesofchemotherapywith cyclophosphamide, adriamycin and cisplatin (CAP) which endedinOctober2009.Afterchemotherapyasecond evalu-ationwith18FDG-PET/CTrevealedapersistentdisease.
Itwasdecidedtosubmitthepatienttoparietaland vis-ceralpleurectomyandexcisionoftheperipheralpulmonary lesions.Thepathologicalfindingswereconsistentwith pul-monary and pleural metastasis of type B1 thymoma, R0 resection.
Subsequently, the patient underwent entire hemithorax andanteriormediastinumradiotherapy.
Theentirelefthemithoraxreceived12Gyin12fractions of1Gy,5timesaweekwithathreefieldtechnique (antero-posterior,postero-anteriorandcranial–caudalrightposterior oblique)with6MVphotonsplus45Gyin25fractionsof1.8Gy, 5daysaweektotheanteriormediastinumthrough2fields (anterior oblique andposterior oblique) with6MV photons
(Figs.1and2).
Therewerenocomplicationsduringtreatment.Attheend ofthetreatment,thepatientpresentedastheniaanddyspnea withordinaryeffort.Respiratorysoundswereequalbilaterally. Thispatientchangedresidencyandwaslosttofollow-up.
3.
Case
2
Thirty-four-year-oldfemale,presentedwithahistoryof non-productivecough,moderatedyspneaandweightloss.
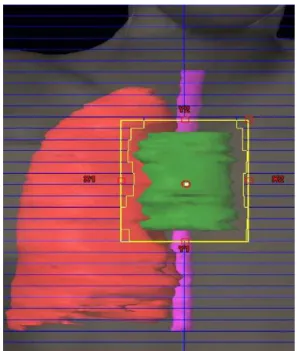
Fig.2–Anteriormediastinumvolume.
Assessmentwithanoctreotidescanrevealedanincreased uptakeoftheradionuclideintherighthemithoraxwith exten-siveinvolvementoftheanteriorandposteriormediastinum. 18FDG-PET/CTshowed increased metabolism involving the
entirerightpleura.
Thetumorboarddecidedtotreatthepatientwith6cycles of chemotherapy: cyclophosphamide, adriamycin, cisplatin (CAP)plusprednisolone.
The post chemotherapy 18FDG-PET/CT showed partial responsewithpersistentuptakefociinthethymusandpleura. InFebruary 2010,the patientwassubmitted to thymec-tomyandtotalparietalpleurectomyincludingresectionofthe pericardialanddiaphragmaticpleura.Histologicexamination revealedatypeB2/B3corticalthymomawithpleuralinvasion, R0ressection.
Then,sheunderwentadjuvantradiotherapytotheentire hemithoraxandanteriormediastinum.
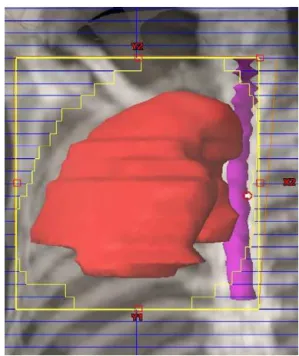
Theentirerighthemithorax(Fig.3)received12Gy in12 fractionsof1Gy,5timesaweekwithatwofield technique (antero-posterior and postero-anterior) with6MV photons, plus45Gyin25fractionsof1.8Gy,5daysaweektothe ante-riormediastinum(Fig.4)through4fields (antero-posterior, postero-anterior,rightobliqueandleftanterioroblique)with 6MVphotons(Figs.3and4).
Therewerenocomplicationsduringtreatment.Attheend ofthetreatment,thepatientpresentedarightchestpain,but norespiratory symptoms. Pulmonaryauscultation revealed diminishedrespiratorysoundsonthebaseoftherightlung.
ThreemonthsafterRT,thepatientreportedasthenia, dys-pneaondoingmorethanordinaryeffort,andrightthoracic pain.Pulmonarysoundsonthebaseoftherightlungwere diminished.
OnDecember2011,thepatienthadnosymptomsorany evidenceofrecurrentdisease.
Fig.3– Righthemithoraxandmediastinumvolume.
4.
Case
3
Fifty-two-year-oldmale,diagnosedwithMasaokastageIII thy-momaB3in2000aftertotalthymectomy.BetweenJulyand August 2000,hewassubmittedtoadjuvantradiotherapyto theanteriormediastinum(totaldoseof45Gyin25fractions with6MVphotons).
In2005,thepatientunderwentsurgicalexcisionofright pleuralsuspiciouslesionsthatwerepathologicallydiagnosed asthymomametastases,R1resection.
Fig.5–Entirerighthemithoraxvolume.
Thepatientcompletedsixcyclesofchemotherapywith cis-platin,vincristine,doxorubicinandcyclophosphamide(ADOC regimen)byDecember2005.
In2007,apleuralrecurrencewas diagnosedand hewas submittedto11cyclesofchemotherapy–FOLFOX–achieving acompleteremission(assessedby18FDG-PET/CT).
Duetoanewpleuralrelapsein2008,thepatientwasonce again subjected to chemotherapy – Carboplatin and Pacli-taxel– achievingstabilizationofthediseaseuntilMarch2010. Because ofdisease progression, the patient underwent an incompletesurgicalexcisionofpleurallesionsthatwerealso compatiblewithpleuralmetastasesofthymoma.
Thetumorboardthenproposedentirehemithorax irradi-ation,whichthepatientaccepted.
Thepatientperformed3Dconformalradiotherapywiththe followingplan:12Gy tothe entireright hemithorax(Fig.5) in12fractionsof1Gyeach,5daysaweek,using6MV pho-tonsthrough4fields(antero-posterior,postero-anterior,right lateralandleftlateral).
Therewerenocomplicationsduringtreatment.Attheend ofthetreatmentthe patientreportednorespiratoryorany othersignificantsymptoms.Pulmonarysoundswere dimin-ishedontheinferiorhalfoftherightlung.
OnDecember2011,thepatienthadnosymptomsorany evidenceofrecurrentdisease.
5.
Discussion
Giventherarityofthymomas,its therapeuticapproachhas beenevaluatedsolelyinretrospectiveseries.Furthermore,the therapeuticmanagement ofstageIVa isonlymentioned in smallseriesandcase-reports.
Inthe initialMasaokapublications,patients withinitial stageIV(includingIVaandIVb)hadsurvivalratesof approxi-mately50%at5yearsand0%at10years.24Sincethen,several
authorshavearguedthatamultimodaltreatmentapproach
mayincreasetheresectabilityofthediseaseandreduce recur-rencerates.20
Thismultimodalapproachshouldincludepreoperativeor postoperativechemotherapy,1,2,4,20,25 extensivesurgerywith
maximumpossibleresectionofthepleuraldiseaseand post-operative radiotherapy to the thymic bed with low dose irradiationtotheentireinvolvedhemithorax.24–26
In these stages, the most widely used chemotherapy schemes in the literature are based on cisplatin or doxo-rubicin, including ADOC (cisplatin, doxorubicin,vincristine and cyclophosphamide) and PAC (cisplatin, cyclophos-phamide, anddoxorubicin) withorwithout theadditionof corticosteroids.1,2,20,25ThereviewperformedbyKondo20that
includedthymomasinadvancedstages(IIIandIV)confirmed thebenefitofaddingchemotherapy,sinceitallowedtoachieve anobjective responsein67–100%ofpatientsandcomplete responsesinabout33%.
ThesurgicaltreatmentofstageIVa(orpleuralrecurrence) casesconsistsinthemaximumpossibleresectionofall pleu-raland/orpericardialimplantsusing,ifnecessary,extensive pleurectomy or resection of the pericardium. Despite the aggressivenessofthisapproach,Huangetal.25 presenteda
seriesof18patientswhounderwentpleurectomyandwedge resectionsofinvolvedlungwithlowmorbidity,nooperative mortalityandhighOS.
Therationaleofusingpost-operativehemithoracic irradi-ation isbasedon threemainpoints:the knownsensitivity ofsuchtumorsto radiation;theknown application ofthis radiotherapytechniqueinmesotheliomasafterextra-pleural pneumonectomyandthefactthattheriskofrecurrenceof thediseaseismuchhigherloco-regionallythandistantly.8,10,14
Inthiscontext,radiotherapydosesmoreoftenreportedhave beenbetween11.2Gyand16Gyin7–10fractions.
Uematsuetal.27usedtotalhemithoracicirradiation
pro-phylacticallyinstagesIIandIII,usingdosesbetween10–16Gy in 10–16 fractions. Recurrence-free survival of 100% at 5 yearswasachievedintheentirehemithoraxirradiationgroup (withgood clinical tolerance)versus 66% inthegroup that onlyreceivedradiotherapytothethymicbed.Thisreinforces the ideathatthe additionofradiotherapyisbeneficial and produceslowsideeffects.
According to Huang et al.,25 this multimodal approach
achieves OS rates of 91%, 78% and 65% at 3, 5 and 10 years, respectively, which is much higher than initially reported.24
6.
Conclusion
Therearefewstudiesabouttheoptimaltherapeuticapproach for stageIVa thymomas. Somepublications report thatfor selected patients in stage IVa, postoperative (excision of metastaticlesions)radiotherapytotheentirehemithoraxwith doses ranging from 11 to 16Gy with fractions of 1–1.6Gy shouldbeconsidered.
Prospectivemulticenterstudiesareneededtoassessand validatetheeffectivenessofthismodalityapproachtotreat MasaokastageIVathymoma.
Conflict
of
interest
Nonedeclared.
Financial
disclosure
Nonedeclared.
r
e
f
e
r
e
n
c
e
s
1. LuJJ,ThamIWK,KongF-M.Thymictumors.In:LuJJ,Brady LW,editors.Decisionmakinginradiationoncology,vol.2. Heidelberg:Springer;2011.p.309–28.
2. WrightCD.Managementofthymomas.CritRevOncolHematol 2008;65(2):109–20.
3. EngelsEA.Epidemiologyofthymomaandassociated malignancies.JThoracOncol2010;5(October(10Suppl. 4)):S260–5.
4. VenutaF,AnileM,DisoD,etal.Thymomaandthymic carcinoma.EurJCardiothoracSurg2010;37(January(1)): 13–25.
5. LucchiM,RicciardiR,MelfiF,etal.Associationofthymoma andmyastheniagravis:oncologicalandneurologicalresults ofthesurgicaltreatment.EurJCardiothoracSurg2009;35(May
(5)):812–6,discussion816.
6. MarcinZ.Managementofmyasthenicpatientswith thymoma.ThoracSurgClin2011;21(1):47–57.
7. LeeBW,IhmSH,ShinHS,YooHJ.Malignantthymoma associatedwithmyastheniagravis,Graves’disease,and SIADH.InternMed2008;47(11):1009–12.
8. HungAY,EngTY,ScarbroughTJ,FullerJrCD.CRT. Mediastinumandtrachea.In:HalperinEC,PerezCA,Brady LW,editors.PerezandBrady’sprinciplesandpracticeofradiation oncology.5thed.Philadelphia:WoltersKluwer
Health/LippincottWilliams&Wilkins;2008.p. 1109–17.
9. MarchevskyAM,GuptaR,McKennaRJ,etal.Evidence-based pathologyandthepathologicevaluationofthymomas. Cancer2008;112(12):2780–8.
10. SovakMA,AisnerSC,AisnerJ.Tumorsofthepleuraand mediastinum.In:AbeloffMD,ArmitageJ,NiederhuberJ, KastanM,McKennaW,editors.Abeloff’sclinicaloncology.4th ed.Philadelphia:ChurchillLivingstone/Elsevier;2008.p. 1367–98.
11. SusterS.Diagnosisofthymoma.JClinPathol 2006;59(December(12)):1238–44.
12. HosakaY,TsuchidaM,ToyabeS.-i.,UmezuH,EimotoT, HayashiJ-i.Masaokastageandhistologicgradepredict
prognosisinpatientswiththymiccarcinoma.AnnThoracSurg 2010;89(March(3)):912–7.
13. FullerCD,HousmanDM,ThomasCR.Radiotherapyfor thymomaandthymiccarcinoma.HematolOncolClinNorthAm 2008;22(June(3)):489–507.
14. KorstRJ,KanslerAL,ChristosPJ,MandalS.Adjuvant radiotherapyforthymicepithelialtumors:asystematic reviewandmeta-analysis.AnnThoracSurg2009;87(May (5)):1641–7.
15. EngTY,ThomasJrCR.Radiationtherapyinthemanagement ofthymictumors.SeminThoracCardiovascSurg2005;17(Spring (1)):32–40.
16. ForquerJA,RongN,FakirisAJ,LoehrerPJ,JohnstonePAS. Postoperativeradiotherapyaftersurgicalresectionof thymoma:differingrolesinlocalizedandregionaldisease.Int JRadiatOncolBiolPhys2010;76(2):440–5.
17. OgawaK,UnoT,ToitaT,etal.Postoperativeradiotherapyfor patientswithcompletelyresectedthymoma:a
multi-institutional,retrospectivereviewof103patients. Cancer2002;94(March(5)):1405–13.
18. UtsumiT,ShionoH,KadotaY,etal.Postoperativeradiation therapyaftercompleteresectionofthymomahaslittle impactonsurvival.Cancer2009;115(December(23)):5413–20. 19. PatelS,MacdonaldOK,NagdaS,BittnerN,Suntharalingam
M.Evaluationoftheroleofradiationtherapyinthe managementofmalignantthymoma.IntJRadiatOncolBiol Phys2011[Epub2011May17].
20. KondoK.Optimaltherapyforthymoma.JMedInvest 2008;55(February(1–2)):17–28.
21. HetnałM,MałeckiK,WolaninM,KorzeniowskiS,WalasekT. Thymoma:resultsoftreatmentandroleofradiotherapy.Rep PractOncolRadiother2010;15(1):15–20.
22. TagawaT,KometaniT,YamazakiK,etal.Prognosisand therapeuticresponseaccordingtotheWorldHealth Organizationhistologicalclassificationinadvanced thymoma.SurgToday2011;41(December(12)):1599–604.
23. HuangJ,RielyGJ,RosenzweigKE,RuschVW.Multimodality therapyforlocallyadvancedthymomas:stateoftheartor investigationaltherapy?AnnThoracSurg2008;85(February
(2)):365–7.
24. SugieC,ShibamotoY,Ikeya-HashizumeC,etal.Invasive thymoma:postoperativemediastinalirradiation,low-dose entirehemithoraxirradiationinpatientswithpleural dissemination.JThoracOncol2008;3(1):75–81, 10.1097/JTO.1090b1013e31815e3181831873.
25. HuangJ,RizkNP,TravisWD,etal.Feasibilityofmultimodality therapyincludingextendedresectionsinstageIVAthymoma. JThoracCardiovascSurg2007;134(December(6)):1477–84.
26. YanoM,SasakiH,YukiueH,etal.Thymomawith dissemination:efficacyofmacroscopictotalresectionof disseminatednodules.WorldJSurg2009;33(July(7)):
1425–31.