ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Brief
communication
Is
there
an
association
between
systemic
lupus
erythematosus
and
periodontal
disease?
夽
Débora
Cerqueira
Calderaro
a,∗,
Gilda
Aparecida
Ferreira
b,
Santuza
Maria
Souza
de
Mendonc¸a
c,
Jôice
Dias
Corrêa
d,
Fabrícia
Xavier
Santos
e,
João
Guilherme
Capinam
Sanc¸ão
e,
Tarcília
Aparecida
da
Silva
f,
Antônio
Lúcio
Teixeira
gaPost-GraduatePrograminInfectiousandParasiticDiseases,MedicineSchool,UniversidadeFederaldeMinasGerais(UFMG),Belo
Horizonte,MG,Brazil
bDepartmentofLocomotorSystem,SchoolofMedicine,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil cDentalSchool,CentroUniversitárioNewtondePaiva,BeloHorizonte,MG,Brazil
dPost-GraduatePrograminCellBiology,BiologicalSciencesInstitute,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,
Brazil
eUniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil
fDepartmentofClinics,PathologyandSurgery,DentalSchool,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil gMedicineSchool,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received31July2014
Accepted1March2015
Availableonline8September2015
Keywords:
Systemiclupuserythematosus
Periodontitis
Chronicperiodontitis
a
b
s
t
r
a
c
t
Periodontaldiseaseresultsfromtheinteractionbetweenpathogenicbacteriathatcolonize
supragingivalandsubgingivalbiofilmsandthehost,triggeringaninflammatoryresponse,
withsystemiceffectsleadingtoimmune-mediateddestructionoftheattachment
appara-tusandlossofsupportingalveolarbone.Immunologicalpathwaysandpredisposinggenetic
factorscommontoperiodontaldiseaseandrheumaticdiseases,includingsystemiclupus
erythematosus,havebeendescribed.Casereportshavesuggestedgreaterseverityof
peri-odontaldiseaseinpatientswithsystemiclupuserythematosus.However,studiesevaluating
theinfluenceofthetreatmentofonediseaseontheclinicalandlaboratorymanifestations
oftheotherhaveyieldedconflictingresults.
©2015ElsevierEditoraLtda.Allrightsreserved.
Há
associac¸ão
entre
o
lúpus
eritematoso
sistêmico
e
a
doenc¸a
periodontal?
Palavras-chave:
Lúpuseritematososistêmico
Periodontite
Periodontitecrônica
r
e
s
u
m
o
Adoenc¸aperiodontalresultadainterac¸ãoentrebactériaspatogênicasquecolonizamos
filmessupraesubgengivaleohospedeiroedeflagramumarespostainflamatórialocal,com
efeitossistêmicos,quelevaàdestruic¸ãoimunomediadadostecidosdesustentac¸ãodos
dentesedoossoalveolar.Viasimunológicasefatoresgenéticospredisponentescomuns
夽StudylinkedtotheMedicineSchoolandDentalSchool,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](D.C.Calderaro).
http://dx.doi.org/10.1016/j.rbre.2015.08.003
àdoenc¸aperiodontaleàsdoenc¸asreumáticas,entreelasolúpuseritematososistêmico,
vêmsendodescritos.Relatosdecasosugerirammaiorgravidadedadoenc¸aperiodontal
em pacientescomlúpuseritematoso sistêmico. Noentanto,estudosqueavaliaramas
influênciasdotratamentodeumasobreasmanifestac¸õesdaoutraapresentaramresultados
conflitantes.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Currently,therelationshipbetweenconnectivetissuediseases
andperiodontaldisease (PD)hasbeen thesubjectofmuch
discussion.1
PDisagroupofinfectiousandinflammatorydiseasesthat
resultfrom the interaction betweenperiodontal pathogens
present in supragingival and subgingival biofilms and the
host,generatinganinflammatoryresponseofvariable
inten-sity,whichcanleadtoimmune-mediateddestructionofthe
attachmentapparatusandlossofsupportingalveolarbone.
Gingivitis,themostcommonformofperiodontaldisease,is
aninflammatoryprocesscharacterizedbyerythema,edema
andgingivalbleeding.Periodontitisischaracterizedby
gingi-valinflammationaccompaniedbyaninflammatoryresponse
bythehost,whichresultsindestructionoftheattachment
apparatusandlossofsupportingalveolarboneandthathave
systemiceffects.Thechangesfoundindentalevaluationof
periodontitisareanincreaseinprobingdepth(probingpocket
depth –PPD), whichreflects the distancefrom the bottom
ofthe pockettothe gingivalmargin, thepresenceof
clini-calattachmentloss(CAL),whichmeasuresthepositionofthe
softtissueinrelationtothecemento-enameljunction,and
theoccurrenceofgingivalbleedingonprobing(BOP),mobility
andtoothandalveolarboneloss.2
Theexistenceofimmunepathwaysandofagenetic
predis-positioncommontoPDandconnectivetissuediseases,among
thesesystemiclupuserythematosus(SLE),isrecognizedand
hasbeendescribed.1
In this brief communication, we reviewed studies
pub-lishedinEnglishorPortuguese,whichinvestigatedpossible
associationsbetweenPDandSLE,foundthrougha
system-aticsearchinPubMed/MedlineandLILACSdatabases,using
theterms“LupusErythematosus,Systemic”and
“Periodon-titis”,“Periodontitis,Chronic”or“Periodontitis,Adult”.There
wasnorestrictionaboutthesearchperiod.Twenty-two
arti-clesfromPubMed/MedlineandfivearticlesfromLILACSwere
found.Thirteenoriginalarticlesthatdealtwiththetopicwere
includedinthisreview.3–15Amanualsearchofthereferences
ofincluded articleswas carried out, and fivearticles were
selected.16–20
Studies
of
association
between
SLE
and
periodontal
disease
Casereportssuggestingthatclinicalandtherapeutic
associ-ations betweenSLEand PDhave been publishedsincethe
1980s,3–5 reportingagreaterseverityofPDinpatientswith
SLE,probablyassociatedwithimmunosuppressioncausedby
thedisease,oritstreatment.
ThefrequencyofperiodontitisinSLEpatientsvariedin
dif-ferentstudies,between60and93.8%(Table1).6–11AJapanese
study reportedthatSLEpatientshadahigher frequencyof
PD versus the generalpopulation of that country,9 but no
studyhascomparedthefrequencyofPDwithacontrolgroup
(healthyvolunteers).Thevariabilityofthefrequencyof
peri-odontitisfoundindifferentstudiesisprobablyassociatedwith
theuseofdifferentcriteriaforitsdiagnosis,ortodifferences
inpatientgroupswithSLEwithregardtodiseaseseverityor
activity.Thus,thequestion offrequencyofperiodontitisin
patientswithSLEremainsanopenone,andcontrolled
stud-iesareneededforsettingupwhetherperiodontitisisactually
morecommoninSLEpatients.
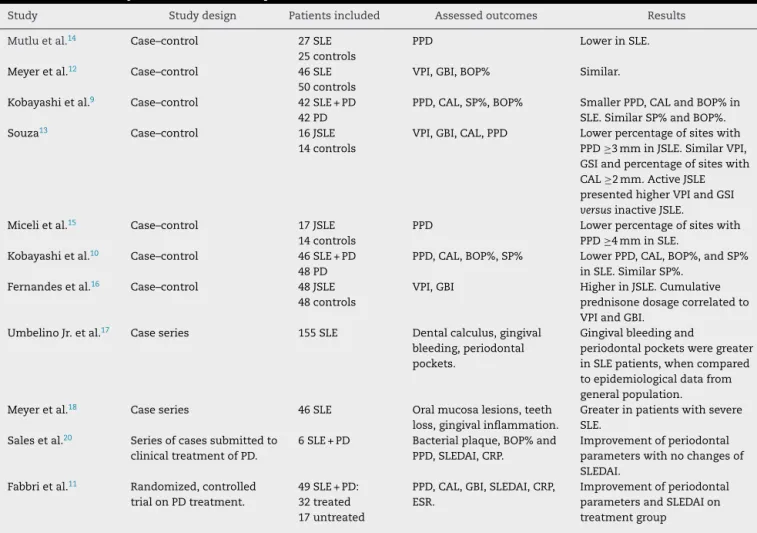
Several authors evaluated the severity of PD in SLE
patientscomparedtohealthyvolunteers,ortopatientswith
PD without SLE, and their results were conflicting.
Peri-odontal parameters were found to be: similar,9,10,12,13 less
severe,9,10,13–15ormoresevere16–18(Table2).
These controversial data prompted some questions as:
immunosuppressioninducedbySLEoritstreatmentwould
increase, would not affect,or would reducethe infectious
andinflammatoryperiodontaldestruction?Thestudiesthat
foundlowerseverityofperiodontalparametersinSLEsuggest
a smaller immune-mediated periodontal destruction
asso-ciatedwithimmunosuppressivedrugs.9,10,13–15 However,the
composition biasofthecontrol group,consistingprimarily
ofpatientsreferredforspecializedtreatmentandpotentially
withmoreseriousperiodontitis,wasnotcontrolled.Studies
werealsopublishedthatsuggestagreaterseverityofPDin
patientswithSLE,especiallywhenthediseaseisactive.16–18
Then, immunosuppression would increase the periodontal
decayassociatedwithchronicinfection?Thispointalsoisnot
definedandrequiresfurtherstudiesthatincludepatientswith
activeandinactiveSLE,evaluatingtheinfluenceofSLE
activ-ityandoftheimmunosuppressivetreatmentonperiodontal
parameters,withtheinclusionofacontrolgroup
representa-tiveofthegeneralpopulation,withpeoplewithandwithout
PD.
Biological
basis
of
the
association
between
SLE
and
PD
InPD,theguminfectiontriggersaseriesofimmuneresponses
thatinvolvetheparticipationofimmunecellsandcytokines,
that results in the destruction of the attachment
appara-tus and alveolar bone loss. A study reported an increase
Table1–PeriodontitisfrequencyinpatientswithSLE.
Study Numberofpatients
withSLE
Frequencyofperiodontitis observed
Frequencyofperiodontitis ingeneralpopulation
RhodusandJohnson6 16 93.8% Notreported
Novoetal.7,8 30 60% Notreported
Kobayashietal.9 60 70% 30–40%
Kobayashietal.10 71 64.8% Notreported
Fabbrietal.11 55 89% Notreported
and serum levelsof variouscytokines, including: IL-1␣,
IL-1,IL-6, IL-8,TNF-␣, TNF-,IFN-␥(inflammatory)and IL-10
(anti-inflammatory).19
ThereceptorsfortheconstantregionofimmunoglobulinG
(Fc␥R)participateintheimmuneresponse,facilitating
phago-cytosis by opsonization and acting in antibody-dependent
cellularcytotoxicityandintheactivationofthe toxic
gran-ule release by inflammatorycells. There isevidence of an
associationbetweencertaingeneticpolymorphismsofgenes
encoding these receptors and infectious and autoimmune
diseases. Kobayashi et al. 9,10 found higher expression of
Fc␥RIIa-R131 allele in patients with SLE and periodontitis
versuspatientswithSLEbutwithoutperiodontitis,andalso
healthy volunteers.9 These authors have also shown that
patientswithSLEandperiodontitisexhibitedthe
combina-tion ofpolymorphismsFc␥RIIa-R131andFc␥RIIB-232Tmore
oftenthanSLEpatientswithoutperiodontitis,patientswith
periodontitisbutwithoutsystemicdisease,andhealthy
vol-unteers.Combinedallelesalsowereassociatedwithgreater
severityofperiodontalparametersinpatientswithSLE.10
Ontheotherhand,sofar,studieshavenotidentifiedan
association betweenperiodontitisorperiodontalevaluation
parametersandevidenceofinflammatoryactivity(ESRand/or
CRP)inSLEorSLEDAI.13,16
Table2–PDseverityclassificationinSLEpatientsandtheinfluenceoftreatmentofadiseaseovertheother.
Study Studydesign Patientsincluded Assessedoutcomes Results
Mutluetal.14 Case–control 27SLE 25controls
PPD LowerinSLE.
Meyeretal.12 Case–control 46SLE 50controls
VPI,GBI,BOP% Similar.
Kobayashietal.9 Case–control 42SLE+PD 42PD
PPD,CAL,SP%,BOP% SmallerPPD,CALandBOP%in SLE.SimilarSP%andBOP%.
Souza13 Case–control 16JSLE
14controls
VPI,GBI,CAL,PPD Lowerpercentageofsiteswith PPD≥3mminJSLE.SimilarVPI, GSIandpercentageofsiteswith CAL≥2mm.ActiveJSLE presentedhigherVPIandGSI versusinactiveJSLE. Micelietal.15 Case–control 17JSLE
14controls
PPD Lowerpercentageofsiteswith PPD≥4mminSLE.
Kobayashietal.10 Case–control 46SLE+PD 48PD
PPD,CAL,BOP%,SP% LowerPPD,CAL,BOP%,andSP% inSLE.SimilarSP%.
Fernandesetal.16 Case–control 48JSLE 48controls
VPI,GBI HigherinJSLE.Cumulative prednisonedosagecorrelatedto VPIandGBI.
UmbelinoJr.etal.17 Caseseries 155SLE Dentalcalculus,gingival bleeding,periodontal pockets.
Gingivalbleedingand
periodontalpocketsweregreater inSLEpatients,whencompared toepidemiologicaldatafrom generalpopulation. Meyeretal.18 Caseseries 46SLE Oralmucosalesions,teeth
loss,gingivalinflammation.
Greaterinpatientswithsevere SLE.
Salesetal.20 Seriesofcasessubmittedto clinicaltreatmentofPD.
6SLE+PD Bacterialplaque,BOP%and PPD,SLEDAI,CRP.
Improvementofperiodontal parameterswithnochangesof SLEDAI.
Fabbrietal.11 Randomized,controlled trialonPDtreatment.
49SLE+PD: 32treated 17untreated
PPD,CAL,GBI,SLEDAI,CRP, ESR.
Improvementofperiodontal parametersandSLEDAIon treatmentgroup
Twostudiesexaminedinflammatorycytokinesingingival
crevicularfluid(whichcanbefoundinperiodontalpockets)
andinserum.Souza13foundhighercrevicularfluidlevelsof
totalandfreeelastaseandlowercrevicularfluidlevelsof
IL-18,buthigherserumlevelsofIL-18inpatientswithjuvenile
SLEversuscontrolgroup.CALshowedanegativecorrelation
withcrevicularfluidIL-18levels(r=−0.5;p<0.05),suggesting
thatthiscytokinecouldhaveaprotectiveeffectonthetissue
destructionassociatedwithPD.InthestudybyMicelietal.,15
healthyadolescentshadhigherlevelsofIL-1-increvicular
fluidversuspatientswithjuvenileSLEwhowereevaluatedfor
presenceofperiodontaldisease.
Twostudiesevaluatedtheassociationbetweenthe
pres-ence of antineutrophil cytoplasmic antibodies (ANCA) and
periodontitisinsubjects withoutrheumatic disease and in
patientswithSLEorrheumatoidarthritis(RA).7,8 Halfofthe
subjectswithperiodontitiswerepositiveforANCA.Amongthe
18patientswithSLEandperiodontitis,83.3%werepositivefor
ANCA.HalfofthepatientswithRAhadperiodontitis,butthis
diseasewasnotassociatedwithahigheroccurrenceofANCA.
ThesignificanceoftheassociationbetweenANCAand
peri-odontitisinhealthysubjectsorinpatientswithSLEremains
unclear.7,8
Insummary,thereisevidenceofacommongenetic
predis-position(sharedpolymorphisms)ofSLEandPD,whichcould
explaintheassociationbetweenthesetwoconditions.Still,at
leastfromatheoreticalpointofview,thereare
pathophysio-logicalmechanismscommontoPDandLESthatneedtobe
betterdescribedandunderstood,becausetheymayrepresent
prospectsforfuturetherapeuticapproaches.
Specific
treatment
and
influence
on
SLE
and
periodontal
disease
Fernandesetal.16 foundapositivecorrelationbetweenthe
cumulativedose ofcorticosteroidsand increasesinplaque
and gingival bleeding rates in patients with juvenile SLE
(respectively, r=0.385, p=0.01; r=0.471; p=0.001), but did
notidentifyanassociationwiththeuse ofantimalarialsor
immunosuppressiveagents(Table2).16
TwostudiesevaluatedtheinfluenceofthetreatmentofPD
onSLEactivity(Table2).Salesetal.20selectedsixpatientswith
SLE(meanofSLEDAI=3.5)and PD.Thepatientsunderwent
non-surgicaltreatmentofperiodontitisandwerereassessed
45daysafteritscompletion.Therewassignificant
improve-mentintheirperiodontalindices.SLEDAIandCRPlevelsdid
notchangesignificantlyafterperiodontaltreatment.20
Fabbri et al.11 selected 49 patients withactive SLE and
PD,dividedintotwogroups:onegroupwithtreatmentofPD
performedduringthestudy(n=32)andagroupwhose
treat-mentofPDwasdelayedforatimeaftercompletionofthe
study.TherewasnosignificantdifferenceinbaselineSLEDAI
in treated and control groups. Patients were reassessed 3
monthsafterthetreatmentofPD,whenasignificant
reduc-tioninSLEDAIwasobservedinthetreatmentgroup(5.9±4.2
vs.3.4±3.3,p=0.04),butdidnotoccurintheuntreatedgroup.
NosignificantdifferenceswerenotedinESRorCRPinboth
groups(Table2).11
Thehighestcumulativedoseofcorticosteroids,givenlocal
and systemic immunosuppressiveand metabolic effectsof
theseagents(withaninterferenceinbonemetabolism),could
beassociatedwiththeworstoutcomeoftheinfectious
pro-cessand,consequently,withgreaterperiodontaldestruction
inpatientswithSLEandPD.Studiesareneededtoestablish
whethertheconcomitantuseofimmunosuppressantswould
haveaprotectiveeffector,onthecontrary,wouldcontribute
togreaterperiodontaldestructioninSLEandPDpatients.
StudiesevaluatingtheinfluenceofPDtreatmentonSLEDAI
inSLEpatientsshowedconflictingresults.Onestudy,which
showed no change inSLEDAI, included asmall number of
patientswithouthighactivityofthedisease.20Anotherstudy
evaluated agreater numberofpatientswithactiveSLE, all
onmonthlyintravenousinfusionsofcyclophosphamideand
corticosteroids, and showed significant decline in SLEDAI,
compared tobaseline,in patientstreated forperiodontitis,
whichdidnotoccurinthegroupuntreatedforthisdisease;
thissuggestsapossibleroleofthetreatmentofperiodontitis
inthecontrolofactiveSLE.11Thisresultisquiteinteresting,
becauseitopensuppromisingprospectsinSLEapproaches,
howeveritmustbeconfirmedbyprospectivecontrolled
stud-ies.Theoretically,thecontrolofchronicinfectionrelatedto
PDcouldreducethedegreeofactivationoftheimmune
sys-tem,favoringtheresponseofSLEtotheimmunosuppressive
treatment.
Conclusion
The data about possible associations between SLE and PD
arecontroversial.Thegoodclinicalpractice,however,
recom-mendsattentiontotheoralhealthofpatientswithSLE,ideally
withperiodicdentalevaluation.IntheeventofPD
identifica-tion,itstreatmentshouldbeperformed,asitcanpositively
influencethehoweverofSLE.Furtherstudieswillbeneededto
establishtheassociationbetweenSLEandPD,aswellastheir
biologicalbasis,andtoclearlydefinetheeffectoftreatment
ofaconditionovertheother.
Conflict
of
interests
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.GonzalesTS,ColemanGC.Periodontalmanifestationsof collagenvasculardisorders.Periodontology2000. 1999;21:94–105.
2.WilderRS,MorettiAJ.Gingivitisandperiodontitisinadults:
classificationanddentaltreatment.In:UptoDate.Available
from http://www.uptodate.com/contents/gingivitis-and- periodontitis-in-adults-classification-and-dental-treatment?source=searchresult&selectedTitle=1%7E97
[accessed27.02.14].
3.VogelRI.Periodontaldiseaseassociatedwith
4. JaworkskiCP,KoudelkaBM,RothNA,MarshallKJ.Acute necrotizingulcerativegingivitisinacaseofsystemiclupus erythematosus.JOralMaxillofacSurg.1985;43:43–6.
5. NaglerRM,LorberM,Ben-AriehY,LauferD,PollackS. Generalizedperiodontalinvolvementinayoungpatientwith systemiclupuserythematosus.Lupus.1999;8:770–2.
6. RhodusNL,JohnsonDK.Theprevalenceoforal manifestationsofsystemiclupuserythematosus. QuintessenceInt.1990;21:461–5.
7. NovoE,MacGregorEG,NavaS,PeriniL.Apossibledefective estimationofantineutrophilcytoplasmicantibodiesin systemiclupuserythematosusduetothecoexistenceof periodontitis:preliminarobservations.PRJSJ.1997;16:369–73.
8. NovoE,Garcia-MacGregorE,VieiraN,ChaparroN,CrozzoliY. Periodontitisandanti-neutrophilcytoplasmicantibodiesin systemiclupuserythematosusandrheumatoidarthritis:a comparativestudy.JPeriodontol.1999;70:185–8.
9. KobayashiT,ItoS,YamamotoK,HasegawaH,SugitaN, KurodaT,etal.Riskofperiodontitisinsystemiclupus erythematosusisassociatedwithFc␥receptor polymorphisms.JPeriodontol.2003;74:378–84.
10.KobayashiT,ItoS,YasudaK,KurodaT,YamamotoK,Sugita N,etal.Thecombinedgenotypesofstimulatoryand inhibitoryFc␥receptorsassociatedwithsystemiclupus erythematosusandperiodontitisinJapaneseadults.J Periodontol.2007;78:467–74.
11.FabbriC,FullerR,BonfáE,GuedesLK,D’AllevaPS,BorbaEF. Periodontitistreatmentimprovessystemiclupus
erythematosusresponsetoimmunosuppressivetherapy.Clin Rheumatol.2014;33:505–9.
12.MeyerU,KleinheinzJ,HandschelJ,Kruse-LöslerB,Weingart D,JoosU.Oralfindingsinthreedifferentgroupsof
immunocompromisedpatients.JOralPatholMed. 2000;29:153–8.
13.SouzaAA.Condic¸õesperiodontaisempacientescomlúpus eritematososistêmicojuvenil.TeseapresentadaàFaculdade deOdontologiadaUERJ,comorequisitoparaobtenc¸ãodo títulodeDoutoraemPeriodontia,RiodeJaneiro;2006.p.70.
14.MutluS,RichardsA,MaddisonP,ScullyC.Gingivaland periodontalhealthinsystemiclupuserythematosus. CommunityDentOralEpidemiol.1993;21:158–61.
15.MiceliVC,BragaF,ÁreasA,FigueredoCMS,SztajnbokF, FischerRG.Condic¸õesclínicaseníveisdeIL1-empacientes adolescentescomlúpuseritematososistêmico.RPeriodontia. 2006;16:21–7.
16.FernandesEGC,SaviolliC,SiqueiraSTT,SilvaCAA.Oral healthandthemasticatorysysteminjuvenilesystemiclupus erythematosus.Lupus.2007;16:713–9.
17.UmbelinoAAJr,CantisanoMH,KlumbEM,DiasEP,SilvaAA. Achadosbucaiselaboratoriaisempacientecomlúpus eritematososistêmico.JBrasPatolMedLab.2010;46: 479–86.
18.MeyerU,KleinheinzJ,GaubitzM,SchulzM,WeingartD,Joos U.Oralmanifestationsinpatientswithsystemiclupus erythematosus.MundKieferGesichtschir.1997;1:90–4 [abstract].
19.AgarwalS,SuzukiJB,RiccelliAE.Roleofcytokinesinthe modulationofneutrophilchemotaxisinlocalizedjuvenile periodontitis.JPeriodontRes.1994;29:127–37.