Universidade de Lisboa Faculdade de Medicina Dentária
Insights on the Thermal Aging of
Acrylic Reline Resins
Filipe Gaudêncio Pacheco
Dissertação
Mestrado Integrado em Medicina Dentária
Universidade de Lisboa Faculdade de Medicina Dentária
Insights on the Thermal Aging of
Acrylic Reline Resins
Filipe Gaudêncio Pacheco
Dissertação orientada pela Professora Doutora Maria Cristina Bettencourt Neves e coorientada pela Professora Doutora Ana Francisca Bettencourt
Mestrado Integrado em Medicina Dentária
Table of Contents i TABLE OF CONTENTS Agradecimentos ii Resumo iv Abstract viii 1. Introduction 1 2. Objectives 5
3. Materials and methods 6
3.1 Preparation of the specimens 7
3.2 Thermocycling aging process 8
3.3 Mass determination 9
3.5 Analitical methodology 9
3.6 In vitro release studies 12
3.7 Statistical Analysis 13
4. Results 15
4.1 The effect of thermal aging in mass variation 15 4.2 The effect of Thermal aging on color variation 16
4.3 CHX release 17
4.3.1 CHX quantification 17
4.3.2 The effect of different materials on the drug release 18
5. Discussion 20
6. Conclusion 25
7. References 28
Appendices 30
Appendice 1- List of Tables 31
Appendice 2- List of Figures 32
Agradecimentos
AGRADECIMENTOS
A produção deste trabalho contou com a colaboração de várias pessoas. a quem quero deixar os meus sinceros agradecimentos
À minha orientadora Professora Doutora Maria Cristina Bettencourt Neves, Professora Auxiliar da disciplina de Prostodontia Removível da Faculdade de Medicina Dentária da Universidade de Lisboa a quem quero agradecer por toda a confiança, amizade, orientação científica, disponibilidade e incentivo ao longo da elaboração desta tese de Mestrado. Tem sido sem dúvida uma grande referência pelo seu enorme sucesso profissional e qualidades humanas que muito valorizo.
À minha co-orientadora Professora Doutora Ana Francisca Bettencourt, Professora Auxiliar da Unidade Curricular de Dispositivos Médicos e Física do Departamento de Ciências Toxicológicas e Bromatológicas da Faculdade de Farmácia pelos ensinamentos e acompanhamento na realização do trabalho experimental e pela disponibilidade, apoio e incentivo com que sempre me orientou.
À minha colega Fábia Alexandre por toda a sua ajuda, tempo, simpatia e companheirismo ao longo deste projecto.
Gostaria também de agradecer aos meus amigos e colegas de turma que muito contribuíram para a minha alegria e crescimento pessoal ao longo destes últimos anos em especial à Tiffany Pinto, Mara Ramos, Carolina de Sá, Pedro Gomes, Sara Mendes, Isabel Rodrigues e Catarina Serra por todos os momentos fantásticos e pela verdadeira amizade que me têm dedicado.
Ao João Pedro Rosa que foi sem dúvida das melhores pessoas que surgiram na minha vida. O seu companheirismo, carinho, atenção e dedicação revelaram-se
Agradecimentos
iii À Isabel Lucas por ter sido a pessoa que mais me acompanhou durante toda esta caminhada. A sua amizade, carinho e dedicação foram absolutamente fundamentais para a minha felicidade e crescimento pessoal. É, sem dúvida uma pessoa que representa um exemplo perfeito de combinação entre excelentes valores humanos com um grande sucesso académico e profissional.
Ao Duarte Afonso que muito admiro pela extraordinária pessoa que é. Não podia deixar de agradecer pela amizade e apoio absolutamente incondicional com que me tem presenteado nestes últimos anos. A sua coragem, espirito de sacrifício,
dedicação e bondade serão para sempre uma grande referência na minha vida.
Aos docentes, alunos e funcionários da Faculdade de Medicina Dentária da Universidade de Lisboa que contribuíram para a minha formação pessoal e profissional.
À minha família, em especial aos meus pais pelo seu amor incondicional, respeito, apoio, carinho e confiança que depositaram em mim desde sempre. São a minha principal fonte de força e eles devo grande parte do meu sucesso e felicidade.
Resumo
RESUMO
Apesar dos métodos e campanhas de prevenção aplicados no sentido de melhorar a saúde oral, a perda de peças dentárias ainda é um problema prevalente numa população significativa de idosos. Assim sendo, e tendo em conta o envelhecimento da população prevê-se um aumento na utilização de próteses totais ou parciais por um elevado número de pacientes no futuro.
As resinas acrílicas de rebasamento são materiais utilizados de forma frequente em medicina dentária. A sua principal função é a adaptação das próteses removíveis a alterações causadas nos tecidos de suporte após a perda de dentes.
A estomatite protética é uma condição recorrentemente observada em portadores de próteses removíveis. Esta patologia tem múltiplas causas (trauma, xerostomia, uso continuo da prótese) mas associa-se principalmente à infecção por espécies Candida, principalmente Candida albicans cuja capacidade de aderir a células hospedeiras ou a polímeros como as resinas acrílicas é uma característica essencial para a patogénese da infecção.
Atualmente, a terapêutica da estomatite protética é feita principalmente pela aplicação de fármacos através de um regime periódico por via tópica ou sistémica. Este método tem-se mostrado pouco eficaz principalmente devido a problemas de adesão à terapêutica por parte dos pacientes e à dificuldade em manter a dose necessária no local afectado por longos períodos de tempo. Desta forma foi necessária investigação no sentido de encontrar novas modalidades de tratamento.
Recentemente foi proposta a utilização de agentes de libertação controlada para o tratamento da estomatite protética. Esta intervenção terapêutica baseia-se na incorporação de fármacos em materiais como as resinas acrílicas com o objectivo de serem libertados de forma lenta e controlada. Os estudos indicam que estas formulações têm a capacidade de manter níveis terapêuticos no local pretendido muitas vezes superiores à concentração mínima inibitória das espécies alvo e por longos períodos de tempo. Adicionalmente, estes veículos são praticamente independentes da adesão à terapêutica do paciente e estão associados a menor interacção medicamentosa e efeitos colaterais. Apesar de vários fármacos terem sido incorporados em resinas acrílicas, a clorexidina tem mostrado os resultados mais promissores. A evidência tem demonstrado
Resumo
vi que este antisséptico reduz a capacidade de adesão da C. albicans à superfície das próteses dentárias (processo essencial para a formação de biofilme) e não causa o aparecimento de estripes resistentes.
No entanto, a literatura carece de estudos que avaliem as alterações físicas provocadas nas resinas acrílicas aquando da sua incorporação com clorexidina e submetida a processos de envelhecimento.
Assim sendo, os objectivos do presente estudo foram o de avaliar a estabilidade de cor e variação de massa de duas resinas acrílicas de rebasamento directo (Ufi Gel Hard e Kooliner) e uma de rebasamento indirecto (Probase Cold) com diferentes concentrações de clorexidina incorporada, após submetidas a termociclagem, e o estudo posterior de libertação do fármaco destas resinas ao longo de 28 dias.
Para cada um dos materiais foram produzidos 5 grupos de espécimes, um de controlo e 4 com diferentes concentrações de clorexidina incorporada (2.5%, 5%, 7.5% e 10%). Foram avaliados um total de 45 espécimes em forma de cilindro (12mm de comprimento por 6mm de diâmetro). Os espécimes foram pesados numa balança de precisão e registada a sua massa e foi feita a avaliação da cor com auxílio de um espectrofotómetro antes e após a termociclagem. Após a termociclagem, de modo a estudar a libertação da clorexidina pelos espécimes, os cilindros foram armazenados individualmente em frascos graduados de 5mL e cobertos por saliva artificial, num rácio de 1g/5mL. Estes foram posteriormente incubados a 37ºC e, em intervalos de tempo específicos (2, 4, 7, 24, 48, 72, 144, 168,192,216, 240, 336, 504, 672 horas), foram pipetados 450μL a partir de cada frasco para uma placa de micropoços. As amostras foram de seguida analisadas num espectrofotómetro a 255nm e as absorvâncias foram convertidas em concentrações. Nos mesmos intervalos de tempo, 450μL de saliva artificial foram renovados em cada frasco, de modo a simular a constante renovação salivar.
Foi realizada a análise estatística dos dados dos espécimes incorporados, de forma a verificar a existência de diferenças significativas entre os materiais e entre concentrações. Tendo em conta que os dados não apresentavam uma distribuição normal para as variáveis em estudo, os resultados foram submetidos a testes não paramétricos pelo método de Kruskall-Wallis. Para tal, foi considerado um nível de significância igual a 5%.
Resumo
Relativamente à variação de massa, observou-se que houve variação estatisticamente significativa antes e após a termociclagem. Nos espécimes de Probase Cold a incorporação do fármaco não causou alterações na variação de massa comparadas com o controlo. Por outro lado, para o Ufi gel Hard e para o Kooliner, a presença de clorexidina conduziu à perda de massa. Esta perda foi mais significativa no Ufi Gel Hard do que no Kooliner. Observou-se ainda que para os grupos controlo em todos os materiais houve um aumento de massa. Considera-se que estes resultados estão associados a alterações físicas já avaliadas em outros estudos como solubilidade e formação de poros na superfície do material que ocorrem quando são sujeitos a alterações térmicas. Acredita-se que estas alterações físicas condicionem a libertação de clorexidina do material e facilitem a entrada de água o que pode justificar estas alterações de massa.
Acerca da estabilidade de cor após a termociclagem, houve variação de cor em todos os materiais e a variação foi diferente entre diferentes resinas. Probase Cold foi o que teve a maior variação de cor seguido do Ufi Gel Hard e do Kooliner. Verificou-se, no entanto, que a presença de clorexidina incorporada não condicionou de forma estatisticamente significativa a mudança de cor em nenhum dos materiais. Tendo em conta que a clorexidina não teve influência significativa, pensa-se que a justificação para os resultados se prenda novamente com os mecanismos já descritos de entrada de água no material.
No que diz respeito à libertação de clorexidina, os resultados mostraram que apenas o Probase Cold teve valores de quantificação de clorexidina superiores ao limite de detecção do método utilizado. Para este material, foi observado que independentemente da concentração de clorexidina, a libertação teve um início rápido e crescente seguido de uma libertação mais lenta e constante até ao final do estudo. Este comportamento está de acordo com a literatura que o justifica com fenómenos iniciais de libertação rápida do fármaco que está à superfície com a posterior libertação lenta do fármaco que se encontra no interior da resina. Observou-se igualmente, que maiores percentagens de clorexidina incorporadas tiveram maiores valores de libertação (μg/mL). Também se verificou que a clorexidina libertada (μg/mL) às 48 horas foi sempre superior a 4.78 μg/mL valor este que de acordo com outros estudos, representa a concentração mínima inibitória para a candida albicans. Observou-se ainda que a percentagem máxima de clorexidina libertada (w/w) foi de apenas 1.94% o que significa
Resumo
que grande parte do fármaco não se libertou durante o período de incubação. Este resultado foi também observado de forma semelhante em outros estudos.
Relativamente às limitações do estudo, a forma cilíndrica dos espécimes não reproduz superfície protética. Surge a necessidade de fazer estudos que avaliem a rugosidade e formação de poros nas resinas acrílicas com clorexidina incorporada após a termociclagem bem como outros estudos microbiológicos e de biocompatibilidade.
O presente estudo conclui que os sitemas de libertação de clorexidina em resinas acrílicas de rebasamento poderão vir a ser uma boa alternativa no tratamento da estomatite protética .
Palavras-chave: Estudos de libertação; Clorexidina; Termociclagem; Resinas acrílicas; Estomatite protética.
Abstract
ABSTRACT
The use of controlled-release agents has being studied as therapeutic alternatives for the treatment of denture stomatitis.
The main purpose of this study was to evaluate mass variation color stability and drug release of acrylic reline resins loaded with chlorhexidine after thermal aging. Three different materials were evaluated in the present study, Kooliner, Ufi Gel Hard and Probase Cold. For each, one control group and four experimental groups with chlorhexidine (2.5%, 5%, 7.5% and 10% (w/w)) were produced. A total of 45 cylinder-shaped specimens were evaluated. Mass was calculated using a precision scale and color was evaluated using a spectrophotometer. These measurements were made before and after a thermocycling aging procedure of 1000 cycles of thermal fluctuations between 5ºC and 55ºC (20 seconds each bath). After that, the cylinders were stored individually in graduated falcon tubes and covered with saliva at pH=7. The falcons were then placed into an incubator and, at specific time intervals, an aliquot were collected from each falcon and the same amount of artificial saliva was renovated, in order to simulate the constant salivary renovation. The samples were analyzed by UV-spectroscopy and chlorhexidine content was determined. Data were submitted to nonparametric tests according to Mann-Whitney and Kruskall Wallis methods (p<0.05). Results showed that thermocycling caused variationsin mass in all the materials. For Ufigel and Kooliner specimens, chlorhexidine incorporation caused a mass decrease when compared to control. However, clorhexidine incorporation didn’t affect mass variation on Probase Cold. It was also observed that thermocycling caused color variation in all the specimens but chlorhexidine incorporation didn’t affect the color stability. Color variation was higher in Probase Cold followed by Ufi Gel Hard and Kooliner. after thermocycling, it was perceived that only Probase Cold released chlorhexidine whose quantification was superior to 0.6 μg/mL (minimum detectable capacity of the technique used).
Overall, results indicate that chlorhexidine delivery systems based on acrylic reline resins are a potential approach in the treatment of denture stomatitis.
Keywords: Thermocycling; Release studies; Chlorhexidine; Acrylic resins; Stomatitis
Introduction
11 INTRODUCTION
Tooth loss is considered one of the most common oral health complications among the elderly population. This unfortunate situation is a result of an accumulation of preventable oral health diseases experienced during a lifetime such as periodontal disease or dental caries (Jones et al. 2003; Pisani et al. 2011). ( Jones et al. 2003 )
One of the consequences of tooth loss is the alveolar resorption. This process is continuous and progressive and will cause the desadaptation in local areas of the denture base (Reis et al., 2006; Urban et al., 2007b; Kranjcic et al., 2013, Lyu X, 2016)). Therefore it is very important to make a periodic exam to detect the changes in the adaptation of the denture. (Reis et al., 2006)
A relining procedure is made to overcome the problem of bone resorption, it consists in resurfacing the base of a denture with a new material in order to fill the existing space between the original denture contour and the altered tissue, improving the retention, stability and support of the prosthesis (Ahmad et al., 2009; van Meegen and Kalk, 2011). Some of the materials that can be used to this procedure are the acrylic resins, they consist of polymeric biomaterials and can be classified as chemical, heat or light activated.( Koran III 2002)
The majority of dentures worldwide are fabricated form acrylic resins whose good characteristics like good thermal conductivity, low price and ease of manipulation contribute to its preference. However, acrylic resins still have some handicaps like discoloration and change of physical properties over time (Salloum, 2014) With the prevalence of 45-70%, candida-associated dentures stomatitis is a very common chronic inflammatory disease among denture wearers. Although it’s a multifactorial disease (associated with trauma from ill-fitting dentures, bad oral hygiene, reduced saliva secretion, broad spectrum antibiotic disease, immunologic disease among others) the main cause is the presence of Candida albicans and biofilm formation. (Redding et al. 2009; Rautemaa and Ramage 2011, Lyu X, 2016)) When symptomatic, it’s main clinical sign is a diffuse inflammation of the denture-bearing areas (Chandra et al. 2001; Amin et al. 2009; Cao et al. 2010;da Silva et al. 2011; Ryalat et al. 2011; Salim, Moore,
et al. 2012a)
1 vi
Introduction
Candida albicans is a fungal organism that act as an opportunistic pathogen
(Patel et al. 2001; Bertolini et al. 2014, Lyu X, 2016)) and it is the principal agent contributing to this disease. There is evidence indicating that Candida is able to adhere to acrylic resin dentures, namely to polymethylmethacrylate (PMMA) and Polyethilmethylmethacrylate (PEMA) and form biofilms that are a crucial to the pathogeny of stomatitis. (Chandra et al, 2001;Salim Moore, et al 2012; Pereira, 2008, Figueiral, 2015)
Currently, the treatment of denture stomatitis includes the mechanical and chemical control of plaque, the respect of the rest periods of denture wearing and also the use of antimicrobial agents (Silva 2011, Figueiral, 2015). Systemic and topic antifungal treatment is advised but recurrences are frequent (Figueiral, 2015) and one of the problems is that it requires a daily compliance with the appropriate dosage to maintain its efficacy (Salim 2012). An example of this situation is Nystatin that, despite its good efficacy, it requires four applications daily (Moore, et al. 2012; Salim, Moore et al. 2013, Lyu X, 2016)
Fluconazole is a commonly used systemic antifugal due to its low toxicity and mild side effects. However, it doesn’t present a good long term efficiency and it has been related to the emergence of resistant strains of C.albicans (Chandra et al. 2001;Redding et al. 2009; da Silva et al. 2011). This way, it is recommended to take other therapeutic/prevention strategies before fluconazole, and leave it to cases of immunodeficiency or to severe cases of stomatitis (Figueiral, 2015).
Many studies have shown that chlorhexidine is able to supress the ability of
candida albicans to adhere not only to the buccal epithelal cells but also to the surface
of the acrylic denures. (Bertolini et al. 2014 ; da Silva et al. 2011; Peter A. Suci, 2002; Shino B, 2016). Also, it has been proved that chlorhexidine compared to fluconazole, has a higher efficacy against candidal biofilms and, so far, it has not been observed the emergence of resistance strains (Salim, Silikas, et al. 2013b). Chlorhexidine has a good substantivity but, in fact, most of the agent is dissolved and removed from the oral cavity thanks to the renovation of saliva and self-cleaning effect of the oral musculature. According to that, the efficacy of the topical agents is limited to a short term action. (Ryalat et al. 2011; Salim, Moore, et al. 2013a)
Introduction
.3 To overcome the problem of topical substantivity in the treatment of stomatitis it was suggested the use of drug carriers and controlled-release agents (Riggs et al. 2000; Salim, Silikas, et al. 2013b). In this method, the antifungal or antimicrobial agent is impregnated into the material in order to be released slowly overtime. This way, it will maintain satisfying therapeutic levels of the medication at the spot of infection (Amin et
al. 2009) being able to exceed, in some cases, the minimum inhibitory concentration candida albicans (MIC) (Gong et al. 2007)(Salim, 2013) . One of the advantages of this
therapeutic methodology is that the therapeutic effect is achieved with less amount of drug, contributing to a decrease in lateral effects or drug-drug interactions (Bertolini et
al. 2014). Another benefit is that it is non-compliance-dependent which is especially
good to physically or mentally disabled patients (Amin - 2009; Salim 2012; S. J. Wilson and H. J. Wilson 1993;).
Spectroscopy is an easy and reliable method that can measure the release of chlorhexidine from the acrylic resins (Amin et al. 2009; Ryalat et al. 2011; Salim, Moore, et al. 2012a)
However, it is assumed that the physical properties of the acrylic resins will be altered in the presence of the drug’s particles. This alteration is caused by de dissolution of the material and porous formation. Furthermore, the porous formation into the material will encourage drug release and increase water uptake (Amin,2009; S. J. Wilson and H. J. Wilson 1993; Hiraishi et al. 2008 )
Regardless of the big variety of antifungal agents and polymeric systems that have been proposed and studied for oral use as controlled release agents, chlorhexidine is considered one of the best agents to be incorporated in acrylic resins for its better results in terms of releasing and microbial tests (Amin et al. 2009; Gong et al. 2007; Redding et al. 2009; Salim, Moore, et al. 2012a).
Evidence shows that the release of chlorhexidine from the acrylic resins depends on its concentration. Also, it has been witnessed that bigger concentrations are released initially supposedly because it represents the release of the drug that is on the surface of the material. Afterwards it starts a second phase where it is observed a slow release of the medicine. That release is a result of a complex process that involves the formation of fluid clusters around the drug molecules Those clusters will interact with the fluid absorption of the acrylic resins (Amin et al 2009; Thaw 1982 )
Colour stability is a very important clinical property as it is related to anging or damaging of the materials (Salloum, 2014) Incomplete polimeryzation, diet, oral
Introduction
.3 hygiene, water sorption and surface rugosity of the material are some of the factors that can affect the amount of colour change in an acrylic resin (S.-K. PARK, 2004; Hatim & Al-Tahho, 2013a) .Colour determination should be accurately measured with spectrophotometers (S.-K. PARK, 2004; Hatim & Al-Tahho, 2013a;)
The international Commission on illumination (CIE) l*a*b system is widely used in dentistry in order to evaluate variations in color in dental materials. The colorimeters are able to measure three parameters of color : l (lightness) a ( red/green) and b (yellow/blue). The color difference between two samples is represented as ΔE. If ΔE > 3.3 then the color difference is perceptible by humans. (Hatim & Al-Tahho, 2013b)
Colour stability is a very important clinical property as it is related to anging or damaging of the materials (Salloum, 2014) Incomplete polimeryzation, diet, oral hygiene, water sorption and surface rugosity of the material are some of the factors that can affect the amount of colour change in an acrylic resin (S.-K. PARK, 2004; Hatim & Al-Tahho, 2013a) .Colour determination should be accurately measured with spectrophotometers (S.-K. PARK, 2004; Hatim & Al-Tahho, 2013a;)
The international Commission on illumination (CIE) l*a*b system is widely used in dentistry in order to evaluate variations in color in dental materials. The colorimeters are able to measure three parameters of color : l (lightness) a ( red/green) and b (yellow/blue). The color difference between two samples is represented as ΔE. If ΔE > 3.3 then the color difference is perceptible by humans. (Hatim & Al-Tahho, 2013b)
Other authors have studied the release of chlorhexidine from acrylic resins, but they used distilled water as media solution and they didn’t study the effects of thermocycling on color and weight variation on the acrylic resins with chlorhexidine incorporation (Hiraishi et al. 2008;Salim, Moore, et al. 2012a; Bertolini et al. 2014). In the present study it was used artificial saliva at pH 7 to simulate the release in the oral cavity. Also, the period of analysis was 28 days, allowing comparisons with other studies (Hiraishi et al. 2008; Salim, Moore, et al. 2012a; Salim, Silikas, et al. 2013b). In addition, four different percentages of chlorhexidine incorporation were evaluated, as opposed to the other studies so far that only studied the release of chlorhexidine in one concentration.
Objectives
5 2. OBJECTIVES
The main objective of this study was to evaluate the effect of a thermal aging procedure on the weight and color of three different acrylic reline resins with different percentages of chlorhexidine incorporated, according to the following hypotheses:
H0: Thermocycling doesn’t affect the mass of reline resins with incorporated CHX
H1: Thermocycling affects the mass of reline resins with incorporated CHX
H0: Thermocycling doesn’t affect the color of reline resins with incorporated CHX.
H1: Thermocycling affects the color of reline resins with incorporated CHX.
Another purpose was to evaluate the release of chlorhexidine from acrylic reline resins after thermocycling, in particularly:
1. The effect of different materials composition (Kooliner, Ufi Gel Hard and Probase Cold) on the drug release;
2. The effect of different chlorhexidine loading percentages ( 2.5%, 5%, 7.5% and 10%) on the drug release.
Materials and Methods
3. MATERIALS AND METHODS
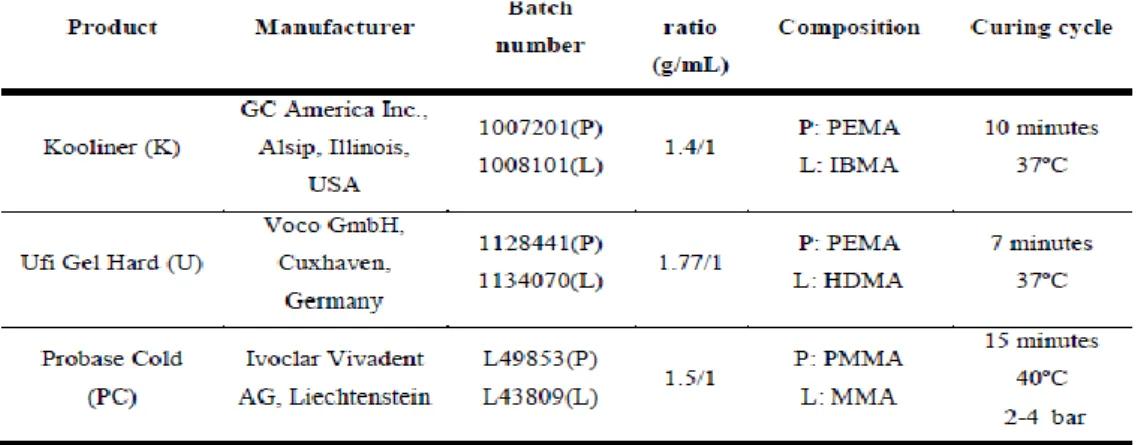
In the present study, it was used three auto-polymerizing acrylic resins (Table 3.1) presented in the powder-liquid form. Two of them are direct reline resins: a non-crosslinking material, Kooliner (GC America Inc, Alsip, Illinois, USA) (Figure 3.1a), and a crosslinking material, Ufi Gel Hard (voco GmbH,Cuxhaven, Germany) (Figure 3.1b) and one indirect reline resin, Probase Cold ( Ivoclar Vivadent AG,
Liechenstein)(Figure 3.1c) that has methylmethacrylate (MMA) as the monomer (Arima et al.,1995 and 1996).
Figure 3.1 Materials under evaluation in the study : a) Kooliner; b) Ufi Gel Hard; c) Probase Cold Table 3.1- Materials under evaluation in the study
Materials and Methods
7 3.1 Preparation Of The Specimens
The acrylic resins were manipulated according to the manufacturer’s instructions (Table 3.1). The powder was weighed using a precision balance (Mettler Toledo) and the liquid was measured using a pipette. On the experimental specimens, chlorhexidine diacetate monohydrate (CHX) ( Panreac Applichem, Darmstadt, Germany) (Figure 3.2a) was incorporated at a proportion of 2.5%, 5%, 7.5% and 10% of the acrylic resin’s powder weight (w/w) and mixed using a mortar and pestle for homogenization (figure 3.2b)
Five groups of specimens were produced for each material (one control group without CHX and four experimental groups using the CHX percentages mentioned), that resulted in fifteen specimens per material (n=15), three of each group (Table 3.2).
The cylinder-shaped specimens with the size of 12mm height and 6m diameter (Figure 3.2c) were produced using stainless steel molds (Figure 3.2b). A total of 45 specimens were prepared for this study.
Figure 3.2 Preparation of the specimens: a) Package of the Chlorhexidine diacetate monohydrate: b) Incorporation and homogenization of the CHX; c) shaped specimens d)
Materials and Methods
In each preparation of Kooliner and Ufi Gel specimens, the materials dough was poured into the cylinder-shaped molds, maintained at the temperature of 37±2ºC, during the recommended polymerization time (Table 3.1) in order to simulate the intraoral polymerization of direct reline resins. Polymerization of the indirect reline resin was carried out in a pressure device (Ivomat,Ivoclar Vivadent, Liechenstein)(Figure 3.3) at recommended time, temperature and pressure (Table 3.1)
3.2 Thermocycling Aging Process
All the specimens (n=45) were exposed to a thermocycling aging procedure of 1000 cycles of thermal fluctuations between 5ºC and 55ºC (20 seconds each bath), with 5 seconds of dwell time, in a specific machine (Refri 200-E, Aralab, Cascais, Portugal) (Figure 3.4).
Figure 3.4 - Thermocycling equipment Figure 3.3 Ivomat pressure device
Materials and Methods
9 3.3. Mass Determination
It was measured all the specimen’s mass (n=45) with a precision scale, before and after the thermocycling. Specimens were divided in each material in “with clorhexidine”- meaning all the specimens with some concentration of clorhexidine and “without clorhexidine” wich included the control group.
3.4 Color Determination
Color was determinated using a Easyshade spectrophotometer ( Fig3.5) inside of a dark box (fig 3.6) and 3 evaluations were made at the bottom and the top of each specimen. The specimens were measured with a spectrophotometer, using the CIE L*a*b* system, at three specific times : before thermocycling aging ; after thermocycling aging and after the in vitro relase study
3.5 ANALITICAL METHODOLOGY
3.5.1 Standard stock and releasing solutions
To prepare a standard stock solution of 1000 ug/ml it was dissolved approximately 10mg of CHX into 10 ml of deionized water. This solution was kept out of light and at room temperature. On each new measurement of CHX, a series of dilutions of the stanrd stock solution were prepared ( 125; 62,5; 31,25; 15,62; 7,81; 3,905 μg/mL)
In this present study, the selected releasing solution was artificial saliva at pH=7 (Figure 3.7), to preview how the CHX would be released in the oral cavity. The
Figure 3.6 – Dark box Figure 3.5 – Vita Easyshade
Materials and Methods
artificial saliva was prepared according to a Faculty of Pharmacy University of Lisbon formula, courtesy of PhD student Joana Marto:
Boiling 50mL (F12-ED Refrigerated/Heating Circulator) of phosphate buffer pH=7.0 (Anhydride disodium phosphate, Monosodium phosphate anhudride and Deionized water) at 60ºC. Then sprinkled 0.05g of xanthan gum into boiling buffer and stirring until total of xanthan gum was dissolved.
Dissolving 0.04g of Calcium chloride dihydrat ( EW-N/EG-N balance) 0.08g of Sodium chloride and 0.08g of Potassium chloride in solution 1 and stirring until total of materials were dissolved.
Dissolving 15g of Propylene glycol in solution 2 and stirring until total of Propylene glycol was dissolved.
Pouring the solution 3 into graduated beaker and complete the solution with phosphate buffer pH=7.0 to 100mL
This solution was kept out of light, at room temperature. .
Materials and Methods
15 3.5.2 Analytical Technique
The absorbance of each solution was measured in a microplate reader ( FLUOstar Omega- BMG LABTECH) (Figure 3.8) and the absorbance values were obtained using an Ultraviolet-Visible absorbance Spectra detection mode, with a wavelength of 255nm, as recommended by other authors ( Anusavice et al. 2006). The measurements were performed at room temperature of 25ºC.
The CHX release concentrations were determined based on the linear calibration methodology, after subtracting the average of control’s absorbance at the corresponding time interval.
Figure 3.8 – Microplate reader
Materials and Methods
3.6 IN VITRO RELEASE STUDIES
A preliminary pilot study was conducted in order to optimize further experimental protocols.
With the aim to study the release of CHX from the specimens, the cylinders were stored individually in graduated falcon tubes of 5mL and covered with saliva pH=7, with a ration of 1g/5,mL (figure 3.9a) The Falcons were then placed into an incubator at 37ºC (Memmert), with constant gentle shaking ( 300rpm) (Figure 3.9b). At specific time intervals (1,4,24,48,72,144,168,192,216,240,336,504,672 hours)( Table 3.2), and after the falcons were agitatd in a mixer ( VELP Scientifica, Vortex), 450μLwere pipetted from each falcon to a polystyrene flat bottom microplate wells (96-well microplates) (150μL were pipetted to each (96-well). At the same time intervals, 450μL of artificial saliva at pH=7 were renovated in each falcon, in order to simulate the constant salivar renovation. The samples were analyzed as described above.
Figure 3.8 - Incubation of the speciens in graduated falcon tubes with saliva at ph=7
Figure 3.9 - Incubator at 37 ºC under constant gentle shaking
Materials and Methods
15 3.7. STATISTICAL ANALYSIS
Data were statistically analyzed using SPSS Statistics 20 (SPSS Inc., Chicago, IL, USA).
Descriptive statistics of mass, color variation and release data was carried out. Since data did not follow a normal distribution for the studied variables (verified by Kolmogorov-Smirnov normality tests), the results were submitted to the nonparametric tests according to the Kruskall Wallis method followed by multiple comparisons using Mann-Whitney tests with Bonferroni correction to determine whether there were specific significant differences among materials and groups.
In all statistical tests, it was considered the 5% level of significance (p<0.05)..
Materials and Methods
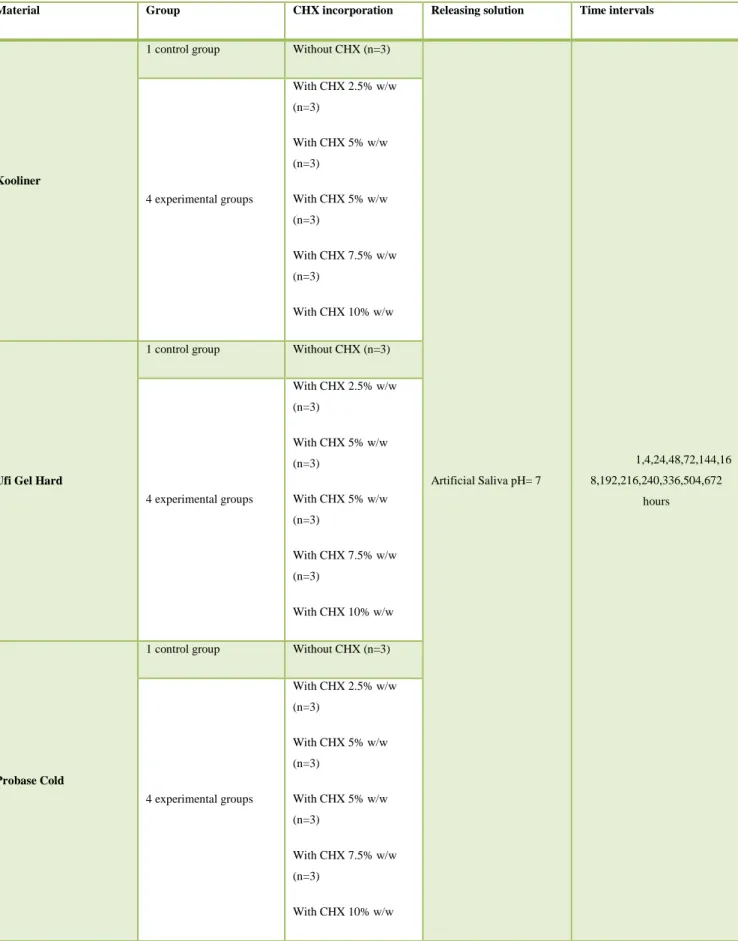
Table 3.2 – Schematization of distribution of the specimens
Material Group CHX incorporation Releasing solution Time intervals
Kooliner
1 control group Without CHX (n=3)
Artificial Saliva pH= 7 1,4,24,48,72,144,16 8,192,216,240,336,504,672 hours 4 experimental groups With CHX 2.5% w/w (n=3) With CHX 5% w/w (n=3) With CHX 5% w/w (n=3) With CHX 7.5% w/w (n=3) With CHX 10% w/w
Ufi Gel Hard
1 control group Without CHX (n=3)
4 experimental groups With CHX 2.5% w/w (n=3) With CHX 5% w/w (n=3) With CHX 5% w/w (n=3) With CHX 7.5% w/w (n=3) With CHX 10% w/w Probase Cold
1 control group Without CHX (n=3)
4 experimental groups With CHX 2.5% w/w (n=3) With CHX 5% w/w (n=3) With CHX 5% w/w (n=3) With CHX 7.5% w/w (n=3) With CHX 10% w/w
Results
15 4. RESULTS
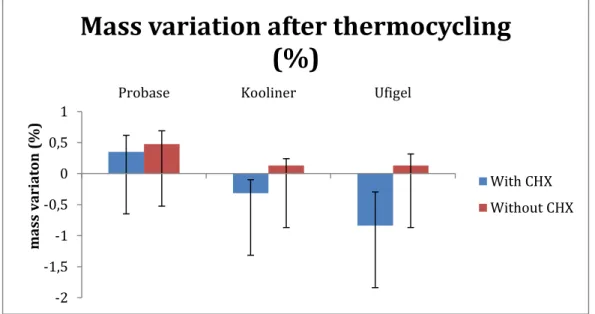
4.1 The effect of thermal aging in mass variation
Thermocycling caused mass variation in all the different materials (p<0.001).
Kooliner specimens with CHX had a mass decrease of 0,33557±0.2% compared to specimens without CHX (p=0.04). Ufi Gel Hard specimens with CHX had a mass decrease of 0,81435±0.4% when compared to specimens without CHX (p=0.018). Probase Cold had had no significant differences in mass variation (p= 0.365).
-2 -1,5 -1 -0,5 0 0,5 1
Probase Kooliner Ufigel
ma ss va ria ton (%)
Mass variation after thermocycling
(%)
With CHX Without CHX
Figure 4.1 Mass variation (%) between different materials and CHX loading
Results
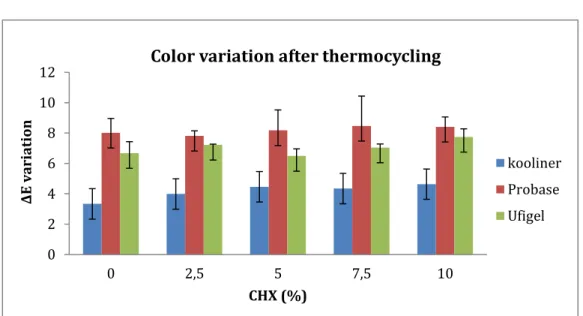
4.2 The effect of Thermal aging on color variation
Thermocycling caused color variation in all the different materials (p<0.001)
After thermocycling, specimens were considered having higher color variation in Probase (ΔE= 8,176424) than Ufi Gel (ΔE= 7,045814) and kooliner (ΔE= 4,34457) . Specimens of Ufi Gel Hard had higher values than Kooliner (p<0.001)
In each material, CHX incorporation didn’t lead to significant differences in ΔE (p=0.631) 0 2 4 6 8 10 12 0 2,5 5 7,5 10 Δ E va ria tio n CHX (%)
Color variation after thermocycling
kooliner Probase Ufigel
Figure 4.2 Color variation (ΔE) between different materials and CHX loading (2.5%, 5%, 7.5%,10%)
Results 15 y = 0,0122x - 0,0441 R² = 0,999 0 0,2 0,4 0,6 0,8 1 1,2 1,4 1,6 0 50 100 150 Abs 25 5 nm CHX concentration (μg/mL)
Saliva pH 7
Saliva pH 7 Linear (Saliva pH 7) 4.3. CHX release 4.3.1 CHX quantificationA linear relationship between CHX concentrations and the absorbance peak areas was established at 255 nm The analytical method showed good linearity (Figure 4.1).
Figure 4.3 – Linear relationship between CHX concentrations and the absorbance peak areas for artificial saliva at pH 7
Results
4.3.2. The effect of different materials on the drug release
Specimens of three different materials (Kooliner, Ufi Gel Hard and
Probase Cold) were evaluated in the present study, with CHX 2.5%, 5%, 7.5% and 10% (w/w), after thermocycling.
In K and U, the CHX quantified from all specimens was inferior to 0.6 μg/mL that was the minimum detectable capacity of the technique used in the present study. Considering Probase Cold specimens, it was observed a high rate of release until 336 h followed by a slower and steadier release until the end of the study (28 days) (Figure 4.2).
For CHX 2.5%, 14.493 μg/mL from Probase Cold were released until 48 hours of incubation. For CHX 5% , 22.832 μg/mL were released from Probase Cold were released until 48 hours . For CHX 7.5%, 35.895 μg/mL were released from Probase Cold were released until 48 hours. For CHX 10 %, 33.619 μg/mL were released from Probase Cold until 48 hours
All the comulative values were higherthan MIC described by Salim (Salim et al. 2013a) 0 10 20 30 40 50 60 70 80 90 0 200 400 600 800 Abs 25 5n m (u g/ml ) Time (h)
Probase Cold
Probase 2.5 % Probase 5% Probase 7.5% Probase 10% MICFigure 4.4 – Line diagram with the cumulative CHX concentration (μg/mL) versus time (hours) for Probase
Results
15 The maximum cumulative release (µg/mL) from Probase Cold during the study, is shown in Table 4.1. The results show that the maximum cumulative release is only 0.195%, meaning that only a small amount of initial loaded CHX is liberated from the specimens to the artificial saliva.
Table 4.1 Maximum cumulative release of chlorhexidine for Probase with CHX 2.5%, 5%, 7.5%, 10%.
Material Group (%) Maximum Cumulative Release
(µg/mL) t(h) % (w/w) 2.5 31,12803 336 0,032886 Probase Cold 5 62,98447 336 0,043487 7.5 75,05869 336 0,050299 10 78,74153 336 0,194504 19
Discussion
DISCUSSION
Several studies have investigated the use of polymers as drug delivery systems for slow release of antifungal drugs in order to treat oral infections (Li et al. 2009b; Salim, Satterthwaite, et al. 2012b).
Early Studies have mentioned that chlorhexidine is superior to other antifungal agents both on releasing and microbiological tests when compared to other antifungal drugs. (Amin et al. 2009; Redding et al. 2009; Salim, Moore, et al. 2012a; Salim, Moore, et al. 2013a; Salim, Silikas, et al. 2013b) However, there weren’t found many studies regarding the evaluation of physical changes over time of these acrylic resins with antimicrobial agents incorporated. (Goiato, 2009; Landayan,, 2014; S.-K. PARK, 2004) (Sousa 2014) () (2014)
The aim of the present study was to evaluate mass and color variation of three different reline acrylic resins with different drug loading after 1000 cycles of thermocycling between 5ºC and 55ºC. This method was selected because it is believed to simulate 6 weeks of thermal variation in the oral cavity (Gale and Darvell, 1999) caused by routine eating, drinking and breathing (Palmer et al., 1992). In addition it was tested the release capability of those resins after the aging process.
In terms of mass variation, it was hypothesized that thermocycling wouldn’t affect the mass of acrylic reline resins with incorporated chlorhexidine. However, the results have shown that there were statistically significant mass variations after thermocycling in the different materials. In Ufi Gel Hard and Kooliner the incorporation of drug caused differences in the mass variation. There was observed a mass gain in the control specimens and a mass decrease in the specimens with chlorhexidine.
In Probase Cold there was a general mass increase after thermocycling in all the specimens with no differences between the controls and the specimens with incorporated chlorhexidine. According to that, the null hypothesis was accepted. Probase mass gains during thermocycling might have been caused by water absorption from the specimens. In fact, studies have suggested that thermal fluctuations can cause surface stresses due to the high thermal gradients near the surface. Those mechanical stresses can directly induce crack propagation, porous
Discussion
15 formation and increase in solubility that will lead to water absorption (Bettencourt et
al. 2010, Goiato, et al. 2009a and 2009b,Landayan,et al. 2014, S.-K. PARK, 2004,
Sousa, 2014). On the other hand, it is believed that the mass loss observed in Ufi Gel Hard and Kooliner was caused by the release of chlorhexidine. However, if there was any water absorption from those resins it was not enough to compensate significantly the weight loss caused by the release of chlorhexidine. This makes sense if we consider that the molecular weight of chlorhexidine is much higher than water.
About color variation, it was hypothesized that thermocycling wouldn’t affect color stability in the acrylic resins with chlorhexidine incorporated. The results prove that there were differences in color variation after the thermocycling in all specimens. Also, it was observed that there were no differences between specimens with and without chlorhexidine. And this way, the null hypothesis was accepted.
Probase Cold was the material that had higher values of color variation followed by Ufi Gel Hard and Kooliner. This is in agreement with other studies that also found color variations in acrylic resins after thermocycling. However they didn’t test the effect of drug loading on that variation as we did in our study. The reason for color change might be related to intrinsic properties of each material, as well as dissolution of plasticizers and colorants. Also, the physical changes caused by thermocycling and water sorption could justify that color instability. In fact it is believed that water absorption and surface roughness affects color stability (Salloum, 2014) Color variation is also related to aging or damaging of the material (Goiato, 2009)
After thermocycling, the release study showed that in Kooliner and Ufi Gel specimens the chlorhexidine quantified from all specimens was inferior to 0.6 μg/ml (minimum detectable capacity of the technique used in the present study), Probase Cold was the only material that had release values superior than those.
Probase Cold had a high rate of initial release followed by a slower and steadier release that continued until the end of the study period. This agrees with earlier studies that explain that chlorhexidine release is controlled by a concentration dependent diffusion process (Amin et al. 2009, Anusavice et al. 2006; Bertolini et al. 2014; Gong et al. 2007; Hiraishi et al. 2008;; Li et al. 2009; Marcelino 2015; Ryalat
Discussion et al. 2011; Salim, Moore, et al. 2012a;,).It is believed that initially the drug that is on
the surface of the material is released rapidly. Afterwards it starts a second phase where there is a slow release of the medicine that is a result of a complex process involving the formation of fluid clusters around the drug molecules that will interact with the fluid absorption of the acrylic resins (Thaw 1982, Amin et al 2009)
The maximum cumulative release of the present study was 0,194% for PC. This signifies that a very small amount of the initial chlorhexidine incorporated was released to the artificial saliva. This percentage is lower than what was observed in other studies (Patel et al.2001; Salim, Moore, et al. 2012a) and the reason for that is probably because some part of the chlorhexidine might have been released during the thermocycling procedure which means that this process is not adequate to simulate aging in release studies.
In the present study, it was used artificial saliva at pH 7 to simulate oral cavity conditions because properties like viscosity can have an influence in the results. Most of the studies that were found used distilled water as media solution (Hiraishi et al. 2008; Salim, Moore, et al. 2012a; Bertolini et al. 2014). The total length of the study (28 days) was selected in order to compare with the existing investigations of the same length.
In contrast to the majority of the other studies that only measured the release of chlorhexidine in one concentration, in the present study four different chlorhexidine concentrations were evaluated in order to find the minimum concentration that is effective against C. albicans and at the same time preventing an allergic reaction by the host.
It is believed that chlorhexidine was released during thermocycling from Ufi Gel Hard and Kooliner because another study have tested the release capability of those materials with similar conditions and same chlorhexidine loading but without the effect of thermocycling and there was observed the release of much higher values of chlorhexidine (Neuza, 2015). The cause of drug release during the aging process may be related to the composition of the acrylic resins. Polyethylmethacrylate based materials like Ufi Gel Hard and Kooliner are known for their anomalous water uptake
Discussion
15 (Riggs et al. 2000; Patel et al. 2001; Salim, Moore, et al. 2012a; Salim, Satterthwaite,
et al. 2012b) that will cause a superior drug release compared to the materials with
methylmethacrylate like Probase ColdC (Patel et al. 2001). Compared to other drugs such as Fluconazole, chlorhexidine has higher solubility (Salim, Satterthwaite, et al 2012). Moreover, in Polymethylmethacrylate materials, after the droplet expansion it is observed the formation of cracks that will lead to a release of the drug (Addy and Thaw 1982; Riggs et al. 2000; Patel et al. 2001; Amin et al. 2009; Salim, Satterthwaite, et al. 2012b).
According to the findings of the present study, it is suggested to use Probase Cold chlorhexidine 2.5% because that percentage of chlorhexidine was enough to maintain minimum inhibitory drug releases for candida albicans (Salim 2013). for a long time and it will be less likely to cause allergic reactions to the host (Amin et al. 2009; Bertolini et al. 2014). In addition, Probase cold was the material whose release capability wasn’t affected seriously when exposed to the type of thermal variations that will be observed in the oral cavity. Even though it was the material whose color variation was the most perceived clinically, his therapeutic effect for long periods surpasses that disadvantage.
In respect of study limitations the size of the specimens used in this in vitro study is very different from the denture surface. In fact, drug release is related to surface area as smaller areas will expose less drug particles to the saliva (Salim, Moore, et al. 2012a), this can be compensated by the higher number of surfaces releasing chlorhexidine in the cylinders while in the denture would only release from one surface. The use of Thermocycling aging is not the best method to apply when a posterior release study is going to be performed because it causes drug releases that can’t be quantified during the aging process. The cylinder shape was not the best option to evaluate color variation as it only gives 2 good surfaces to read. A suggestion would be to make the specimens in a shape that allows more different readings but also that is more similar to the denture surface.
In future studies, it will be important to study the surface roughness of the specimens as well as other mechanical characteristics right after thermocycling and also after the release study. This way, it would be easier to find the causes of weight
Discussion
and color variation between materials and different drug loads. Also, it is important to associate microbiological and biocompatibility tests.
To sum up it is difficult to predict the duration and the physical properties of delivery systems based on acrylic reline resins when incorporated with chlorhexidine. Clinical studies should be performed in order to expose the materials to the complexity of the oral cavity and, this way, guide the implementation of this system in clinical practice.
Discussion
15 CONCLUSION
Within the limitations of this study, the main conclusions are:
Thermocycling induced significant changes in all the specimens in terms of weight, color stability and drug release capacity. Probase Cold was the only material that had appreciable release values after the aging process.
The incorporation of CHX into reline acrylic resins affects drug release and weight variation but it doesn’t affect significantly the color
variationafter thermocycling
To all the Probase Cold specimens with added CHX it was observed a fast initial release followed by a slower and steadier relase.
In Probase Cold, maximum CHX release was 0.6% meaning that only a small amount of initial loaded chlorhexidine was liberated.
All the drug loading specimens in Probase had cumulative concentrations superior than MIC values against C. albicans isolates.
References
7. REFERENCES
Addy, M. and Thaw, M., 1982. In vitro studies into the release of chlorhexidine acetate, prednisolone sodium phosphate, and prednisolone alcohol from cold cure denture base acrylic. Journal of Biomedical Materials Research Part B: Applied
Biomaterials, 16(2), pp.145–157.
Amin, W.M. et al., 2009. A new form of intraoral delivery of antifungal drugs for the treatment of denture-induced oral candidosis. European journal of dentistry, 3(4), pp.257–266.
Anusavice, K.J., Zhang, N.-Z. and Shen, C., 2006. Controlled release of chlorhexidine from UDMA-TEGDMA resin. Journal of Dental Research, 85(10), pp.950–954.
Arima, T., Murata, H. and Hamada, T., 1995. Properties of highly cross-linked
autopolymerizing reline acrylic resins. The Journal of prosthetic dentistry, 73(1), pp.55–59.
Bertolini, M.M. et al., 2014. Resins-based denture soft lining materials modified by chlorhexidine salt incorporation: An in vitro analysis of antifungal activity, drug release and hardness. Dental Materials, 30(8), pp.793–798.
Bettencourt, A 2010. Biodegradation of acrylic based resins : A review. Dental materials, e171-e180.
Cao, Z. et al., 2010. Rechargeable Infection-responsive Antifungal Denture Materials.
Journal of Dental Research, 89(12), pp.1517–1521.
Chandra, J. et al., 2001. Antifungal Resistance of Candidal Biofilms Formed on Denture Acrylic in vitro. Journal of Dental Research, 80(3), pp.903–908.
da Silva, P.M.B. et al., 2011. Microscopical analysis of Candida albicans biofilms on heat-polymerised acrylic resin after chlorhexidine gluconate and sodium hypochlorite treatments. Mycoses, 54(6), pp.e712–e717.
References
15 El-Hadary, A., & Drummond, J. L. (2000). Comparative study of water sorption, solubility, and tensile bond strength of. THE JOURNAL OF PROSTHETIC
DENTISTRY.
Figueiral, F. P.-L.-M. (2015). Effect of Denture-Related Stomatitis Fluconazole Treatment on Oral Candida albicans Susceptibility Profile and Genotypic Variability.
Open Dent J, 46-51.
Gong, K. et al., 2007. Controlled release of chlorhexidine diacetate from a porous methacrylate system: Supercritical fluid assisted foaming and impregnation. Journal
of Pharmaceutical Sciences, 96(8), pp.2048–2056
Hiraishi, N. et al., 2008. Chlorhexidine release and water sorption characteristics of chlorhexidine-incorporated hydrophobic/hydrophilic resins. Dental Materials, 24(10), pp.1391–1399.
Hatim, N. A., & Al-Tahho, O. Z. ( 2013). Comparative Evaluation of Color Change Between Two Types of Acrylic Resin and Flexible Resin After Thermo Cycling. An In Vitro Study. The Journal of Indian Prosthodontic Society, 327-337.
Hatim, N. A., & Al-Tahho, O. Z. (2013). Comparative Evaluation of Color Change Between Two Types of Acrylic Resin and Flexible Resin After Thermo Cycling. An In Vitro Study. The Journal of Indian Prosthodontic Society, 327-337.
Jordi Izzard Andaya Landayan, e. a. (2014). Effect of aging on tear strength and cytotoxicity of soft denture lining materials; in vitro. Adv Prosthodont.
Li, J. et al., 2009. In vitro drug release study of methacrylate polymer blend system: effect of polymer blend composition, drug loading and solubilizing surfactants on drug release. Journal of Materials Science: Materials in Medicine, 21(2), pp.583–588.
Lyu X, Z. C. (2016). Efficacy of nystatin for the treatment of oral candidiasis: a systematic review and meta-analysis. Drug Des Devel Ther.
Marcelino, N. Effect of Chlorhexidine Incorporation on Acrylic Reline Resins- Release Studies. Dissertação (Mestrado integrado em Medicina Dentária) Faculdade de Medicina Dentária da universidade de Lisboa; 2015
References
Marcelo Coelho Goiato, B. C. (2009). EFFECTS OF THERMOCYCLING ON MECHANICAL PROPERTIES OF SOFT LINING MATERIALS. Acta Odontol.
Latinoam, 227-232.
Marcelo Coelho Goiato, R. M.-A. (2009). EVALUATION OF HARDNESS AND COLOR STABILITY IN THE SOFT LINING MATERIALS AFTER THERMOCYCLING AND CHEMICAL POLISHING. Acta Odontol. Latinoam., 63-68.
Patel, M.P. et al., 2001. A polymeric system for the intra-oral delivery of an anti-fungal agent. Biomaterials, 22(17), pp.2319–2324. Rautemaa, R. and Ramage, G., 2011. Oral candidosis – Clinical challenges of a biofilm disease. Critical Reviews in
Microbiology, 37(4), pp.328–336.
Redding, S. et al., 2009. Inhibition of Candida albicans biofilm formation on denture material. YMOE, 107(5), pp.669–672.
Paulo Maurı´cio Batista da Silva, 1. J. (2011). Microscopical analysis of Candida albicans biofilms on heat-polymerised acrylic resin after chlorhexidine gluconate and sodium hypochlorite treatments. Mycoses, 54-58.
Pereira-Cenci T, D. B. (2008). Development of Candida-associated denture stomatitis: new insights. J Appl Oral Sci, 86-94.
Peter A. Suci, B. J. (2002). Action of Chlorhexidine Digluconate against Yeast and Filamentous Forms in an Early-Stage Candida albicans Biofilm. Antimicrob Agents
Chemother, 3522–3531.
Polyzois GL1, Y. S. ( 1999). Color stability of visible light-cured, hard direct denture reliners: an in vitro investigation. Int J Prosthodont, 140-6.
Riggs, P.D. et al., 1999. The water uptake of poly(tetrahydrofurfuryl methacrylate).
Biomaterials, 20(5), pp.435–441.
Riggs, P.D., Braden, M. and Patel, M., 2000. Chlorhexidine release from room temperature polymerising methacrylate systems. Biomaterials, 21(4), pp.345–351.
References
15 Ronanki S, K. S. (2016). Efficacy of commercially available chlorhexidine mouthrinses against specific oral microflora. Indian J Dent Res, 48-53.Ryalat, S., Darwish, R. and Amin, 2011. New form of administering chlorhexidine for treatment of denture-induced stomatitis. Therapeutics and Clinical Risk Management p.219 Salim, N., Moore, C., et al., 2012a. Fungicidal amounts of antifungals are released from impregnated denture lining material for up to 28 days. Journal of Dentistry, 40(6), pp.506–512.
Salim, N., Moore, C., et al., 2013a. Chlorhexidine is a highly effective topical broadspectrum agent against Candida spp. International journal of antimicrobial
agents, 41(1), pp.65–69.
Salim, N., Satterthwaite, J.D., et al., 2012b. Impregnation with antimicrobials challenge bonding properties and water sorption behaviour of an acrylic liner. Journal
of Dentistry, 40(8), pp.693–699.
Salim, N., Silikas, N., et al., 2013b. Chlorhexidine-impregnated PEM/THFM polymer exhibits superior activity to fluconazole-impregnated polymer against Candida albicans biofilm formation. International journal of antimicrobial agents, 41(2), pp.193–196.
Salloum, A. M. (2014). Effect of 5.25 % Sodium Hypochlorite on Color Stability of Acrylic and Silicone Based Soft Liners and a Denture Base Acrylic Resin. J Indian
Prosthodont Soc, 179–186.
S.-K. PARK, Y.-K. L.-S.-W. (2004). Changes in properties of short-term-use soft liners after thermocycling. Journal of Oral Rehabilitation, 717–724
Wala M. Amin, a. M.-A.-T. ( 2009). A New Form of Intraoral Delivery of Antifungal
Appendices
APPENDICES
Appendice 1- List of Tables
Table 3.1 Materials used in the study
Table 3.2 Schematization of distribution of the specimens
Table 4.1 Maximum cumulative release of chlorhexidine for Probase with CHX 2.5%, 5%, 7.5%, 10%.
Appendices
15 APPENDIX 2 – LIST OF FIGURES
Figure 3.1 Materials used in the study: a) Kooliner; b) Ufi Gel Hard c) Probase Cold Figure 3.2 Preparation of the specimens: a) Package o the Chlorhexidine diacetate monohydrate; b) incorporation and homogenization of the CHX; c) Cylinder-shaped specimen; d) Cylinder-shaped mold
Figure 3.3 Ivomat pressure device Figure 3.4 themocycling equipment Figure 3.5 Vita easyshade
Figure 3.6 Dark Box
Figure 3.7 Artificial Saliva at pH 7 Figure 3.8 Microplate reader
Figure 3.9 Incubation of specimens in graduated falcon tubes with saliva at pH=7 Figure 3.10 Incubator at 37ºC under constant gentle shaking
Figure 4.1 Mass variation (%) between different materials and CHX loading
Figure 4.2 Color variation (ΔE) between different materials and CHX loading ( 2.5%; 5%; 7.5%, 10%)
Figure 4.3 Linear relationship between CHX concentrations and the absorbance peak areas for artificial saliva at pH7
Appendices
APPENDIX 3 – LIST OF ABBREVIATIONS
1.6- HDMA 1.6-hexanedioldimethacrylate C.albicans Candida albicans
CHX chlorhexidine h Hours IBMA Isobutylmethacrylate K Kooliner L Liquid M Mean m Mass
MIC Minimum inhibitory concentration
MMA Methylmethacrylate
P Powder
PEMA Polyethylmethacrylate
PMMA Polymethylmethacrylate
Appendices
15 APPENDIX 4 – EXPERIMENTAL DATA
Mass variation (%) CHX % (w/w) Material 0 2,5 5 7,5 10 Probase Cold M 0,477627 0,128733 0,304105 0,401405 0,441826 SD 0,313694 0,741256 0,951704 0,391605 0,180004 Ufi Gel Hard M 0,132661 -0,22727 -3,84421 -1,2987 -0,37244 SD 0,183151 0,553177 0,603677 0,266592 0,527019 Kooliner M 0,131199 -0,52274 -0,73973 -0,10596 -0,07853 SD 0,109487 0,152848 0,228223 0,599137 0,205076 Color Variation CHX % (w/w) Material 0 2,5 5 7,5 10 Probase Cold M 8,018767 7,816454 8,176424 8,469745 8,408993 SD 0,946694 0,329665 1,344761 1,965721 0,646104 Ufi Gel Hard M 6,677866 7,223732 6,49068 7,045814 7,74022 SD 0,754326 0,045325 0,467175 0,228654 0,530888 Kooliner M 3,336215 3,986597 4,458546 4,34457 4,633626 SD 0,688525 0,041243 1,349876 1,12548 0,420405 33
Appendices Release study Probase Cold 2.5% Time intervals (hours) M(comulative concentration) SD(Comulative concentration) M(CHX %released) SD( CHX %released) 0 0 0 0 0 1 0 0 0 0 4 0 0 0 0 24 12.49268 0.054843 0.042366 0.069816 48 14.49262 0.153142 0.023565 0.051681 72 15.70131 0.061365 0.035062 0.092262 144 16.82454 0.035528 0.026846 0.065218 168 24.68697 0.05847 0.0.39549 0.081469 192 29.23516 0.077853 0.021652 0.049258 216 30.4468 0.063644 0.0216199 0.051816 336 30.9254 0.072923 0.0261881 0.0218969 504 31.12803 0.087821 0.05656 0.091285 672 33.55959 0.065986 0.050278 0.851836
Appendices 15 Probase Cold 5% Time intervals (hours) M(comulative concentration) SD(Comulative concentration) M(CHX %released) SD( CHX %released) 0 0 0 0.044883 0.0596816 1 17.49262 0.08414 0.083044 0.0715481 4 18.58101 0.106275 0.124145 0.056262 24 29.51054 0.093798 0.143609 0.037218 48 35.6946 0.1014 0.155751 0.025869 72 40.01578 0.145438 0.164431 0.057938 144 45.3652 0.060514 0.174309 0.067816 168 47.66471 0.069383 0.194504 0.8458969 192 53.21193 0.098097 0.189813 0.063785 216 58.94509 0.086797 0.186083 0.051836 336 60.06124 0.08789 0.044883 0.031451 504 62.98447 0.096146 0.083045 0.0184851 672 65.37444 0.08896 0.124145 0.0486151 35
Appendices Probase Cold 7.5% Time intervals (hours) M(comulative concentration) SD(Comulative concentration) M(CHX %released) SD (CHX % released) 0 0 0 0 0 1 18.65991 0.158173 0.176516198 0.0545481 4 20.35455 0.044721 0.186884641 0.065262 24 22.83224 0.076164 0.296812024 0.038418 48 28.15926 0.07535 0.402472028 0.0632869 72 38.90505 0.182313 0.479403675 0.087838 144 44.70762 0.100316 0.535196725 0.0987816 168 54.76601 0.042287 0.592859873 0.789695 192 61.43249 0.117726 0.601186155 0.0987785 216 65.70508 0.061996 0.621861814 0.098366 336 75.05869 0.087097 0.633487251 0.0978451 504 75.1279 0.038772 0.657525129 0.0975884 672 85.02716 0.092054 0.673529431 0.04526151
Appendices 15 Probase Cold 10% Time intervals (hours) M(comulative concentration) SD(Comulative concentration) M(CHX %released) SD( CHX %released) 0 0 0 0 0 1 5.524365007 0.067015 0.186884641 0.071481 4 14.14065826 0.052922 0.296812024 0.046262 24 18.16993777 0.065864 0.402472028 0.012218 48 33.61890654 0.024396 0.479403675 0.035869 72 50.25785615 0.103822 0.535196725 0.034238 144 54.25675626 0.016851 0.592859873 0.055216 168 58.13757875 0.034493 0.6113151316 0.2358969 192 63.05333277 0.053648 0.625565186 0.0342785 216 66.56722166 0.010837 0.633487251 0.065836 336 70.56621225 0.052151 0.657525129 0.052451 504 78.74153101 0.020474 0.673529431 0.05254851 672 76.84272257 0.073326 0.276516198 0.0656151 37