w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Reactions
related
to
asparaginase
infusion
in
a
10-year
retrospective
cohort
Amanda
Cabral
dos
Santos
∗,
Marcelo
Gerardin
Poirot
Land,
Nathalia
Peroni
da
Silva,
Kelly
Oliveira
Santos,
Elisangela
da
Costa
Lima-Dellamora
UniversidadeFederaldoRiodeJaneiro(UFRJ),RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20February2017 Accepted3August2017
Availableonline12September2017
Keywords:
Leukemia
Acutelymphoblastic Asparaginase Adversedrugreaction Intravenousinfusions
a
b
s
t
r
a
c
t
Introduction:Althoughitis anessentialcomponentofthetreatment ofacutelymphoid leukemiainchildren,asparaginasecausesadversereactionsthatsometimesmakeit impos-sibletouseitfully.Hypersensitivityreactionsarethemostfrequentandmayleadtoearly discontinuationoftreatment.Thepresentstudyaimedtoinvestigatesuspicionsofadverse reactionsduringtheinfusionofasparaginaseinapediatriccohort.
Methods:Aretrospectiveobservationalstudywascarriedoutatauniversitypediatric insti-tuteinthestateofRiodeJaneiro.Informationregardingclinicalfeaturesandcharacteristics ofadversereactionswascollectedfromhospitalmedicalrecords.Suspicionsofadverse reactionswereclassifiedregardingcausalityandseverity.
Results:Seventy-threesuspicionsofadversereactionswererecordedduringasparaginase infusionin72childreninthestudyperiod.Allergichypersensitivityreactionswere sus-pectedin60.5%ofthecases.Ofthese,25%ofthereactionsoccurredduringinductionand 61.1%inconcomitantusewithvincristine,findingsthatdivergefromotherstudies. High-riskclassificationandyoungeragewereconsideredriskfactorsforthesereactions.Atotal of72.4%ofthereactionswereclassifiedasgrade1or2,whichsuggestthatnotallarerelated toantibodyformation;thishighlightstheimportanceofdifferentialdiagnosiswithother reactions,suchasnon-allergichypersensitivityandhyperammonemia.
Conclusion: Theimplementationofthedifferentialdiagnosisofreactionsrelatedtoinfusion ofasparaginasewithammoniadosageandclassificationofthegradeofreactionsiscrucial tofacilitatetheidentificationandpropermanagementofeachtypeofreaction.
©2017PublishedbyElsevierEditoraLtda.onbehalfofAssociac¸ ˜aoBrasileirade Hematologia,HemoterapiaeTerapiaCelular.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthorat: FaculdadedeFarmácia daUniversidadeFederaldoRio deJaneiro(UFRJ),RuaBrunoLobo,n◦50,Cidade
Universitária,21941-912RiodeJaneiro,RJ,Brazil.
E-mailaddress:[email protected](A.C.Santos). https://doi.org/10.1016/j.bjhh.2017.08.002
Introduction
Canceristhemaincauseofdeathduetoillnessintheage groupof0–19yearsinBrazil.Inrecentyearstherehasbeen a progressive and linear increase in the number of pedi-atriccases,especiallyofacutelymphoblasticleukemia(ALL),1 whichisthemostcommontypeinchildhood.Treatmentof ALLincludesthe useofthe bacterialenzymeasparaginase becauseofitsabilitytohydrolyzetheaminoacidl-asparagine inasparticacidandammonia,thusaffectingleukemicblasts, whicharegenerallyincapableofproducingasparaginebytheir ownmetabolism,unlikenormalcells,whichhaveasparagine synthetase. Asparagine depletion causes disruption of the functioningofblastsandconsequentlycelldeath.2
Asparaginase was incorporated into the treatment of ALL in the 1970s as an essential component of induction regimens andconsolidationofremission inpediatricALL.3 Threeenzymepreparationsareused:(i)nativel-asparaginase derivedfromEscherichiacoli(EcA)or(ii)inthepegylatedform (EcPA)and(iii)isolatedl-asparaginasefromErwinia
chrysan-themi(ErA).4Themainlimitationofitsuseistheoccurrence ofadversereactionsthat canprovokeharmful,unintended responses,evenwithadequatedoses.Someofthesereactions, suchashypersensitivityreactionsandhyperammonemia,can occurduringasparaginaseinfusion.5
EcAcanbeadministeredintravenously(IV)or intramuscu-larly(IM).TheIVrouteallowsinterruptionoftheinfusionin caseofanaphylacticreactions.Thispathwayistheleast sensi-tizingamongtheparenteralroutes,althoughwithahigherrisk ofseriousanaphylacticreactions.6Inaddition,IM administra-tioncausespain,mayrequiremultipleinjectionsforhigh-dose administrationandexposesthepatienttothefulldose,even withseverereactions.Recentstudieshaveshowncomparable incidenceofhypersensitivityreactionsinbothroutes.5
Hypersensitivity reactions are considered unpredictable and not related to dose.7,8 Among these, those that are
Table1–Clinicalcharacteristicsofpatientsand suspectedadversereaction(n=119).
Clinicalcharacteristic n(%)
Sex
Male 67(56.3)
Female 52(43.7)
TypeofALL
BCP-LLA 101(84.9)
T-LLA 18(15.1)
Riskclassification
Standard 27(22.7)
Medium 43(36.1)
High 49(41.2)
SRAduringtheasparaginaseinfusion
Yes 72(60.5)
No 47(39.5)
BCP-LLA: acute lymphoblastic leukemia of B-cell precursors; T-ALL:acuteT-celllymphoblasticleukemia;SRA:suspectedadverse reaction.
triggeredbyanimmunological mechanismandwhich may causeanaphylaxisareconsideredallergic.6,9
Allergic hypersensitivity reactions impairthe continuity oftreatmentwiththetypeofl-asparaginaseadopted,since inactivationoftheenzymemayoccurduetotheformation ofanti-asparaginaseimmunoglobulinIgGandIgEantibodies, makingitsuseriskyandineffective.10,11
Somefactorsarerelatedtoagreaterchanceofdeveloping hypersensitivity reactionssuchastheprotocolphase (post-inductionphases),routeofadministration,doseinterval,type ofl-asparaginaseandconcomitantuseofdrugs.2,4,10,12,13
Early discontinuation of treatment with the enzyme is common,14especiallyincountriessuchasBrazil,whereonly the conventional EcA has been registered in the national healthsurveillanceagency.Suchaninterruptionmayleadto inferiorresultswhencomparedtopatientswhocanuseall theprescribeddoses.4
Thepresentstudyaimedattheanalysisofreactionsrelated toEcAinfusionsinacohortofchildrenwithALLtreatedover aperiodoftenyears.
Methods
Alongitudinalstudywasconductedwithretrospectivedata collectedonALLtreatment(inthephasesofinduction, consol-idationandremissionre-induction)inapediatricuniversity hospitallocatedinthestateofRiodeJaneiro.
Patientsofupto12years ofage,diagnosedwithALLin the period between January 2005 and December 2014 and treatedwithEcAaccordingtotheGermanprotocol ALL-BFM-IC,11,15wereidentifiedthroughthehigh-complexitytreatment authorization lists,which allowtheidentification of proce-dures, such as chemotherapy, according to the individual and disease. This was supplemented by the hospital data records system.16 Infantstreated withtheINTERFANT pro-tocol, patientson relapse treatment,aswell astransferred patientswhostartedorterminatedtreatmentatanother insti-tutionwereexcludedfromthestudy.
Datawerecollectedfromspeciallydesignedtreatment pro-tocolsusedtoregisterdetailedinformationaboutthedisease stage,thechemotherapyactuallyappliedandcomplications, andtheoutcomes.Thecompletemedicalrecordswere con-sulted when informationwas missingabout the signs and symptomsofthereactionsintheserecords.
Thedatarelatedtothecharacterizationofthepatient(age at diagnosis and sex), leukemia (type ofALL, risk classifi-cation),treatment(treatmentphase,prescribedmedication, posology, routeofadministration)and descriptionof suspi-cions of adverse reactions to EcA13,17 were collected on a specificformdesignedforthisstudyandlaterorganizedon spreadsheetsoftheMicrosoftExcel®program.
asdubious,possible,probableanddefined.20Severityanalysis consideredthedescriptionofsignsandsymptomstakinginto accountthecommonterminologycriteriaforadverseevents (CTCAEv3.0)21forallergicreactions/hypersensitivity.
Theexploratoryanalysisofthedataconsistedinthe calcu-lationofmeasuresofcentraltendencies(meanandmedian), dispersion(standarddeviation)andproportions.
Theanalysisofadversereactionsrelatedtotheinfusion demandedareviewofevidenceontheeffectivenessandsafety ofEcA.Themechanismsrelatedtoallergicandnon-allergic hypersensitivityinfaceoftheoccurrenceof hyperammone-mia, as well as aspects related to drug interaction with vincristinehighlightedinthetherapeuticschemeusedinthe studiedinstitutionwereparticularlyimportantforthe formu-lationofhypothesesrelatedtocausalityandtypeofreaction presentedduringtheintravenousinfusionofEcA.
Thebinomiallogisticregressionmodelwasusedto calcu-latetheunivariateoddsratioofeachvariable selectedasa possibleriskfactorforthedevelopmentofhypersensitivity reactionsfromitsbiologicalplausibilityinisolation.For mul-tivariateanalysis,variableswithp-values<0.20intheprevious stageandaftercollinearityanalysiswereconsideredpotential predictivevariablestobeincludedinthemodeling.The step-wisemethodwithbackwardeliminationwasusedtoselectthe parsimoniouspredictivemodel,usingthelikelihoodratiofor itsselection.AlltheseanalyzeswereperformedintheSPSS® program.
Theresearchprojectwassubmittedto,registeredinand approvedbytheResearchEthicsCommitteeoftheInstitution (#1.218.087).
Results
Case-by-case
Onehundredandtwenty-fivepatientswithALLweretreated duringthestudyperiod.Ofthese,sixcasesfulfilledthe exclu-sioncriteria.Themeanandmedianagesoftheinvestigated groupwere 5.1(±2.97)and four years,respectively.Table 1 showsthecharacterizationofthepatients.
All reactions related toEcA infusionwere described as allergicinthe medicalrecords.Allpatients who presented reactionshadtheirtreatmentinterrupted.Inonlyonecase thereactionoccurred twice,withdifferentsignsand symp-toms;treatmentwasdiscontinuedafterthesecondreaction, thus73reactionsarereportedin72individuals.
Table2showstheexploratoryanalysisofthe characteris-ticsrelatedtothetreatmentatthetimeoftheappearanceof thereactionthatarepointedoutintheliteratureasriskfactors forallergichypersensitivity.Differenttypesofasparaginase andadministrationroutescouldnotbeanalyzedbecausethis isanobservationalstudyinwhichonlyEcAwasused,and alwaysbyanIVroute.
Analysis
AfterapplyingtheNaranjo’salgorithmforcausalityanalysis, 34suspectedadversereactionswereclassifiedaspossibleand 39asprobable.
Table2–Descriptiveanalysisofcharacteristicsrelatedto thetreatmentatthetimeofreaction(n=73).
Characteristic n(%)
Treatmentphase
Induction 18(25)
Post-induction 54(75)
Increasedintervalbetweendosesforpreviousreactions
Yesa 37(51)
No 36(49)
Concomitantuseofvincristine
Yes 44(61.1)
No 28(38.9)
Concomitantuseofcorticosteroids
Yes 31(43)
No 41(57)
a 37 individuals had reactions other than hypersensitivity on
oneormoreoccasionsbeforethehypersensitivity:36suffered hypofibrinogenemiaandonehepaticalterationthatledtothe postponementofdoses.
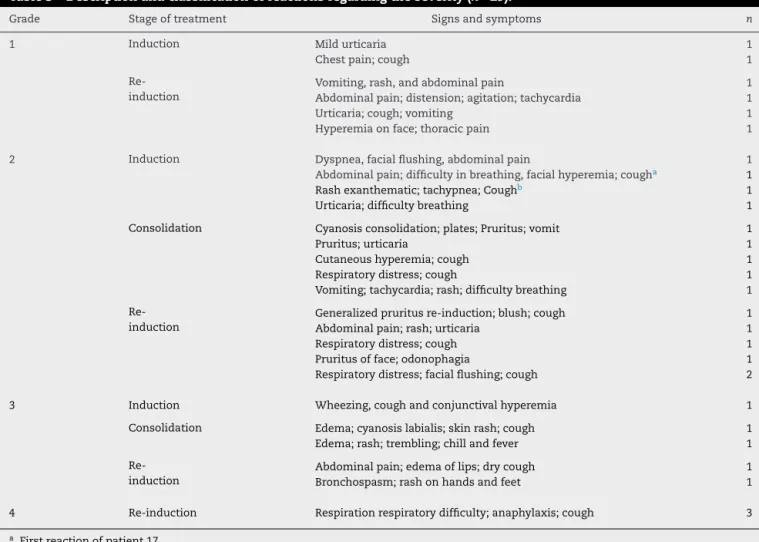
Only29cases(40%)couldbeclassifiedaccordingtoseverity (Table3).Theothersuspicionsofhypersensitivity reactions had no description ofsigns and symptoms inthe medical recordsandweredenominatedonlyas‘allergy’.
Among the suspicionsof hypersensitivity that could be classified,therewasapredominanceofgrade1and2 reac-tions(72.4%).Itwasobserved,however,thatsomesignsand symptomsdescribedincasesoflessseverity,suchas respira-torydistress,vomiting,rashandagitation,12arealsocommon toincreasesinserumammonialevelaftertheadministration ofasparaginaseand13patientshadsuchsymptoms.
Riskfactors forthe development ofreactions relatedto asparaginase infusion were analyzed and it was identified that gender, type ofALL and previous hypofibrinogenemia were notstatisticallysignificant.Riskandageclassification werestatisticallysignificant(Tables4and5)andnon-collinear. Inamultivariateanalysis,thehigh-riskclassificationwasa riskfactorforthedevelopmentofthesereactions(oddsratio: 2.801)withageprovingtobeaprotectivefactor(0.883foreach yearoflife).
Discussion
ThedistributionofsexandoftypeofALLofthispopulation weresimilartootherstudies,withadiscretepredominanceof casesinboysandwithapproximately85%ofALLbeingcases ofB-cellprecursors.4,12,13Themajority(41.2%)werehigh-risk patients.Thisprofilediffersconsiderablyfromthatobserved intheGermanstudythatwasthebasisoftheALL-BFM-IC2002 protocol,inwhichonly17%werehigh-riskcasesandtherewas ahighernumberofintermediate-riskpatients(52.4%).13
Anotherrelevantaspectwastheoccurrenceofreactions (25% of the cases) in the induction phase. Allergic hyper-sensitivityreactionsare predominantinthepost-induction phases.10 Woo et al. reported an incidenceof only12% of hypersensitivityreactionsintheinductionphase.22
Table3–Descriptionandclassificationofreactionsregardingtheseverity(n=29).
Grade Stageoftreatment Signsandsymptoms n
1 Induction Mildurticaria 1
Chestpain;cough 1
Re-induction
Vomiting,rash,andabdominalpain 1
Abdominalpain;distension;agitation;tachycardia 1
Urticaria;cough;vomiting 1
Hyperemiaonface;thoracicpain 1
2 Induction Dyspnea,facialflushing,abdominalpain 1
Abdominalpain;difficultyinbreathing,facialhyperemia;cougha 1
Rashexanthematic;tachypnea;Coughb 1
Urticaria;difficultybreathing 1
Consolidation Cyanosisconsolidation;plates;Pruritus;vomit 1
Pruritus;urticaria 1
Cutaneoushyperemia;cough 1
Respiratorydistress;cough 1
Vomiting;tachycardia;rash;difficultybreathing 1
Re-induction
Generalizedpruritusre-induction;blush;cough 1
Abdominalpain;rash;urticaria 1
Respiratorydistress;cough 1
Pruritusofface;odonophagia 1
Respiratorydistress;facialflushing;cough 2
3 Induction Wheezing,coughandconjunctivalhyperemia 1
Consolidation Edema;cyanosislabialis;skinrash;cough 1
Edema;rash;trembling;chillandfever 1
Re-induction
Abdominalpain;edemaoflips;drycough 1
Bronchospasm;rashonhandsandfeet 1
4 Re-induction Respirationrespiratorydifficulty;anaphylaxis;cough 3
a Firstreactionofpatient17.
b Secondreactionofpatient17.
Table4–Riskfactorsforreactionsrelatedto asparaginaseinfusion.
Reactionduringasparaginaseinfusion
Riskfactor YesNoOddratio95%confidenceintervalp-value
Sex
Female 33 19 1.247 0.592–2.625 0.577
Male 39 28
TypeofALL
BCP-ALL 63 38 1.658 0.605–4.542 0.433
T-ALL 9 9
Previoushypofibrinogenemia
Yes 36 29 0.621 0.294–1.311 0.254
No 36 18
Riskclassification
Highrisk 36 13 2.615 1.189–2.755 0.021
Nothighrisk36 34
Age 0.873a 0.767–0.995 0.041
SC 0.351b 0.080–1.547 0.167
BCP-LLA:acutelymphoblasticleukemiaofB-cellprecursors;T-ALL: acuteT-celllymphoblasticleukemia.
a Foreachyearoflife.
b Foreachsquaremeter.
Table5–Multivariateanalysis(binomiallogistic regression).
Variable B Oddsratio Exp(B)
95% confidence intervalfor oddsratio
p-value
Lower Upper
Highrisk 0.980 2.665 1.180 6.019 0.018
Age −0.151 0.860 0.750 0.986 0.031
Constant 0.939 2.557 0.037
averageof30%forpatientsusingasparaginasederivedfrom E.coli7,10),thepercentageobservedinthepresentstudy(60.5%) was high,aconditionaggravatedbythe lackofalternative typesofasparaginasetocontinuetreatmentinBrazil.
ofALL,since,ofthethreetypes,itwasconsideredthemost immunogenic.14,23
Concomitantuseofcorticosteroidsandvincristineis con-sidered a protective factor for hypersensitivity reactions.10 However,therewasahigherincidenceofreactionsinpatients whoreceivedvincristinetogether withasparaginase,which may be related to the routine of shortening the interval betweentheadministrationsofthesedrugsatthestudysite. Administrationof vincristineand asparaginase withinless than12hincreasestheriskofneurotoxicityandreactionsto vincristine.Asparaginaseisahepatotoxicdrugandvincristine undergoes hepatic metabolism.24 The possible increase in reactionstovincristinemaybeaconfounderinthediagnosis ofreactionstoasparaginase.
Discontinuationoftreatmentonsuspicionofa hypersen-sitivityreactiontoasparaginasemayhavebeenunnecessary. Theanalysisofthedescriptionsofthesuspectedadverse reac-tionssuggeststhat,insomeofthecases,hyperammonemia reactionsmayhaveoccurred,whosemanagementispossible. Theincreaseinserumammonialevelsaftertheintravenous administrationofasparaginaseoccursinchildrenat concen-trationsof260–700mol/L17(referencevalueupto30mol/L). Hyperammonemia can cause nausea, vomiting, headache, restlessness,dizzinessandrash,8,25 whichwereobservedin 13casesofthisstudy.
Grade3 (bronchospasm and/or angioedema) and Grade 4 (anaphylaxis) hypersensitivity reactions are easily diag-nosed.Van derSluis et al.recommend the replacementof asparaginasewhenseverereactionsare observed.However, itseemspossibletohavereactionsclassifiedasGrade2,with manifestationssimilartoallergies,withouttheformationof antibodies,as demonstrated by Kloss et al.25 According to these authors,the reactions related to antibodyformation occur,ingeneral,atthebeginningoftheinfusion.
Theidentificationthat highriskandlowageofpatients aremorelikelytodevelopinfusion-relatedreactionsalso indi-catestheneedforadifferentialdiagnosisofthesereactions, sinceearlytreatmentdiscontinuationfurtherincreasesriskin thesetwogroups.
Itis known thathigh-risk patients are exposed tohigh doses of asparaginase (25,000IU/m2) in the consolidation
phaseofremission,whichdoesnotoccurintreatmentsof chil-drenwithotherriskclassifications.15Inaddition,Liuetal.26 demonstrated intheir work that hypersensitivity reactions aremorecommoninlessintensiveregimenssuchasthose appliedtonon-high-riskpatientsinthepresentstudy.This findingdiffersfromthepresentstudy.Animportantdifference betweenthetwostudiesisthatadministrationwasIVinthe currentstudywhereasanIMadministrationwasusedinthe other;thisreinforcesthepossibilityofhyperammonemiaand non-allergichypersensitivityreactionsamongthose consid-eredallergichypersensitivity,asammonialevelsriserapidly duringasparaginaseinfusionbyIVadministrationandthere isthepossibilityofanaphylactoidreactionsrelatedtotheIV route.12,24
Concerning age, children undergo intense physiological changesinthefirstyearsoflifethatculminatein differenti-atedpharmacokineticsinthedifferentstagesofchildhood,27 this fact can modify the incidence of reactions related to plasmaconcentrationofdrugsandmetabolitesdueto
modifi-cationsinmetabolization,excretionordistribution,butnotin reactionssuchashypersensitivity,thatarenotdose depend-ent.Intheirwork,Jorcketal.24consideredhyperammonemia followingthe administrationofasparaginaseasserum lev-els above80mol/Linneonatesand100mol/Linchildren olderthanoneyear,demonstratingthegreatersusceptibility ofyoungerindividualstohyperammonemiareactions.
Thefindingsofthepresentstudysuggestthatearly with-drawal of EcA due to suspected hypersensitivity may be mistaken because of the possibility of hyperammonemia ornon-allergic hypersensitivityreactions.Inthissense, the dosageofammonia beforeand afterasparaginaseinfusion andtheclassificationastothegradeofthesuspected hyper-sensitivity reactionare proposed strategiestomonitor and inthedifferentialdiagnosis ofthereactions thatcanguide clinicalstaffinthedecisionofcontinuingorinterrupting treat-mentwithEcA.Burkeetal.reportelevatedserumammonia levelsasevidenceofnon-antibody-mediatedreactionsduring intravenousasparaginaseinfusion.28
Thedosageofammoniaischeap(R$4.20–lessthanUS$ 1.50)and thetechniqueusedissimple(colorimetrictestof drychemistryusingthebromophenolbluereagent). Measure-mentofammoniaalsopermitstheanalysisoftheinactivation oftheenzyme,asammonia serumlevels canhelptoinfer aboutenzymeactivity.23Amarkedincreaseinammonia lev-elsisexpectedinpatientswhodonotshowantibodies,since ammonia isone of the productsof the reaction catalyzed by asparaginase and antibodies are associatedwith minor increasesofammonia.
Thetranslationoftheresearchresultsintothepracticeof theserviceallowedtheimplementationofanactive pharma-covigilancestrategybymonitoringboththeadministrationof allinfusionsofasparaginaseandammonialevels.Reactions areclassifiedaccordingtotheseverityandthetimeafterthe infusion,whichpromotesgreatersafetyintheidentificationof thereaction.Thisstrategyalsoallowsanindirectmeasureof asparaginaseactivityusingammonialevelsduetothelowcost andbecausethisexaminationwasadoptedbytheinstitution forotherpurposes.
Becausethiswasaretrospectivestudy,someofthe sus-pectedadversereactionshadnodescriptionofthesignsand symptoms,whichmadeitimpossibletoanalyzetheseverityof all.Inaddition,thereviewoftheliteratureandtheriskfactors foundinthepresentstudymakeitclearthatnotallreactions reported asallergichypersensitivity in theclinical practice wereactuallythistypeofreaction.Itcanbeimpliedthatthere were casesofreal allergichypersensitivity and others that werenot,however,thepreciseclassificationofallreactions astothetypeandseverityisinfeasibleretrospectively.
Conclusion
BecauseofthepredominanceofGrade1and2reactions andthe lackofclassificationofmanyofthereactionsthat occurredduringthestudyperiod,itisexpectedthatthistool willreducethediscontinuationoftreatmentwith asparagi-nase.
Thisreductioninthenumber ofearly interruptionsdue to reactions that may not be related to antibody forma-tion should positively impact the survival of individuals, sincethis drugisan essentialcomponent ofpediatricALL protocols.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. InstitutoNacionaldoCâncer.Epidemiologiadostumoresda crianc¸aedoadolescente[Internet];2015.Availablefrom: http://www.inca.gov.br/conteudo view.asp?id=349[accessed 20.11.15].
2. MüllerHJ,BoosJ.Useofl-asparaginaseinchildhoodALL.Crit RevOncolHematol.1998;28(2):97–113.
3. PietersR,HungerSP,BoosJ,RizzariC,SilvermanL,Baruchel A,etal.l-Asparaginasetreatmentinacutelymphoblastic leukemia:afocusonErwiniaasparaginase.Cancer. 2011;117(2):238–49.
4. VanderSluisIM,VroomanIM,PietersR,BaruchelA, EscherichG,GouldenN,etal.Consensusexpert recommendationsforidentificationandmanagementof asparaginasehypersensitivityandsilentinactivation. Haematogica.2016;101(3):279–85.
5. AsselinB,RizarriC.Asparaginasepharmacokineticsand implicationsoftherapeuticdrugmonitoring.Leuk Lymphoma.2015;56(8):2273–80.
6. WorldAllergyOrganization.Drugallergies[Internet];2017. Availablefrom:http://www.worldallergy.org/professional/ allergicdiseasescenter/drugallergy/[accessed03.01.17]. 7. RuggieroA,TriaricoS,TrombatoreG,BattistaA,Dell’acquaF,
RizzariC,etal.Incidence,clinicalfeaturesandmanagement ofhypersensitivityreactionstochemotherapeuticdrugsin childrenwithcancer.EurJClinPharmacol.
2013;69(10):1739–46.
8. SyrigouE,MakriliaN,KotiI,SaifMW,SyrigosKN,etal. Hypersensitivityreactionstoantineoplasticagents:an overview.AntiCancerDrugs.2009;20(1):1–6.
9. EnsinaLF,FernandesFR,GesuGD,MalamanMF,Chavarria ML,BerndLA.Reac¸õesdehipersensibilidadea
medicamentos.RevBrasAlergimunopatol.2009;32(2):42–7. 10.BurkeMJ.Howtomanageasparaginasehipersensitivityin
acutelymphoblasticleukemia.FutureOncol. 2014;10(16):2615–27.
11.StaryJ,ZimmermannM,CampbellM,CastilloL,DibarE, DonskaS,etal.Intensivechemotherapyforchildhoodacute lymphoblasticleukemia:resultsoftherandomized intercontinentaltrialALLIC-BFM2002.JClinOncol. 2014;32(3):174–85.
12.AsselinB.Immunologyofinfusionreactionsinthetreatment ofpatientswithacutelymphoblasticleucemia.FutureOncol. 2016;12(13):1609–21.
13.RaetzEA,SalzerWL.Tolerabilityandefficacyof l-asparaginasetherapyinpediatricpatientswithacute lymphoblasticleukemia.JPediatrHematolOncol. 2010;32(7):554–63.
14.AvramisVL,PanosyanEH.
Pharmacokinetic/pharmacodynamicrelationshipsof asparaginaseformulations:thepast,thepresentand recommendationsforthefuture.ClinPharmacokinet. 2005;44(4):367–93.
15.CampbellM,CastilloL,RiccheriC,JanicD,JazbecJ,Kaiserova E,etal.ALLIC-BFM2009.ArandomizedtrialoftheI-BFM-SG forthemanagementofchildhoodnon-Bacutelymphoblastic leukemia[Internet];2016.Availablefrom:http://tphd.org.tr/ 5thhematolojisempozyumu/LebrizYukselALLICBFM
2009.pdf[accessed18.12.16].
16.MinistériodaSaúde.Sistemadeinformac¸ões ambulato-riais:manualdebasestécnicas[Internet];2017.Availablefrom: http://www1.inca.gov.br/inca/Arquivos/comunicacao/manual debasestecnicasoncologia.pdf[accessed10.02.17].
17.CzogalaM,BalwierzW,SztefkoK,RogatkoI.Clinicalutilityof ammoniaconcentrationasadiagnostictestinmonitoringof thetreatmentwithl-asparaginaseinchildrenwithacute lymphoblasticleukemia[Internet].BiomedResInt.2014. Availablefrom:
https://www.hindawi.com/journals/bmri/2014/945860/ [accessed23.07.14].
18.NaranjoCA,BustoU,SellersEM,SandorP,RuizI,RobertsEA, etal.Amethodforestimatingtheprobabilityofadversedrug reactions.ClinPharmacolTher.1981;30(2):239–45.
19.SucarDD.Interac¸ãomedicamentosadevenlafaxinacom captopril.RevBrasdePsiquiatr.2000;22(3):134–7.
20.BrackenL[thesis]Avoidingadversedrugreactionsinchildren –developmentoftheliverpooladversedrugreaction avoidabilityassessmenttool.Liverpool:Universityof Liverpool;2015.p.23.
21.NacionalCancerInstitute(NCI).CommonTerminology CriteriaforAdverseEventsv3.0(CTCAE)[Internet];2006. Availablefrom:https://ctep.cancer.gov/protocoldevelopment/ electronicapplications/docs/ctcaev3.pdf[accessed09.08.06]. 22.WooMH,HakLJ,StormMC,SandlundJT,RibeiroRC,Rivera
GK,etal.Hypersensitivityordevelopmentofantibodiesto asparaginasedoesnotimpacttreatmentoutcomeof childhoodacutelymphoblasticleukemia.JClinOncol. 2000;18(7):1525–32.
23.ShinnickSE,BrowningML,KoontzSE.Managing
hipersensitivitytoasparaginaseinpediatrics,adolescents, andyoungadults.JPediatrOncolNurs.2013;30(2):63–77. 24.JorckC,KiessW,WeigelJF,MützeU,BierbachU,BebloS.
Transienthyperammonemiaduetol-asparaginasetherapyin childrenwithacutelymphoblasticleukemiaornon-hodgkin lymphoma.PediatrHematolOncol.2011;28(1):3–9.
25.KlossRQ,PietersR,EscherichG,VanderSluisIM.Alergic-like reactionstoasparaginase:atypicalallergieswithout
asparaginaseinactivation.PediatrBloodCancer. 2016;63(11):1928–34.
26.LiuC,KawediaJD,ChengC,PeiD,FernandezCA,CaiX,etal. Clinicalutilityandimplicationsofasparaginaseantibodiesin acutelymphoblasticleukemia.Leukemia.2012;26(11):2303–9. 27.SeybertHW,RaneA,SchwabM.Pediatricclinical
pharmacology.Berlin:Springer;2011.p.205.