Pleasecitethisarticleinpressas:GeorgeF,etal.AlargeoutbreakofLegionnaires’DiseaseinanindustrialtowninPortugal.RevPortSaúde w w w . e l s e v i e r . p t / r p s p
Original
article
A
large
outbreak
of
Legionnaires’
Disease
in
an
industrial
town
in
Portugal
Francisco
George
a,∗,
Tara
Shivaji
a,
Catia
Sousa
Pinto
a,
Luis
Antonio
Oliveira
Serra
a,
João
Valente
a,
Maria
João
Albuquerque
a,
Paula
Cristina
Olivenc¸a
Vicêncio
a,
Ana
San-Bento
a,
Paulo
Diegues
a,
Paulo
Jorge
Nogueira
a,
Teresa
Marques
a,
Helena
Rebelo
b,
Filipa
Costa
b,
Raquel
Rodrigues
b,
Alexandra
Nunes
b,
Vitor
Borges
b,
João
Paulo
Gomes
b,
Daniel
Sampaio
b,
Paula
Barreiro
b,
Silvia
Duarte
b,
Dina
Carpinteiro
b,
Joana
Mendonc¸a
b,
Catarina
Silva
b,
Luís
Vieira
b,
Maria
Joao
Simões
b,
Paulo
Gonc¸alves
b,
Baltazar
Nunes
b,
Carlos
Dias
b,
Jorge
Machado
b,
Fernando
Almeida
b,
Elsa
A
Goncalves
c,
Lucilia
Carvalho
d,
Pedro
Viterbo
e,
Dilia
Jardim
f,
Nuno
Lacasta
f,
Filomena
Boavida
f,
Ana
Perez
f,
Isabel
Santana
g,
Paula
Matias
g,
Nuno
Banza
g,
Carlos
Rabacal
haDirec¸ãoGeraldaSaúde,MinistériodaSaúde,Lisboa,Portugal
bInstitutoNacionaldeSaúdeDr.RicardoJorge,MinistériodaSaúde,Lisboa,Portugal cCentroHospitalardeLisboaOriental,MinistériodaSaúde,Lisboa,Portugal
dCentrodeEstudosAnglísticos,UniversidadedeLisboa,MinistériodaCiência,TecnologiaeEnsinoSuperior,Lisboa,Portugal eInstitutoPortuguêsdoMaredaAtmosfera,MinistériodoAmbiente,Lisboa,Portugal
fAgênciaPortuguesadoAmbiente,MinistériodoAmbiente,Amadora,Portugal
gInspec¸ão-GeraldaAgricultura,doMar,doAmbienteedoOrdenamentoTerritorial,MinistériodoAmbiente,MinistériodaAgricultura,
DesenvolvimentoRuraleFlorestaleMinistériodoMar,Lisboa,Portugal
hHospitaldeVilaFrancadeXira,MinistériodaSaúde,VilaFrancadeXira,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received13October2016 Accepted14October2016 Availableonlinexxx
Keywords:
Legionnaires’disease
Legionellapneumophilafraseri
a
b
s
t
r
a
c
t
Background:WedescribetheinvestigationandcontrolofanoutbreakofLegionnaires’ dis-easeinPortugalinOctober,NovemberandDecember2014.
Methods:Confirmed cases were individuals with pneumonia, laboratory evidence of
Legionellapneumophilaserogroup1andexposure,byresidence,occupationalorleisureto theaffectedmunicipalities.49possiblesourceswerereducedtofourpotentialsources,all industrieswithwetcoolingsystem,followingriskassessment.Wegeo-referencedcases’ res-idencesandthelocationofcoolingtowersdefiningfourstudyareas10kmbuffercentered oneachcoolingtowersystem.Wecomparedthenumberofcaseswithexpectednumbers, calculatedfromtheoutbreak’sattackratesappliedto2011censuspopulation.UsingStones’ Test,wetestedobservedtoexpectedratiosfordeclineinrisk,withdistanceupto10kmfour directions.IsolatesofLegionellapneumophilawerecomparedusingmolecularmethods.
∗ Correspondingauthor.
E-mailaddress:[email protected](F.George).
http://dx.doi.org/10.1016/j.rpsp.2016.10.001
Pleasecitethisarticleinpressas:GeorgeF,etal.AlargeoutbreakofLegionnaires’DiseaseinanindustrialtowninPortugal.RevPortSaúde Results: Weidentified403cases,377ofwhichwereconfirmed,14patientsdied.Patients becameillbetween14Octoberand2December.ANEwindandthermalinversionwere recordedduringtheestimatedperiodofexposure.Diseaseriskwashighestinpeople liv-ingsouthwestfromalloftheindustriesidentifiedanddecreasedwithdistance(p<0.001). 71clinicalisolatesdemonstratedanidenticalSBTprofiletoanisolatefromacoolingtower. WholegenomesequencingidentifiedanunusualL.pneumophilasubsp.fraseriserogroup1 astheoutbreakcausativestrain,andconfirmedisolates’relatedness.
Conclusions: Industrialwetcoolingsystems,bacteriawithenhancedsurvivalcharacteristics andacombinationofclimaticconditionscontributedtothesecondlargestoutbreakof Legionnaires’diseaserecordedinternationally.
©2016TheAuthor(s).PublishedbyElsevierEspa ˜na,S.L.U.onbehalfofEscolaNacionalde Sa ´udeP ´ublica.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Um
grande
surto
da
Doenc¸a
dos
Legionários
numa
cidade
industrial
em
Portugal
Palavras-chave:
Doenc¸adosLegionários
Legionellapneumophilafraseri
r
e
s
u
m
o
Contexto:Descrevemosainvestigac¸ãoepidemiológicaemedidasdecontrolodeumsurtode doenc¸adosLegionários,ocorridoemPortugalemoutubro,novembroedezembrode2014.
Métodos: Adefinic¸ãodecasoengloboudoentescomcritériosclínicosdepneumoniaaguda, comprovasimagiológicascompatíveiseconfirmac¸ãolaboratorialparaaidentificac¸ãode
Legionellapneumophila(L.pneumophila)serogrupo1,paraalémdocritérioepidemiológico de exposic¸ão,querpor motivosderesidência,ocupacionaloulazernasfreguesias sus-peitas.Quarentaenovepossíveisfontesdeinfec¸ãoforamreduzidasa4potenciaisfontes, apósavaliac¸ãode risco,todasasindústriascomsistemade torresdearrefecimento.A georreferenciac¸ãoporresidênciadoscasoselocalizac¸ãodetorrespermitiudefinir4áreasde investigac¸ãonumperímetrode10kmcentradoemcadaumadaquelas4torres. Comparou-seonúmerodecasosobservadoscomonúmerodecasosesperados,calculadosapartirde taxasdeataquedosurtoaplicadasàpopulac¸ão.UsandootestedeStones,testou-searazão entrecasosobservadosecasosesperadosedeclíniodoriscoemrelac¸ãoàdistânciadeaté 10kmem4direc¸ões.AsamostrasdeL.pneumophilaforamcomparadasutilizandométodos moleculares.
Resultados: Foramidentificados403casos,dosquais377foramconfirmados,tendo ocor-rido14óbitos.Osdoentesapresentaramsintomasentre14deoutubroe2dedezembro.Em termosmeteorológicos,foramregistadosventosNEeinversãotérmicaduranteoperíodo estimadode exposic¸ão.Oriscodedoenc¸afoimaiorempessoasquevivemasudoeste detodasasindústriasidentificadas,diminuindocomoaumentodadistância(p<0,001). Amostrasde71doscasosclínicosdemonstraramumperfilSBTidênticoàsamostras iso-ladasapartirdeumatorredearrefecimento.AsequênciadegenomadeL.pneumophila fraseriserogrupo1poucocomumcomoaestirpecausadoradosurtoconfirmouarelac¸ão dasamostrasisoladas.
Conclusões: Torresdearrefecimentoindustriais,agentesbacterianoscomcaracterísticas mais desenvolvidas para elevada sobrevivência e uma rara combinac¸ão de condic¸ões climáticas,contribuíramparaosegundomaiorsurtodedoenc¸adosLegionáriosregistado naliteratura.
©2016OAutor(s).PublicadoporElsevierEspa ˜na,S.L.U.emnomedeEscolaNacionalde Sa ´udeP ´ublica.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
On 7November 2014,the Directorate-Generalof Health in Portugal was informed by a local hospital laboratory of 18 patients with Legionnaires’ disease,all admitted inthe
Pleasecitethisarticleinpressas:GeorgeF,etal.AlargeoutbreakofLegionnaires’DiseaseinanindustrialtowninPortugal.RevPortSaúde outbreakinvestigation,wepresentedareportthathasbeen
publishedasarapidcommunication, providingpreliminary dataoftheepidemiological,microbiologicaland environmen-talinvestigation.1Thisarticlepresentsthefinalresultsofthe outbreakinvestigation.
Legionnaires’ disease, first described during the 1976 PhiladelphiaAmericanLegionconference2isabacterial pneu-monicinfectionwithLegionellaespecies.Mostcasesattributed to L.pneumophila sg1.3 Disease characteristically develops 2–10 days after the inhalation of aerosolized bacteria by susceptibleindividuals.Riskfactorsincludesmoking,older individualsandthosewithchroniccardiorespiratorydisease.4 Water,eitherinnaturalorartificialaquaticenvironments,is thereservoirforLegionellaespecies.5
From2008to2012,between88and140caseswerereported annually in Portugal of which the majority were sporadic communityacquiredcases.6Largecommunityoutbreakscan resultinsignificantmorbidityandmortalityinashortspace oftime,5thelargesttodatewasreportedin2001inMurcia, Spainwith449cases.7
Frequently identified as the source oflarge community outbreaks,industrialcoolingtowersystemssource8areable todisseminatecontaminatedaerosolsoverlargedistances.9 Meteorologicalfactors,industrialoperationalconditionsand inadequatemaintenanceareriskfactorsforLegionella out-breaksassociatedwithtowers.8,10
Methods
Definitions
AconfirmedcaseofLegionnaires’diseasehadradiologically confirmedpneumoniawithsymptomonsetbetween12 Octo-beránd02December2014,wholivedorworkedwithin10km ofVila Franca de Xira and had laboratory confirmation of infection.Thelaboratorycriteriaforaconfirmedcaseincluded theisolationofLegionellaspp.fromrespiratorysecretions,the detectionofL.pneumophilasg1antigeninurine,asignificant riseinspecificantibodyleveltoL.pneumophilasg1inpaired serum samples. We defined a probable case differed only inthe laboratory detection of eitherLegionella spp. nucleic acidinrespiratorysecretionsorasinglehighlevelofspecific antibodytoL.pneumophilasg1.
Identificationofcasesandassessmentofexposure
Caseswere identifiedbyreviewingstatutorylaboratoryand electronic clinical notifications from 1 October 2014. Staff fromregionalhealthauthoritiesinterviewedallconfirmedand probablecasesapplyingastandardPortugueseLegionnaires’ diseasequestionnairewhichrecordeddemographic, epidemi-ologicalandclinicaldetails.Theresidentialaddressofeach casewasgeocodedinGoogleEarth.
Toidentifydeaths, weregularly cross-matchedthe out-break database with the Portuguese real time information systemfordeathcertification(SICO),fromNovember2014to March2015.
Sourceidentification
PossiblesourcesofLegionellacontamination,including indus-tries withwet coolingsystems,hospitals, mallsand public recreationfacilitieswereidentifiedand,asameasureof pre-cautioncloseduntilenvironmentalinvestigation.Operational andmaintenancereportswerecheckedandsamplestakento screenforthepresenceLegionellaspp.,resultsledtothe identi-ficationofpotentialsources.Thelocationsofpotentialsources weremappedusingvisualpinpointinginGoogleEarth.
Microbiological,phenotypicandgenotypiccharacterization
Detection of L. pneumophila sg 1 antigen was performed usingspecificurinaryantigentestsinhospitallaboratories. Respiratoryandbloodspecimenswereprocessedatthe ref-erencelaboratory,theNationalInstituteofHealthDrRicardo Jorge.Environmentalsampleswereobtainedduring inspec-tionscarriedoutbytheGeneralInspectorateforAgriculture, Sea, Environment and SpatialPlanninginaccordance with Portugueseregulations,andprocessedbytheatthereference laboratory,theNationalInstituteofHealthDrRicardoJorge.
Clinicalandenvironmentalsampleswereanalyzedusing cultureand/ormoleculartechniques.Clinicalspecimenswere cultured on BCYE-based media and environmental sam-ples were cultured in GVPC selective media. Isolates were identifiedbycommerciallatex-agglutinationkits(Legionella latexTest,Oxoid,UnitedKingdomandMicrogenLegionella, Microgen® Bioproducts,). Culture results for clinical sam-ples were checked by real-time PCR targeted to the 16S
and/or mip genes (L. pneumophila Real-TM, Sacace Biotech-nologies,Italy;ArgeneLegiopneumo/Ccr-gene,bioMérieux, France).Isolates,orculture-negative/PCRpositivespecimens, werecharacterizedbysequence-basedtyping(SBT)in accor-dance with the guidance of the European Working Group forLegionellaInfections(EWGLI).11 Thesevenlociwere sub-jectedtoSangersequencingbyusingBigDyev1.1chemistry on a3130XLGeneticAnalyzer(Applied Biosystems).Whole genomesequencing(WGS)wasperformedfor10clinicaland oneenvironmentalsampleonaMiSeqinstrument(Illumina Inc., San Diego,USA) using using MiSeq V2 flowcells and 150bppaired-endreads(depthofcoverage>100-fold)to ascer-tain their similarity. Illumina reads were assembled using Velvetversion1.2.10.12
PhenotypiccharacterizationofL.pneumophilasg1usedthe Dresdenpanelofmonoclonalantibodies(MAbs)consistingof sixMAbsplustheMAb3oftheInternationalPanelobtained fromtheAmericanTypeCultureCollection(ATCC).Analysis followedanestablishedalgorithm,endorsedbyEWGLIwhich cancharacterizeL.pneumophilaintooneofninesubgroups; Knoxville,Philadelphia,France/Allentown,Benidorm,OLDA, Oxford,Heysham,CamperdownandBellingham.13Thepanel includedantibodiestoMAb3/1whichisconsideredasa viru-lencemarkerduetohighhydrophobicityofthesestrains.
Meteorologicalandairqualityaspects
Pleasecitethisarticleinpressas:GeorgeF,etal.AlargeoutbreakofLegionnaires’DiseaseinanindustrialtowninPortugal.RevPortSaúde
70
Estimated period of aerosol exposure
Date of symptom onset (2014)
Outbreak declared Environmental sampling and shutdown of cooling systems
Cases in workers/ contractors of two factories 60 50 40 30
Number of confir
med cases
20
10
0
14-out 15-out 16-out 17-out 18-out 19-out 20-out 21-out 22-out 23-out 24-out 25-out 26-out 27-out 28-out 29-out 30-out 31-out 1-no
v 2-no v 3-no v 4-no v 5-no v 6-no v 7-no v 8-no v 9-no v 10-no v 11-no v 12-no v 13-no v 14-no v 15-no v 16-no v 17-no v 18-no v 19-no v 20-no v 21-no v 22-no v 23-no v 24-no v 25-no v 26-no v 27-no v 28-no v 29-no v 30-no v 1-dec 2-dec
Fig.1–ConfirmedcasesofLegionnaires’diseasebydateofsymptomonset,VilaFrancadeXira,Portugal,14October–2 December2014(n=377).
recordingsoftemperatureandoncedailyrecordingsof humid-ity,airquality,windspeedanddirectionwerecollectedforthe periodof18October–1November2014.
Statisticalanalysis
Weconductedasourceproximityanalysisoffour potential sourcestotestthehypothesisthatriskofdiseasewasinversely relatedtodistancefromthesource.UsingQGISsoftware,a bufferof10kmradiusfurthersubdividedintoconcentric1km rings was placedon the towers of each industrial cooling system.Thebufferandringswerethendividedintofour quad-rants,NorthEast,SouthEast,SouthWestandNorthWest.We comparedthenumber ofcaseswithexpectednumbers.To calculateexpectedcases,ageand sexspecificratesforthe outbreakwere appliedtothesubsection populationcounts fromthe2011census.Subsectionswerecategorized accord-ingtothedistanceanddirectionoftheirgeographicalcentroid fromeachsource.Theexpectednumberofcasesforeachband quadrantwascalculatedasthesumoftheexpectedcasesfor thesubsectionswhosecentroidslaywithinit.UsingStones’ Test(ST),wetestedobservedtoexpectedratiosfordecline inrisk,withdistanceupto10km inthe NorthEast,North West,SouthEastand SouthWest14 with 9999MonteCarlo simulationsandsetthecut-offforstatisticalsignificanceat 0.05.15
BackcalculationmodelsdevelopedbyEganetal.16 were usedtoestimatetheperiodofaerosolizedreleaseatthestart oftheoutbreak.Themodelswererepeatedusingcasesnotified uptoMarch2015.StatisticalanalysiswasconductedusingR statisticalsoftware.
Results
Outbreakdescription
By2December2014,403casesofdiseasewereidentifiedof which377confirmedand26probablecases.Fourteenpeople died(casefatality3.5%).
Confirmedcasedevelopedsymptomsbetween14October and 2 December 2014. The number of cases peaked on 6 November and the outbreak was declared on 7 November (Fig.1).
ThehighestattackrateswereseenintheparishofPóvoa de Santa Iria/Fortede Casa (60 per 10,000population) and droppedwithincreasingdistancefromthisparish(Fig.2).
Therewere252confirmedcasesinmen(66%).Themedian age was 59 years, the attack rate was higher in men and increased with age in both sexes (25.1 per 10,000 men aged20–64years versus37.9 per 10,000menagedover 65) andwomen(9.0per10,000womenaged20–64yearsversus 26.1casesper10,000womenagedover65).
Twohundredandeight(55%)confirmedcasesalsoreported increaseddiseasesusceptibilitymostcommonlydueto smok-ingandchroniccardiorespiratorydisease.
Sourceidentification
Pleasecitethisarticleinpressas:GeorgeF,etal.AlargeoutbreakofLegionnaires’DiseaseinanindustrialtowninPortugal.RevPortSaúde Fig.2–MapshowingtheattackrateofLegionnaires’diseasebyplaceofresidence(parish),VilaFrancadeXira,Portugal.
Threeoutofthefourpotentialsourcesreportedsuspected casesamongemployees,ninecaseswereconfirmed.
Microbiologicalandphenotypicanalysisandgenetic characterization
The reference laboratory received 95 environmental sam-ples from 49 possible sources, of which, L. pneumophila
positive cultures were isolated in 8. These samples
originated from four industries with wet cooling sys-tems and one commercial premises. Six of the 8 positive cultures were L. pneumophila sg 2–15 (75%). L. pneumophila
Pleasecitethisarticleinpressas:GeorgeF,etal.AlargeoutbreakofLegionnaires’DiseaseinanindustrialtowninPortugal.RevPortSaúde
152 samples for further analysis including serology, respiratory secretions and isolated strains
130 serology/ respiratory/ bronchial secretions
22 strains isolated after culture in hospital laboratories
98 positive for Legionella pneumophila SG1
72 samples positive on PCR
14 samples positive on culture 12 samples
serology unique titre positive
108 samples underwent SBT analysis
75 samples complete SBT characterization
33 samples incomplete SBT characterization
1 sample ST23 1 sample ST62 1 sample ST94 1 sample ST1967
71 samples ST1905
≥4 alleles characterized 15 samples ST1905
≤4 alleles characterized 18 samples
10 isolates underwent Whole
Genome Sequencing (WGS)
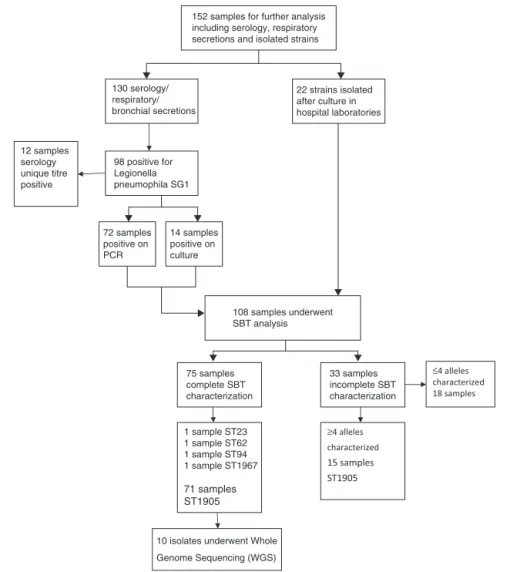
Fig.3–Microbiolologicalprocessingandresultsofclinicalspecimens.
Laboratoryconfirmationofcaseswasdoneby;urinary anti-gentestingforL.pneumophilasg1(92%);seroconversion(2%); PCR(3%) and uniquetiter toL.pneumophila (3%). 152 clini-calspecimensweresenttothereferencelaboratory.Ofthese, 71revealedthepresenceofL.pneumophilasg1withidentical ST1905SBTprofile.
37isolatesofL.pneumophila sg1underwent phenotypic characterization,35 isolatesfrom clinical samplesand two from environmentalsamples. All 37 isolatespresentedthe same phenotypic characteristic; subtype France/Allentown andpossessedthevirulence-associatedepitoperecognizedby monoclonalantibodyMAb3/1(Fig.3).
To confirm the genetic relatedness of ST1905 isolates, 10 out of the 71 clinical isolates and one environmental positive isolateobtained from the industrial coolingtower werenominallyselectedforwholegenomesequencing.We were able to use about 99.8% of each draft sequence and foundnonucleotidedifferenceswithinthecompared3.47Mb ofthe genome. Phylogeneticanalysis involving multiple L. pneumophilaisolatesfromacrosstheworldrevealedthatthe ST1905 cluster clearly diverged from the branch enrolling themoststudiedL.pneumophilastrains(serogroups1,6and
12)17–19 and was more closely related with L. pneumophila subsp.fraseristrains(serogroup4,5and15).20WGS confirma-tionoftheST1905allelicprofilehighlightedabiasassociated with the in silico extraction of the allele sequence for themompSlocus.Thestudiedstraindisplayednon-matching
mompScopies,whichhamperedaproperSTattributionifSBT wasexclusivelydeterminedinsilico(Fig.4).
Meteorological,climate,andairqualityresults
Pleasecitethisarticleinpressas:GeorgeF,etal.AlargeoutbreakofLegionnaires’DiseaseinanindustrialtowninPortugal.RevPortSaúde Fig.4–Phylogenetictreecomparingthewholegenomesequenceofenvironmentalandclinicalisolates.
Periodofexposureassessment
Thebestfittingback-calculationmodelssuggestedalogistic growthoftheenvironmentalexposure,withgreatestintensity between16Octoberand4November(Fig.1).
Sourceproximityanalysisresults
When the source proximityanalysis was conducted, there were 365 confirmed cases, of which 328 (90%) were geo-referencedtowithin10kmofoneofthefourpotentialsources (Fig.5).
All four potential sources demonstrated a significant declineindisease riskwithincreasingdistance(clustering) intheSWQuadrant.Thehighestclustering(ST157,p<0.001) wasobservedintheSWquadrant ofindustry 1.Clustering wasalsoobservedwithindustry2(ST117,p<0.001),industry 3(ST126,p<0.001)andindustry4(ST66.1,p<0.001).Therisk ofdiseasefellconsistentlywithincreasingdistancefromthe sourcewithnoevidenceofpeaksortroughsinthisquadrant. NoclusteringwasobservedintheSEquadrantsofany indus-try,anareathatlargelycomprisedoftheriver.Industry1and2 demonstratedalowerdegreeofclusteringintheNEquadrant (ST5,p=0.01andST4.2,p=0.01respectively).Clusteringwas alsodemonstratedintheNWquadrantofindustry1(ST3.9,
p=0.01).
Discussion
We identified four industries with wet cooling system as the most likely sources of the second largest outbreak of Legionnaires’diseaserecordedwith403casesand14deaths. ElevatedconcentrationsofL.pneumophilasg1ST1905 demon-stratingthevirulentMAb3–1subgroupwereidentifiedinthe towers ofoneindustry. UsingSBT andWGS, wewere able toconfirmthegeneticrelatednessoftheoutbreak-associated clinicalandenvironmentalstrains.Theonlypositiveisolates forL.pneumophilasg1,werebothobtainedfromthecooling towerofoneindustry.SimilarconcentrationsofL.pneumophila
havebeen isolated inother coolingtowersassociatedwith outbreaks.5Itisprobable,thoughunproventhat cross con-tamination of the four closely located towers contributed tothe magnitudeofthe outbreakand haspreviously been described.21
Pleasecitethisarticleinpressas:GeorgeF,etal.AlargeoutbreakofLegionnaires’DiseaseinanindustrialtowninPortugal.RevPortSaúde Fig.5–Legionnaires’diseasenearfourindustrieswithwetcoolingsystemsbydistanceofresidencefromthetower(s).
Theoutbreakoccurredinadenselypopulatedareacloseto thecapitalcityofPortugalcontainingheavilyusedcommuter routesfrom suburbanareas.Theactualnumbers ofpeople exposedwaslikelytohavebeenmuchhigherthanthe resi-dentpopulation.Standarddiagnostictestsmaynotdetectall cases.3ThefigurespresenteddonotcontaincasesofPontiac feverorsuspectedcaseswho testednegativeandtherefore probablyunderestimates the morbidityexperienced bythe
Pleasecitethisarticleinpressas:GeorgeF,etal.AlargeoutbreakofLegionnaires’DiseaseinanindustrialtowninPortugal.RevPortSaúde (LpPhiladelphia-1,LpParis,LpLens,LpCorby,andLp2300/99
Alcoy).Itwas foundtobeclosely related toL.pneumophila
subsp. fraseri strainsfrom serogroupsother than sg1. The studiedstrain harbors an exclusive ∼38kb genomic region comparedwiththenextmostphylogeneticallyrelatedstrain. Thisregionwasfoundtobeintactandhighlysimilar(BLASTn, cover100%,identity99%,E-value0.0)onlyinonestrain(ATCC 33761=DSM 21215) of L. oakridgensis, a species that rarely causesLegionnaires’disease.25Wewouldexplainthelowcase fatalityobservedin terms ofearlydiagnosis and appropri-ateand timelytreatment, whetherthe uniquetraitsofthe outbreak-associatedstrainunderlieimportantcharacteristics oflethalityremainsunderstudy.
Thesourceproximityanalysisestimatedexpected num-bers of cases from the resident population, which likely led to an underestimation of exposure. We reasoned that residentialinformationwas collectedsystematically,unlike displacementhistory,alsoconditionsforthehorizontal prop-agation of aerosols were more pronounced at night time when most residents would have been in their homes. Amorerobustapproachwould havetoperformthe analy-sisaspartofacasecontrolstudy,whichcouldalsoinclude exposuresinnonresidents.Althoughinitiallydiscussed,we didnotproceed withacase–control study due toresource and time constraints. The close geographical proximity of the towers meant that there was overlap of some of the studyareasrenderingitpossible,butunlikelythataclosely locatedsourcecouldleadtopresenceofadistancedecline relationshipforanothersource.Comparingthegeospatial dis-tributionofcaseswithplumemodelingofaerosolcouldbeof valuetoassesstheimpactofcloselylocatedsourcesoneach other.
Thisoutbreakwasthesecondlargestoutbreakof Legion-naires’ disease recorded to date and adds to the body of evidence regarding the impact of climatic conditions and bacterialphenotypesincoolingtowerassociatedcommunity outbreaksofLegionnaires’disease.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
Acknowledgements
OrganizationsandindividualsinvolvedintheTaskForcefor theLegionnaires’DiseaseoutbreakinVilaFrancadeXira;staff fromHospitaldeVilaFrancadeXira,HospitalCUF Descober-tas,CentroHospitalar deLisboa Central,CentroHospitalar deLisboaNorte;CentroHospitalardeLisboaOcidental;staff of the health authorities ofLisbon and Tagus Valley, cen-tral Portugal,northPortugal and the Algarve. Dr.Christian Lucke,TecnischeUniversitatDresden,forsupplyingtheMAbs reagents.MarionMuelhen,andPaulaVasconcelosforcritical review of the manuscript. Emmanuel Robesyn for techni-caladviceongeospatialanalysistechniquesinLegionnaires’ disease.
r
e
f
e
r
e
n
c
e
s
1.ShivajiT,SousaPintoC,San-BentoA,OliveiraSerraLA,
ValenteJ,MachadoJ,etal.Alargecommunityoutbreakof
Legionnaires’diseaseinVilaFrancadeXira,Portugal,October
toNovember2014.EuroSurveill.2014;19,pii:20991.
2.FraserDW,TsaiTR,OrensteinW,ParkinWE,BeechamHJ,
SharrarRG,etal.Legionnaires’disease:Descriptionofan
epidemicofpneumonia.NEnglJMed.1977;297:1189–97.
3.FieldsBS,BensonRF,BesserRE.LegionellaandLegionnaires’
disease:25yearsofinvestigation.ClinMicrobiolRev.
2002;15:506–26.
4.PhinN,Parry-FordF,HarrisonT,StaggHR,ZhangN,KartikK,
etal.EpidemiologyandclinicalmanagementofLegionnaires’
disease.LancetInfectDis.2014;14:1011–21.
5.WorldHealthOrganization.Legionellaandtheprevention
oflegionellosis.Geneva:WHO;2007.p.40.
6.EuropeanCentreforDiseasePrevention,Control(ECDC).
Annualepidemiologicalreport2014,respiratorytract
infections.Stockholm:ECDC;2014.p.17.
7.García-FulgueirasA,NavarroC,FenollD,GarcíaJ,
González-DiegoP,Jiménez-Bu ˜nualesT,etal.Legionnaires’
diseaseoutbreakinMurcia,Spain.EmergInfectDis.
2003;9:915–21.
8.WalserSM,GerstnerDG,BrennerB,HöllerC,LieblB,HerrCE.
Assessingtheenvironmentalhealthrelevanceofcooling
towers:Asystematicreviewoflegionellosisoutbreaks.IntJ
HygEnvironHealth.2014;217:145–54.
9.NguyenTMN,IlefD,JarraudS,RouilL,CampeseC,CheD,
etal.Acommunity-wideoutbreakoflegionnairesdisease
linkedtoindustrialcoolingtowers:Howfarcan
contaminatedaerosolsspread?JInfectDis.2006;193:102–11.
10.MouchtouriVA,GoutzianaG,KremastinouJ,
HadjichristodoulouC.Legionellaspeciescolonizationin
coolingtowers:Riskfactorsandassessmentofcontrol
measures.AmJInfectControl.2010;38:50–5.
11.GaiaV,FryNK,AfsharB,LückPC,MeugnierH,EtienneJ,etal.
Consensussequence-basedschemeforepidemiological
typingofclinicalandenvironmentalisolatesofLegionella
pneumophila.JClinMicrobiol.2005;43:2047–205.
12.ZerbinoDR,BirneyE.Velvet:Algorithmsfordenovoshort
readassemblyusingdeBruijngraphs.GenomeRes.
2008;18:821–9.
13.HelbigJH,SverkerB,PastorisMC,EtienneJ,GaiaV,LauwersS,
etal.Pan-Europeanstudyonculture-provenLegionnaires’
disease:DistributionofLegionellapneumophilaserogroups
andmonoclonalsubgroups.EurJClinMicrobiolInfectDis.
2002;21:710–6.
14.BullM,HallIM,LeachS,RobesynE.Theapplicationof
geographicinformationsystemsandspatialdataduring
Legionnairesdiseaseoutbreakresponses.EuroSurveill.
2012;17:20331.
15.TangoT.Statisticalmethodsfordiseaseclustering.NewYork,
NY:SpringerScience&BusinessMedia;2010.p.191.
16.EganJR,HallIM,LemonDJ,LeachS.ModelingLegionnaires’
diseaseoutbreaks:Estimatingthetimingofanaerosolized
releaseusingsymptom-onsetdates.Epidemiology.
2011;22:188–98.
17.KhanMA,KnoxN,PrasharA,AlexanderD,Abdel-NourM,
DuncanC,etal.Comparativegenomicsrevealthat
host-innateimmuneresponsesinfluencetheclinical
prevalenceofLegionellapneumophilaserogroups.PLoSONE.
2013;8:e67298.
Pleasecitethisarticleinpressas:GeorgeF,etal.AlargeoutbreakofLegionnaires’DiseaseinanindustrialtowninPortugal.RevPortSaúde BMCGenomics.2011;12:536,
http://dx.doi.org/10.1186/1471-2164-12-536.
19.MaJ,HeY,HuB,LuoZQ.Genomesequenceofan environmentalisolateofthebacterialpathogenLegionella pneumophila.GenomeAnnounc.2013;1:e00320-13,
http://dx.doi.org/10.1128/genomeA.00320-13.
20.KoKS,LeeHK,ParkMY,ParkMS,LeeKH,WooSY,etal.
PopulationgeneticstructureofLegionellapneumophilainferred
fromRNApolymerasegene(rpoB)andDotAgene(dotA)
sequences.JBacteriol.2002;184:2123–30.
21.KoolJL,BuchholzU,PetersonC,BrownEW,BensonRF,
PrucklerJM,etal.Strengthsandlimitationsofmolecular
subtypinginacommunityoutbreakofLegionnaires’disease.
EpidemiolInfect.2000;125:599–608.
22.BenthamRH,BroadbentCR.Amodelforautumnoutbreaksof
Legionnaires’diseaseassociatedwithcoolingtowers,linked
tosystemoperationandsize.EpidemiolInfect.
1993;111:287–95.
23.DitommasoS,GiacomuzziM,RiveraSR,RasoR,FerreroP,
ZottiCM.VirulenceofLegionellapneumophilastrainsisolated
fromhospitalwatersystemandhealthcare-associated
Legionnaires’diseaseinNorthernItalybetween2004and
2009.BMCInfectDis.2014;14:483.
24.HelbigJH,LückPC,KnirelYA,WitzlebW,ZähringerU.
Molecularcharacterizationofavirulence-associatedepitope
onthelipopolysaccharideofLegionellapneumophila
serogroup1.EpidemiolInfect.1995;115:71–8.
25.BrzuszkiewiczE,SchulzT,RydzewskiK,DanielR,GillmaierN,
DittmannC,etal.LegionellaoakridgensisATCC33761
genomesequenceandphenotypiccharacterizationrevealsits
replicationcapacityinamoebae.IntJMedMicrobiol.