www.jped.com.br
ORIGINAL
ARTICLE
Fibrinogen:
cardiometabolic
risk
marker
in
obese
or
overweight
children
and
adolescents
夽
,
夽夽
Waldeneide
F.
Azevedo
a,b,
Anajás
S.C.
Cantalice
c,
Nathalia
C.
Gonzaga
d,
Mônica
O.
da
S.
Simões
c,e,
Anna
Larissa
V.
Guimarães
a,
Danielle
F.
de
Carvalho
e,
Carla
Campos
Muniz
Medeiros
e,∗aUniversidadeEstadualdaParaíba(UEPB),CampinaGrande,PB,Brazil
bUniversidadeFederaldeCampinaGrande(UFCG),CampinaGrande,PB,Brazil cUniversidadeFederaldaParaíba(UFPB),JoãoPessoa,PB,Brazil
dUniversidadeFederaldoCeará(UFC),Fortaleza,CE,Brazil
eMasterPost-graduationPrograminPublicHealth,UniversidadeEstadualdaParaíba(UEPB),CampinaGrande,PB,Brazil
Received18July2014;accepted24November2014 Availableonline10June2015
KEYWORDS
Fibrinogen; Obesity; Atherosclerosis; Children; Adolescents
Abstract
Objectives: Todeterminetheprevalenceofincreasedserumfibrinogenlevelsandits associa-tionwithcardiometabolicriskfactorsinoverweightorobesechildrenandadolescents. Methods: Cross-sectional study with 138 children and adolescents (overweight or obese) followedatareferenceoutpatientclinicofthepublichealthcarenetwork.Fibrinogen concen-tration was divided into quartiles, and values above or equal to the third quartile were consideredhigh.Theassociationbetweenhighfibrinogenvaluesandcardiometabolicrisk fac-torswasassessedusingPearson’schi-squaredtestorFisher’sexacttest,asnecessary.Logistic regressionwasusedtoadjustvariablespredictiveoffibrinogenlevels.Analyseswereperformed usingSPSSversion22.0andSASsoftware,consideringaconfidenceintervalof95%.
Results: Serum fibrinogenlevels wereelevatedin 28.3%ofindividuals, showing association withthepresenceofhighCRP(p=0.003,PR:2.41,95%CI:1.30---4.46)andthepresenceoffour ormoreriskfactors(p=0.042;PR:1.78,95%CI:1.00---3.17).Afteralogisticregression,only elevatedCRPremainedassociatedwithalteredfibrinogenlevels(p=0.024;PR:1.32;95%CI: 1.09---5.25).
夽 Pleasecite thisarticleas: AzevedoWF,Cantalice AS, Gonzaga NC, SimõesMO, GuimarãesAL, de CarvalhoDF,et al. Fibrinogen:
cardiometabolicriskmarkerinobeseoroverweightchildrenandadolescents.JPediatr(RioJ).2015;91:464---70.
夽夽
StudyconductedatNúcleodeEstudosemPesquisasEpidemiológicas(NEPE),CentrodeObesidadeInfantil(COI),UniversidadeEstadual
daParaíba(UEPB),JoãoPessoa,PB,Brazil.
∗Correspondingauthor.
E-mail:[email protected](C.C.M.Medeiros). http://dx.doi.org/10.1016/j.jped.2014.11.007
Conclusions: Increased fibrinogenwas prevalentinthestudy populationandwasassociated with ultrasensitiveC-reactive protein andthe presenceoffour or more cardiovascularrisk factors;itshouldbeincludedintheassessmentofindividualsatrisk.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Fibrinogênio; Obesidade; Aterosclerose; Crianc¸as; Adolescentes
Fibrinogênio:marcadorderiscocardiometabólicoemcrianc¸aseadolescentesobesos
oucomsobrepeso
Resumo
Objetivos: Verificaraprevalênciadeníveisséricoselevadosdefibrinogênioesuaassociac¸ão comosfatoresderiscocardiometabólicosemcrianc¸aseadolescentescomsobrepesoou obesi-dade.
Métodos: Estudotransversalcom138crianc¸aseadolescentes(obesosoucomsobrepeso) acom-panhadosemumambulatóriodereferênciadaredepública.Aconcentrac¸ãodofibrinogêniofoi distribuídaemquartis,sendoconsideradaelevadaquandoosvaloreseramiguaisousuperiores aoterceiroquartil.Aassociac¸ãoentreovalorelevadodofibrinogêniocomosfatoresderisco cardiometabólicosfoiverificadaatravésdotestequi-quadradodePearsonoutesteexatode Fisher,quandonecessário.Aregressãologísticafoiutilizadaparaajustedasvariáveis predi-torasdoníveldofibrinogênio.AsanálisesforamrealizadasnoSPSS22.0eSAS,considerando-se ointervalodeconfianc¸ade95%.
Resultados: Osníveisséricosdefibrinogênioestiveramelevadosem28.3%dosindivíduos, apre-sentando associac¸ão com a PCR elevada (RP: 2.41; IC 95%: 1.30---4.46, p=0.003) e com a presenc¸a dequatro oumaisfatores de risco(RP: 1.78; IC95%:1.00---3.17; p=0.042).Após aregressãologística,apenasoPCRelevadocontinuouassociadoaofibrinogênioalterado(RP: 1.32;IC95%1.09---5.25;p=0.024).
Conclusões: Oaumentodofibrinogêniofoiprevalentenapopulac¸ãoestudadaeesteveassociado àproteínaCreativaultrassensíveleaonúmeroigualousuperioraquatrodefatoresderisco cardiovasculares,devendoserincluídonaavaliac¸ãodeindivíduossobrisco.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
The prevalence of excess weighthas increasedin allage groupsin Brazil,similartowhathasoccurred worldwide.1
Data from the Family Budget Survey2 show that the
pro-portion of obese children has increased four-fold in the
last 20 years and three-fold in adolescents in the same
period, findings similar to those observed in developed
countries.3,4
Obesityrepresentsasubclinicalinflammatorycondition
thatresultsinaconsiderablenumberofcardiometabolicrisk factors.5 Stoopa etal.,6 when assessing theinflammatory
andprothromboticstatusofchildrenandadolescentswith
obesityornormalweight,foundelevatedfibrinogenlevelsat anageasyoungas6yearsintheobesechildren,regardless ofpubertalstatus.
Inflammation in atherogenesisis causedby the
synthe-sis, secretion, and storage of proinflammatory cytokines
by adipocytes, producing a state of low-grade
inflamma-tionwithvascularandmetaboliccomplications7thatleads
tovascular endothelial dysfunction,considered to be the
onset of the atherogenic process.8 Coagulation factors,
such as fibrinogen, blood flow, and inflammatory factors,
havegainedimportanceinestablishingtheatherosclerotic
processandareconsideredimportant riskfactors for car-diovasculardisease.7,9
Fibrinogen,anacutephaseprotein,ispartofthegroup
ofinflammatorybiomarkersproducedbyhepatocytesandis
consideredanimportantmarkertomonitorthe
atheroscle-rotic inflammatory process evolution,10 as it acts on the
genesisoftheatherothromboticprocessthroughregulation ofcell adhesionand proliferation,vasoconstrictionat the siteofendothelial injury,stimulationof platelet aggrega-tion,andbloodviscosity.7,8
Although the association of obesity with
hyperfibrino-genemia has been reported in children, the association
of fibrinogen withcardiometabolic risk factors is not yet well-established.11,12 The search for biomarkers for early
identification of individuals at higher risk of
develop-ing atherosclerosis and the knowledge of its association
withother cardiometabolic risk factors is critical for the
understandinganddevelopmentof interventionsaimedat
reducingmorbidity andmortality fromcardiovascular
dis-ease.
Thus,thisstudy aimedtodetermine theprevalence of
elevatedserumlevelsoffibrinogenanditsassociationwith cardiometabolicriskfactorsinoverweightorobesechildren
Methods
Cross-sectional study, conducted between June of 2011 and April of 2012, at the Centro de Obesidade Infantil (ChildhoodObesity Center--- COI), located at Institutode SaúdeElpídeodeAlmeida(ISEA),CampinaGrande-PB.COI is a referral service for childhoodobesity in the city and consists of researchers and a multidisciplinary team that includes doctors (pediatrician and endocrinologist), phar-macists,nutritionists,psychologists,nurses,socialworkers, andphysicaleducationprofessionals.
Whentheresearchbegan,therewere450obeseor over-weightchildrenandadolescentsenrolledatCOI.Thestudy included those who attended COI throughout the study period,comprising a convenience sample of 138 children andadolescents.Thosewithdiseasesreceivingmedication thatinterferedwithglucoseorlipidmetabolism;thosewith adiagnosisofgeneticsyndrome;andthosewhoachieveda nutritionalstatusofnormalweightwereexcluded.Forstudy purposes, the calculation of the sample statistical power wasperformedretrospectivelyinordertoallowestimation of alteredfibrinogen prevalence of 28.3%, toensure that thesamplesizeallowedattainingtheproposedobjectives. Formeasuresofassociation,thesampleshowedastatistical powerof85%(ˇ=15%)fortheconfidencelevelof95%.
Theanthropometricvariables(weight,height,andwaist circumference)wereverifiedinduplicate, consideringthe meanvalueoftwomeasurements,accordingtothe recom-mendationsoftheWorldHealthOrganization(WHO).13
Nutritionalstatuswasclassifiedaccordingtobodymass
index (BMI),as recommended by the Centers for Disease
Control and Prevention (CDC) as overweight (BMI ≥85th
percentileand<95th percentile),obesity (BMI≥95th
per-centile and <97th percentile), and severe obesity (BMI
≥97thpercentile).14 Waistcircumference(WC)was
consid-ered increased when ≥the 90th percentile, according to
theInternationalDiabetesFederation(IDF).15 witha
maxi-mumlimitof88cmforgirlsand102cmforboys,according totheNationalCholesterolEducationProgram-Adult Treat-mentPanelIII(NCEP-ATPIII).16
Blood pressure was measured by the oscillometric
method in a Tycos® (Welch Allyn Inc., NY, USA) device,
accordingtothe guidelinesestablished inthe VIBrazilian GuidelinesonArterialHypertension.17
Total cholesterol (TC),high-density lipoprotein
choles-terol (HDL-C), triglycerides (TG), and glycemia were
evaluated by the enzymatic colorimetric method in
automated equipment (BioSystems, Model 310, Applied
Biosystems, CA, USA); fibrinogen was measured by the
coagulometric method; high-sensitivity C-reactive protein
(hs-CRP) and insulin by chemiluminescence in IMMULITE
1000automatedequipment(Siemens®,SiemensHealthcare,
Erlangen, Germany). Low-density lipoprotein (LDL-c) was
calculatedusingtheFriedewaldformula.18Bloodcollection
wasperformedaftera12-hfastingperiod.
TheHomeostasisModelAssessmentofInsulinResistance
(HOMA-IR)wasusedasthecriterionfordiagnosisofinsulin resistance (IR), classified as suchwhen values ≥2.5 were
found.19
The following were considered cardiometabolic risk
factors:BMI≥97thpercentile,WC≥90thpercentilefor
gen-der, age, and ethnicity, with a maximum limit of 88cm
for girls and 102cm for boys16; systolic blood pressure
(SBP) and/or diastolic blood pressure (DBP) ≥90th
per-centilefor gender, height,and age17;TG ≥130mg/dL, TC ≥170mg/dL;HDL-c<45mg/dL;LDL-c ≥130mg/dL; fasting
glucose ≥100mg/dL; insulin ≥15IU/mL; HOMA-IR ≥2.5;
andCRP>3mg/L.20,21 IndividualswithCRP ≥10mg/Lwere
excludedfromtheanalysisofthisvariable,asinthesecases,
it is recommended to rule out the presence of an acute
inflammatoryprocess.21
Fibrinogenlevelsweredividedintoquartiles;values≥the
75thpercentileofthesample,whichcorrespondsto3.4g/L, wereconsideredhigh,asthereisnoestablishedcutofffor thepediatricpopulation.22
TheprojectwasapprovedbytheResearchEthics
Com-mittee of UniversidadeEstadual da Paraíba (UEPB)(CAEE
--- 0256.0.133.000-1) and was performed after parents or
guardianssignedaninformedconsent,authorizingthe par-ticipationoftheirchildreninthestudy.
Thedataareshownaspercentageandmedian,withthe
respectiveinterquartilerange(IQ).Theassociationbetween high fibrinogen values (values≥the 75thpercentile) with
gender, age, nutritionalstatus, WC, SBP, DBP, TG,HDL-c,
LDL-c,TC,bloodglucose,insulin,HOMA-IR,andhs-CRPwas
evaluated by Pearson’s chi-squared test or Fisher’s exact
test, as necessary, with prevalence ratios (PR) and their
respectiveconfidenceintervals.
After performing the Kolmogorov---Smirnov test, which
verifiedanon-parametricdistributionof the‘‘fibrinogen’’ variable, the Kruskal---Wallis test was applied to test the association of the fibrinogen median withnutritional sta-tus(overweight,obesity,andsevereobesity) andwiththe numberofcardiometabolicriskfactors(1=oneriskfactor; 2=tworiskfactors; 3=threerisk factors,4=fouror more riskfactors).Subsequently,theMann---Whitneytestwasused
toevaluatethedifferenceofthesemeasuresbetweeneach
group,adjusted toensurethatthe˛errordidnotexceed
thevalueof0.05.
Multiplelogisticregressionwasusedtoadjustthe varia-bles, whosecriteriaforinclusion wasthe associationwith
the dependent variable in the bivariate analysis with a
p-value<0.20. The variables were included in the regres-sionanalysis usingthe‘‘Enter’’ method,according tothe
decreasingvalueofthePR.TheHosmerandLemeshowtest
was used as a measure of goodness-of-fit of the logistic
regression models, in which a p≥0.05 indicates that the
modelisadjusted.
The analyses were performed using the SPSS program,
version 22.0 (SPSS Inc, Chicago, USA) and SAS University
Edition (SAS Institute Inc., Cary, NC, USA), considering a confidenceintervalof95%(95%CI).
Results
Biological, clinical, and laboratory characteristics of the 138assessedsubjectsaredescribedinTables1and2.The
observed percentage for cardiometabolicrisk factors was
5.8%foronlyonefactor,13.0%fortwo,28.3%forthree,and 52.9%forfourormorefactors.
Elevatedfibrinogenlevelswerepresentin28.3% ofthe
participants, and were more common in children than in
Table1 Frequencydistributionofthebiologicalandclinicalvariablesaccordingtofibrinogenlevelsinchildrenandadolescents withoverweightorobesity.
Variables Fibrinogen(g/L) PR(95%CI) p
≥3.4(n=39) <3.4(n=99)
n(%) n(%)
Gender Male 28(34.1) 54(65.9) 1.74 0.063a
Female 11(19.6) 45(80.4) (0.95---3.20)
Agerange Childhood 13(43.3) 17(56.7) 1.80 0.038a
Adolescence 26(24.1) 82(75.9) (1.06---3.05)
Nutritionalstatus BMI≥p97 27(31.0) 60(69.0) 1.32 0.345a
BMI<p97 12(23.5) 39(76.5) (0.73---2.37)
WC WC≥p90 32(30.2) 74(69.8) 1.34 0.549b
WC<p90 7(22.6) 24(77.4) (0.66---2.73)
SBP SBP≥p90 9(36.0) 16(64.0) 1.39 0.439b
SBP<p90 29(25.9) 83(74.1) (0.76---2.56)
DBP DBP≥p90 12(27.9) 31(72.1) 0.97 0.922a
DBP<p90 27(28.7) 67(71.3) (0.55---1.73)
CRF ≥4 26(35.6) 47(64.4) 1.78 0.042a
<4 13(20.0) 52(80.0) (1.00---3.17)
WC,waistcircumference;SBP,systolicbloodpressure;DBP,diastolicbloodpressure;CRF,cardiometabolicriskfactors.
a Descriptivelevelofprobabilityofthechi-squaredtest.
b Descriptivelevelofprobabilityofcorrection.
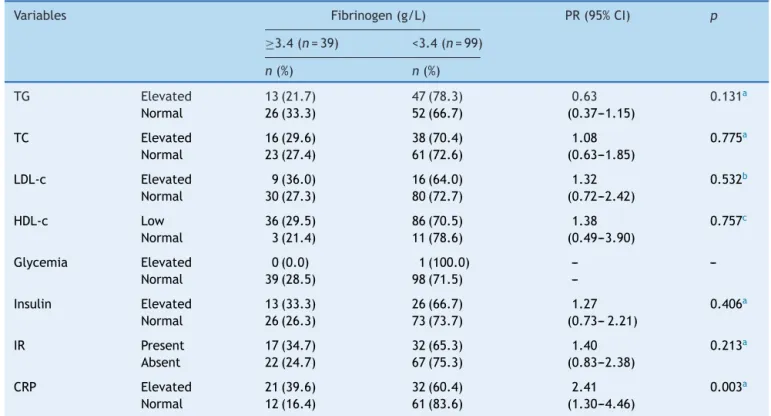
Table2 Frequencydistributionoflaboratoryvariablesaccordingtofibrinogengroupsinchildrenandadolescentswith over-weightorobesity.
Variables Fibrinogen(g/L) PR(95%CI) p
≥3.4(n=39) <3.4(n=99)
n(%) n(%)
TG Elevated 13(21.7) 47(78.3) 0.63 0.131a
Normal 26(33.3) 52(66.7) (0.37---1.15)
TC Elevated 16(29.6) 38(70.4) 1.08 0.775a
Normal 23(27.4) 61(72.6) (0.63---1.85)
LDL-c Elevated 9(36.0) 16(64.0) 1.32 0.532b
Normal 30(27.3) 80(72.7) (0.72---2.42)
HDL-c Low 36(29.5) 86(70.5) 1.38 0.757c
Normal 3(21.4) 11(78.6) (0.49---3.90)
Glycemia Elevated 0(0.0) 1(100.0) --- ---Normal 39(28.5) 98(71.5)
---Insulin Elevated 13(33.3) 26(66.7) 1.27 0.406a
Normal 26(26.3) 73(73.7) (0.73---2.21)
IR Present 17(34.7) 32(65.3) 1.40 0.213a
Absent 22(24.7) 67(75.3) (0.83---2.38)
CRP Elevated 21(39.6) 32(60.4) 2.41 0.003a
Normal 12(16.4) 61(83.6) (1.30---4.46)
TG, triglycerides;TC, totalcholesterol;LDL-c, low-densitylipoproteincholesterol; HDL-c,high-density lipoproteincholesterol;IR,
insulin-resistance;CRP,C-reactiveprotein.
a Descriptivelevelofprobabilityofthechi-squaredtest.
b Descriptivelevelofprobabilityofcorrection.
Table3 Valuesofcrudeandadjustedprevalenceratio(95%CI)offibrinogenalterationsinchildren andadolescentswith overweightorobesity.
Parameter Variables CrudePR AdjustedPR Adjustedp(95%CI) HosmerandLemeshow
Fibrinogen CRP>3mg/L 2.41 1.32 0.024(1.091---5.253)
0.648 CRF≥4 1.78 1.11 0.545(0.483---2.591)
Agerange(10---19years) 1.80 0.78 0.263(0.211---1.260)
CRP,C-reactiveprotein;CRF,cardiometabolicriskfactors.
withfour or more cardiometabolicrisk factors (p=0.042; PR: 1.78;95% CI: 1.00---3.17), andin those withhigh CRP levels(p=0.003;PR: 2.41; 95% CI:1.30---4.46). The latter waspresentin52.9%oftheparticipants.
Therewasnostatisticallysignificantdifferencein rela-tiontofibrinogenmedianwithnutritionalstatuscategories: overweight=3.0 (IQ: 2.3---3.6); obesity=2.5 (IQ:2.1---3.2); severeobesity=2.6(IQ:2.2---3.5);p=0.284.Intherelation tothecardiometabolicrisk,itwasobservedthatthe fibrino-genmedianincreasedasthenumberofriskfactorsincreased (p=0.002).Thisdifferenceoccurredinthegroupswithtwo andfourormoreriskfactors(p=0.003;Fig.1).
At the multiple logistic regression, CRP level>3mg/L
was independently associated with high fibrinogen levels
(≥the75thpercentile),withariskof1.32(p=0.024;95%CI: 1.09---5.25).Thefinalmodel,whichincludedasexplanatory variablesCRPlevels>3mg/L,thenumberofriskfactors≥4,
andtheagegroup(10---18years)showedagoodfit,assessed
bytheHosmerandLemeshowtest(0.648;Table3).
Discussion
Inthepresentstudy,mostassessedindividualswereobese andhadfour or morecardiometabolicrisk factors.It was alsoobservedthathighleveloffibrinogen,oneofthe pro-thromboticstate evaluation factors,was present in more
Med. median; IQ. interquartile range.
Median f
ibr
inoge
n
Med: 2.1 IQ: 1.9-3.5
*P=3.003 Group 2 vs. Group 4 Med: 2.2 IQ: 2.0-3.1
Number of risk factors
Med: 2.4 IQ: 2.2-3.3
Med: 2.9 IQ: 2.4-3.5
≥ 4 0.0
1 2 3
1.0 2.0
3.0 P=.002
*
*
Figure1 Medianfibrinogenconcentration,accordingtothe number of cardiometabolic risk factors. Med, median; IQ, interquartilerange.
thanonequarterofthesample.Theprothromboticstateis consideredastheimbalancebetweenprocoagulantand pro-fibrinolytic factors,characterized, mainlyfromlaboratory analysis, by increase in fibrinogen levels, by plasminogen activationinhibitor-1(PAI-1),andbyactivationofthe coag-ulation pathways, as well as associated with endothelial dysfunction.23
Inobeseindividuals,theincreaseinfibrinogenlevelsand othercoagulationfactors,suchasPAI-1andvonWillebrand
factor (vWF-Ag),has been associatedwith an increase in
cardiovascularevents.24Somestudies8,22havefound
signifi-cantlyhigherfibrinogenlevelsinoverweightchildren,when comparedwithlevelsfoundinchildrenwithnormalweight.
The high levelsof fibrinogen inobese children maybe
explainedbytheincreaseinitssynthesis.Althoughthereis noreportofitsproductionbyadiposetissue,thereleaseof adipocytokinesinto theportal circulation would influence theproductionoffibrinogen andothercoagulationfactors intheliver.7
Astudycarriedoutwith313obesechildrenand adoles-centsdetectedalowerprevalenceofincreaseinfibrinogen levels(10.7%)24whencomparedtothatinthepresentstudy
(28.3%).Thiscanbeexplainedbecausetheabovementioned
study useda cutoff(4.0g/Lto4.5g/L)toconsider
fibrin-ogenlevels aselevated, whichwashigher than thatused
in thepresent study(3.4g/L). Suchcomparisons between
studiesaredifficult,asthereisnoconsensusforthenormal value of fibrinogen levelsin childhood.25 Additionally, the
behaviorof cardiovascularriskfactorsmayvaryaccording toethnicity.24
Fibrinogenlevelsfoundincurrentstudiesareofconcern,
especially becausethey are elevated both in prepubertal
andpubertalobesechildren.6Althoughtheprocessoffatty
streakandatheromatousplaqueformationhavebeen
iden-tifiedpathologically,mainlyin adolescents,thesignificant
increase in markers such asfibrinogen and PAI-1in obese
childrensuggeststheincreaseincardiovascularriskinthis agegroup,whichmaycausetheformationofatherosclerotic plaquesbeforepubertyonsetinyoungobeseindividuals.26
Regardingtheassessedcardiometabolicriskfactors,all children andadolescentshadat leastone riskfactor.The
median of fibrinogen serumlevelswasassociatedwithan
increased number of risk factors. This can be explained
by the potentiation of cardiometabolic risk due to the
aggregationofseveralbiomarkersthatareunfavorablefor cardiovascularhealth.22 This findingreinforcesthe
Studies have also shown the association of some cardiometabolicrisk factors withelevated fibrinogen lev-els from childhood, such as BMI,6,24 HOMA-IR,6,25 fasting
insulin,6,24,25 glycemia,26 triglycerides, total cholesterol,
LDL-c,andlowHDL-c.24
In this study, fibrinogen was associated only with
hs-CRP and the presence of four or more cardiometabolic
risk factors. This may be due to the characteristics of
the sample, which includes only childrenand adolescents
with overweight and obesity, conditions associated with
a proinflammatory state, unlike other abovementioned
studies.6,24,25 Afterthe logistic regression wasperformed,
thevalueofhs-CRPremainedapredictorofhighfibrinogen levelsandwasassociatedwitha1.3-foldhigherchanceof developingthiscondition.
In relation tothe lipidprofile, although noassociation wasfound withfibrinogen,thehighestprevalence oftotal
cholesterolandLDL-Cwasobservedamongthosewhohad
high fibrinogen levels. The association between vascular
alterationsandlipoproteins,especiallythoseoflow-density,
hasbeenexplainedasoriginatingfromthedamageinduced
byoxygen-freeradicals,whichpromotethedestructionof
endothelial cells by oxidizing these lipoproteins,
trigger-ing a cascade of alterations including hypercoagulability
anddecreasedfibrinolysis,signaledbyincreasedfibrinogen production.24
This promotes atherosclerosis through several
mecha-nisms:bybindingtoendothelialcellreceptors(Intercellular
Adhesion Molecule 1-ICAM1); triggering the release of
vasoactivemediators,smooth-musclecellproliferation,and
monocyte chemotaxis induction; and by playing a rolein
foamcellformationandfacilitatingthetransferof choles-terolfromplateletstomacrophagesandmonocytes.6
It is important to note that fibrinogen is an
acute-phaseinflammationproteinwithprocoagulantactivityand, togetherwithhs-CRP,hasbeenusedtopredict cardiovascu-lardiseaseindifferentgroups.Bothseemtobemorereliable markers than interleukin-6 (IL-6), which has a short half-life.27Itshouldalsobenotedthatinflammationplaysakey
roleintheonsetandpromotionofatherosclerosisandcan
leadtoacutecoronarysyndrome(ACS),byinducingplaque
instability.23
This study has some limitations, such as the lack of a
cutoffinliteraturefornormalfibrinogenlevelsinchildren andadolescents,makingitdifficulttocomparestudies;the scopeofagerange,astherearepeculiarcharacteristicsin thedifferent groups, suchaspubertal stage,which inter-fereswiththemetabolismandfatdeposition,althoughthis facthasnotbeenobservedinrelationtofibrinogen;the iso-lateduseoffibrinogenasamarkerfortheassessmentofthe prothromboticstate,althoughsomeresearchersconsiderit amorereliablemarkerofcardiovasculardiseasethanIL-627;
andtheuseofaconveniencesample,whichmaynotreflect thecharacteristicsoftheoverallpopulation.
Itisworthmentioningthattheselimitationsdonot dimin-ishtheimportanceofthisstudy,asitinnovatesbyassessing thefibrinogen behaviorinrelation tocardiometabolicrisk
factors in Brazilian children and adolescents with excess
weight. Thatis due to the fact that studies publishedin
theliterature onthistopichave been conducted inother
countriesand,asmentionedpreviously,thisratiocanvary withethnicity.28
Therefore, thefindings reinforce the concept that the
fibrinogenandhsCRParepotentialbiomarkersthatcanbe
usedin obese children, even in those without associated
complications,forthescreeningofchildrenandadolescents atriskofdevelopingcardiovasculardisease.Itisalso note-worthythatlongitudinalstudiesareneededtoelucidatethe roleof thesebiomarkers inthe genesis of atherosclerotic diseaseinchildhood.
Funding
Research funded by the Programa de Incentivo à Pós-Graduac¸ão e Pesquisa (PROPESQ)Proclamation 01/2008 ---Pró-Reitoria de Pós-Graduac¸ão, Universidade Estadual da Paraíba(PRPGP/UEPB),concessiontermNo.98/2008.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Francescatto C, Santos NS, Coutinho VF,Costa RF. Mothers’ perceptions about the nutritional status of their over-weight children: a systematic review. J Pediatr (Rio J). 2014;90:332---43.
2.BRASIL. Pesquisa de Orc¸amentos Familiares 2008---2009: antropometriaeestadonutricionaldecrianc¸as,adolescentes eadultosnoBrasil.RiodeJaneiro:IBGE;2010.
3.deOnisM,BlossnerM,BorghiE.Globalprevalenceandtrends ofoverweightandobesityamongpreschoolchildren.AmJClin Nutr.2010;92:1257---64.
4.OgdenCL,CarrollMD,KitBK,FlegalKM.Prevalenceofobesity intheUnitedStates,2009---2010.NCHSDataBrief.2012;82:1---8.
5.TzotzasT,EvangelouP,KiortsisDN.Obesity,weightlossand con-ditionalcardiovascularriskfactors.ObesRev.2011;12:282---9.
6.Stoppa-VaucherS,DirlewangerMA,MeierCA,deMoerlooseP, ReberG,Roux-LombardP,etal.Inflammatoryand prothrom-botic states inobese children ofEuropean descent. Obesity (SilverSpring).2012;20:1662---8.
7.KannelWB,WolfPA,CastelliWP,D’AgostinoRB.Fibrinogenand riskofcardiovasculardisease. TheFraminghamStudy.JAMA. 1987;258:1183---6.
8.VanGaalLF,MertensIL,DeBlockCE.Mechanismslinkingobesity withcardiovasculardisease.Nature.2006;444:875---80.
9.BaoW, SrinivasanSR,BerensonGS.Plasmafibrinogenandits correlatesinchildrenfromabiracialcommunity:theBogalusa HeartStudy.PediatrRes.1993;33:323---6.
10.DaneshJ, CollinsR, ApplebyP,PetoR.Association of fibrin-ogen, C-reactive protein, albumin, or leukocyte count with coronaryheartdisease:meta-analysesofprospectivestudies. JAMA.1998;279:1477---82.
11.Valle JM, Estepa RM, Camacho RM. Endothelial dysfunction is related to insulin resistance and inflammatory biomarker levels in obese prepubertal children. Eur J Endocrinol. 2007;156:497---502.
12.CimentiC, ManggeH, HaidlH, Zach D, MunteanW. Throm-bingenerationinseverelyobesechildren.JThrombHaemost. 2006;4:1834---6.
14.CDC.Tableforcalculatedbodymassindexvaluesforselected highsandweightsforages2to20years;2010.Availablefrom: http://www.cdc.gov/growthcharts[cited2010Oct23].
15.The IDF consensus worldwide definition of the metabolic syndrome. International Diabetes Federation. J Diabetes Endocrinol.2005;7(2).
16.ThirdReportofCholesterolEducationProgram(NCEP)Expert PanelonDetection,Evaluation,and TreatmentofHighBlood CholesterolinAdults(AdultTreatmentPanelIII).NIH publica-tionno.01-3670;2000.
17.SociedadeBrasileiradeCardiologia.VIDiretrizesBrasileirasde HipertensãoArterial.ArqBrasCardiol.2010;95:1---51.
18.Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentrationoflow-densitylipoproteincholesterolinplasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499---502.
19.Madeira IR, Carvalho CN, Gazolla FM, de Matos HJ, Borges MA,BordalloMA.Pontodecortedoíndicehomeostaticmodel assessmentforinsulinresistance(homa-ir)avaliadopelacurva receiver operating characteristic (ROC) na detecc¸ão de sín-drome metabólica em crianc¸as pré-púberes com excesso de peso.ArqBrasEndocrinolMetabol.2008;52:1466---73.
20.Giuliano IC, Caramelli B, Pellanda L, Duncan B, Mattos S, FonsecaFA.SociedadeBrasileiradeCardiologia.IDiretrizde prevenc¸ão da aterosclerose do Departamento de Ateroscle-rosedaSociedadeBrasileiradeCardiologia.ArqBrasCardiol. 2001;77:1---48.
21.Lande MB, Pearson TA, Vermilion RP, Auinger P, Fer-nandez ID. Elevated blood pressure, race/ethnicity, and
C-reactive protein levels in children and adolescents. Pedi-atrics.2008;122:1252---7.
22.NagelG,RappK, WabitschM,BücheleG, KrokeA,ZöllnerI, etal.Prevalenceandclusterofcardiometabolicbiomarkersin overweightandobeseschoolchildrenresultsfromalargesurvey insouthwestGermany.ClinChem.2008;54:317---25.
23.TelesCP,FilhoSC,SousaAC,Barreto-FilhoJA.Hipertensão:um estadopró-trombótico,vol.14;2007.p.245---51.
24.Galli-Tsinopoulou A, Kyrgios I, Maggana I, Giannopoulou EZ, KotanidouEP,StylianouC,etal.Insulinresistanceisassociated withatleastthreefoldincreasedriskforprothromboticstatein severelyobeseyoungsters.EurJPediatr.2011;170:879---86.
25.FritschP,KleberM,RosenkranzA,FritschM,MunteanW,Mangge H,etal.Haemostaticalterationsinoverweightchildren: associ-ationsbetweenmetabolicsyndrome,thrombingeneration,and fibrinogenlevels.Atherosclerosis.2010;212:650---5.
26.MaurasN,DelgiornoC,KollmanC,BirdK,MorganM,Sweeten S, et al. Obesity without established comorbidities of the metabolic syndrome is associated withproinflammatory and prothromboticstate,evenbeforetheonsetofpubertyin chil-dren.JClinEndocrinolMetab.2010;95:1060---8.
27.WangQ,YinJ,XuL,ChengH,ZhaoX,XiangH,etal.Prevalence ofmetabolicsyndromeinacohortofChineseschoolchildren: comparisonoftwodefinitionsandassessmentofadipokinesas components byfactor analysis. BMC Public Health.2013;13: 249.