REVISTA
BRASILEIRA
DE
REUMATOLOGIA
ww w . r e u m a t o l o g i a . c o m . b r
Original
article
Translation,
cultural
adaptation,
validity
and
reliability
of
the
shoulder
rating
questionnaire
for
use
in
Brazil
Danilo
Calmon
de
Siqueira
a,∗,
Abrahão
Fontes
Baptista
b,
Israel
Souza
c,
Katia
Nunes
Sá
daFaculdadedeMotricidadeHumana,UniversidadeTécnicadeLisboa,Lisboa,Portugal bInstitutodeCiênciasdaSaúde,UniversidadeFederaldaBahia,Salvador,BA,Brazil cInstitutoFederaldeEducac¸ãoCiênciaeTecnologiadoRiodeJaneiro,Paracambi,RJ,Brazil dEscolaBaianadeMedicinaeSaúdePública,Salvador,BA,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19June2013 Accepted10April2014
Availableonline22October2014
Keywords:
DisabilityEvaluation Questionnaire Shoulder ValidationStudies Translations
a
b
s
t
r
a
c
t
Objective:TotranslateandculturallyadapttheShoulderRatingQuestionnaire(SRQ)tothe BrazilianPortugueselanguage,andtodetermineitsvalidity,reliabilityandsensitivityto changeinpatientswithfunctionalimpairmentoftheshoulder.
Methods:Aftertranslationandback-translation oftheoriginalversionbyfour indepen-denttranslators,theinstrumentwasreviewedbyacommitteeofexpertsandsubsequently appliedtoeightpatientswithshoulderinjury(targetaudience)toproducethePortuguese version.Then,thisversionwasappliedto102patientsselectedfromfourreferencecenters forfunctionaltreatmentoftheshoulder,whohadavarietyofclinicaldiagnoses,educational levels,socioeconomic,andculturalbackgrounds.Theevaluationwasperformedtwicewith anintervaloffourweeksbetweeneachapplication.
Results:TheBrazilianversionofSRQwasequivalentintermsofsemanticsandshowedgood levelsofreliability(Cronbach’sAlpha=0.89andICC=0.83). Thereproducibilitywashigh (SpearmanCorrelationCoefficient=0.82)andvalidityoftheitemsthatrangedfrom0.54to 0.99wasconsideredexcellent.TheCohen’sdandTtestforrepeatedmeasuresshowedthat theinstrumentisabletomonitorandtrackimprovementsinshoulderfunction.
Conclusion: Psychometriccriteriawerefound,whichjustifytheapplicabilityoftheBrazilian versionofSRQinindividualswithshoulderfunctionalimpairments.
©2014ElsevierEditoraLtda.Allrightsreserved.
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rbr.2014.04.006. ∗ Correspondingauthor.
E-mail:[email protected](D.C.deSiqueira).
http://dx.doi.org/10.1016/j.rbre.2014.04.006
Traduc¸ão,
adaptac¸ão
cultural,
validade
e
confiabilidade
do
questionário
de
classificac¸ão
do
ombro
para
uso
no
Brasil
Palavras-chave:
Avaliac¸ãodeIncapacitac¸ão Questionário
Ombro
EstudosdeValidac¸ão Translac¸ões
r
e
s
u
m
o
Objetivo:TraduzireadaptarculturalmenteoShoulderRatingQuestionnaire(SRQ)paraoidioma portuguêsdoBrasil,edeterminarsuavalidade,confiabilidadeesensibilidadeàmudanc¸a empacientescomcomprometimentofuncionaldoombro.
Métodos: Emseguidaàtraduc¸ãoeretro-traduc¸ãodaversãooriginalporquatrotradutores independentes,oinstrumentofoirevisadoporumacomissãodeespecialistas,tendosido subsequentemente aplicadoaoito pacientescomlesão doombro(público-alvo)paraa produc¸ãodaversãoemportuguês.Emseguida,essaversãofoiaplicadaa102pacientes selecionadosdenossoscentrosdereferênciaparatratamentofuncionaldoombro,exibindo diagnósticosclínicos,níveiseducacionaisebasessocioeconômicaseculturaisdiversas.A avaliac¸ãofoirealizadaduasvezescomumintervalodequatrosemanasentreaplicac¸ões.
Resultados: Aversão brasileiradoSRQfoi equivalente emtermosde semântica,tendo demonstrado bons níveis de confiabilidade (Alfa de Cronbach=0,89 e Coeficiente de Correlac¸ãoIntraclasse[CCI]=0,83).Areprodutibilidadefoialta(CoeficientedeCorrelac¸ão deSpearman=0,82)eavalidadedositens,quevarioude0,54até0,99,foiconsiderada exce-lente.OstestesddeCoheneTparamedidasrepetidasdemonstraramqueoinstrumentoé capazdemonitorareacompanharmelhorasnafunc¸ãodoombro.
Conclusão: Oscritériospsicométricosforamatendidos,oquejustificaaaplicabilidadeda versãobrasileiradoSRQemindivíduoscomcomprometimentofuncionaldoombro.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Thereishighincidenceandprevalenceofshoulder muscu-loskeletaldisordersinthegeneralpopulation.Studies have shown that 14% to 21% ofindividuals haveshoulder pain symptoms.Itisestimatedthattwooutofthreeindividuals haveatleastoneepisodeofpainintheneckorshouldersat sometimeintheirlives.1
InBrazil,over80%ofthediagnosesthatresultedinsocial securityaidgrants, accidentanddisabilityretirementwere duetowork-relatedmusculoskeletaldisordersandinvolved mainlytheupperlimbs.2Painandshoulderdysfunctionoften
compromisemotorskills,work activitiesandqualityoflife andrepresentanimportantsocioeconomicproblemby inter-feringwiththeattendanceandproductivityofworkersand resultinhighinvestmentinthesepatients.3,4
Mostshoulderinjuriescause painand functional limita-tions.Thesesymptomsarethereasonsthatleadanindividual toseek medicaltreatment. As thephysical examinationis aninsufficientindicatorforevaluatingfunctionalandsocial aspects,itisnecessarytohaveassessmenttoolsthatcanbe usedinclinicalpractice.5
Toassessaspectsoftheseverityofsymptomsand func-tionalstatusoftheshoulder,questionnairesweredeveloped in the English language. At present, there are versions of some questionnaires for evaluation of the shoulder that havebeenvalidatedandtranslatedintothePortuguese lan-guageinBrazil.Arecentsystematicreviewshowedthatthere aresevenquestionnaireforthispurpose(DASH,WORC,SPADI, PSS,ASORS,ASESeUCLA).6
However,noprospectiveassessmenttoolspecificallyfor the shoulder, such as the Shoulder Rating Questionnaire
(SRQ),hasbeentranslatedinaccordancewiththeappropriate methodologicalrigorofvalidationfortheBrazilianPortuguese language.
A Portuguese version of the SRQ is available to use in Portugal (www.ifisionline.ips.pt/media/2janvol1n2/pdfs/ artigo1voln2.pdf),butitisnotappropriatedtouseinBrazil becauseofculturaldifferences.7Forthisreason,theaimof
thisworkwastomakeacross-culturaltranslationoftheSRQ intothePortugueselanguageofBrazilandhaveitvalidated, inordertoprovideanothertoolforassessingthefunctional statusoftheshoulder.
Methods
Thisaccuracystudywasdevelopedinfoursteps:translation andback-translation,evaluationbyacommitteeofexperts, evaluationbythetargetpopulation,and,finally,application topatientswithshoulderdysfunctioninphysicaltherapyat two time interval,according tothe methodological criteria recommended bythe European Research Group on Health Outcomes (ERGHO),theCenterforHealthResearchandthe UniversityofCoimbra(CEISUC).8,9Documentationshowingall
stepstakenfortranslationandculturaladaptationwassent totheauthoroftheoriginalquestionnaire(Englishversion)to ensuretheadequacyofthetranslationprocesscarriedoutand obtained.Thisstudywasprecededbyaformalauthorization oftheauthorsoftheoriginalversionoftheShoulderRating Questionnaire(SRQ)fortranslationandvalidationtoBrazilian Portuguese.
singleversionafterconsensusbetweenthetwo translators andtheresearchers.Afterthis,theBrazilianPortuguese ver-sionwasretro-translatedtotheoriginallanguagefor compar-isonbytwoothernativeEnglish-speakingtranslators,whose nativelanguageisEnglishandwhodidnotknowthepurpose ofthestudy.These twoEnglishversions underwent anew process of consensus between translators and researchers toreachanEnglishversion,whichwascomparedwiththe originalversion toseeif thereweresignificant differences. ThentheBrazilianPortugueseversionoftheinstrumentwas reviewedbya committeeof expertscomposed ofa physi-cian and two physical therapists, with over five years of clinicalexperienceandknowledgeofthetwolanguages, to verify content validity. For this review, the committeewas askedtocomparetheversionofreconciliation,itembyitem, withthe original version inEnglish, tonote its agreement andsuggestchangesthatcouldimprovethetranslation.Each itemwasalsoevaluatedforitsrelevanceintheevaluationof thecontentinstrument,checkingtheequivalence.Afterthis revision,thesecondversionwaspreparedforreconciliation.
Thethirdstepinvolvedtheassessment,usingthe trans-latedversion,ofeightpatients(onemanandsevenwomen) with shoulder injury and who were beginning with, or undergoingphysicaltherapy.Inthisinterview,thefollowing objectivesweredefined:1)examinethepresence(orabsence) ofquestions oritems that could beconsidered relevantor irrelevant;2)identifyquestionsoritemsthatcouldbe consid-eredredundant;3)analyze,ingeneralterms,acceptabilityand understandabilityofthemeasuringinstrument.Theinterview beganwithabriefexplanationofthework tobedeveloped anditsrationale.Later,thepatientsinterviewedwereasked tocompletethequestionnaire,rememberingthattheinterest didnotlieintheanswers,butintheformulationofthe ques-tions.Asaresultoftheinterviews,ananalysiswasmadeto preparethefinalversionoftheSRQ,inBrazilianPortuguese, tobeusedinthefourthstep.Thesethreestepsconstituted theprocessoflinguisticandculturaladaptationoftheSRQ.
Thefourthphaseofdatacollectionconsistedof applica-tionofthefinalversiontothe102selectedpatientsatfour reference centers for treatment of shoulder function. The questionnairewasappliedontwodifferentoccasionswithan intervaloffourweeksbetweenthem.
Participantswereselectedaccordingtothefollowing inclu-sioncriteria:1)providingaclinicaldiagnosisoftheinjuryto theshoulder(accordingtotheInternationalClassificationof Diseases);and 2) being enrolled in aphysicaltherapy pro-gramforshoulderinjuryattheselectedreferencecenters.The exclusioncriteriawere:1)beingunabletoread,fillingoutand understandthetranslatedquestionnaire;2)havinganytype ofneuromotordeficitorcognitiveimpairment.
After obtaining approval from the Ethics Committee of theBahianFoundationforDevelopmentofSciences(Protocol N◦ 121/2010)andformalauthorizationfromtheinstitutions enrolledinthework,whichwerefourreferencecentersfor thetreatmentofshoulderdysfunctioninSalvador,Bahia, par-ticipantswererecruitedfromaselectionofrecords.
Afterbeing informed about the study objectives, proce-dures used in data collection and clarification of doubts, the volunteers gave their written consent to participate in the study. Patients were selected for a convenience
sampleandsamplesizewasestimated,basedonotherarticles onvalidation.1,5,10
Thefourthphaseincludedanalysisofthereliability, con-struct validity and sensitivity to clinical changes of the BrazilianPortugueseversionofSRQ.Forthereliability anal-ysis, it was necessary to analyze the internal consistency andreproducibility.Toassesstheinternalconsistencyofthe itemsintheinstrument,Cronbach’salphawasused. Repro-ducibilitywastestedbyapplyingthepre-finalversionofthe SRQ on two occasions (test-retest). Spearman’s correlation testandtheintraclasscorrelationwereusedtomeasurethe association ofthe first withthe second application of the instrument.
Forconstructvalidity,theBrazilianPortugueseversionof the American Shoulder and Elbow Surgeons Standardized ShoulderAssessmentForm(ASES)wasusedforcomparison withtheresultsoftheSRQ.Spearman’scorrelationtestwas usedtoevaluatecorrespondencebetweentheresultsofthe instrumentsused(ASESandSRQ).Thefactoranalysisby prin-cipalcomponentsmethodwasusedtoevaluatethevalidityof thecompositionoftheSRQdomains.
Inthefactorialanalysis,thesamplewasdividedintotwo sub-samples.Thefirst,involvedallthepatients(n=102),and excludedtheworkrelateditems,astheyshouldbeanswered onlybythosepatientsthatwereworkingduringthe assess-ment period.Inthe secondsub-sample,onlythe questions thatinvolvedworkactivitieswereused,andansweredonlyby thosewhowereworkingduringtheassessmentperiod(n=46). KMOandBartlett’stestswereusedtoassessadequacyofthe sample.TheAlphaofCronbachwasmadewithHillandHill classification(1999).11,12
Toevaluatethe abilityofthe instrumentto capturethe changesresultingfromthetreatment,theTtestforrepeated measuresandCohen’sdwasused.ThescoresintheSRQtotal scoreofthefirstandsecondevaluationswerecompared. Anal-ysesconsideredanalphavalueof5%.
Results
Ofthe102patientsinvolvedinthestudy,29weremen(28.40%), and73werewomen(71.60%),withmeanageof56.90±12.10 years, with variety in clinical, educational level, socioeco-nomicandculturalaspects.Asregardsshoulderdysfunction, 34(33.30%)reportedhavingimpingement,31(30.40%)rotator cufftear,19(18.60%)adhesivecapsulitis,7(6.90%)proximal humerus fracture, 2 (2.00%) shoulder instability, 3 (2.90%) glenohumeraljointarthritisand6(5.90%)acromioclavicular jointarthritis.
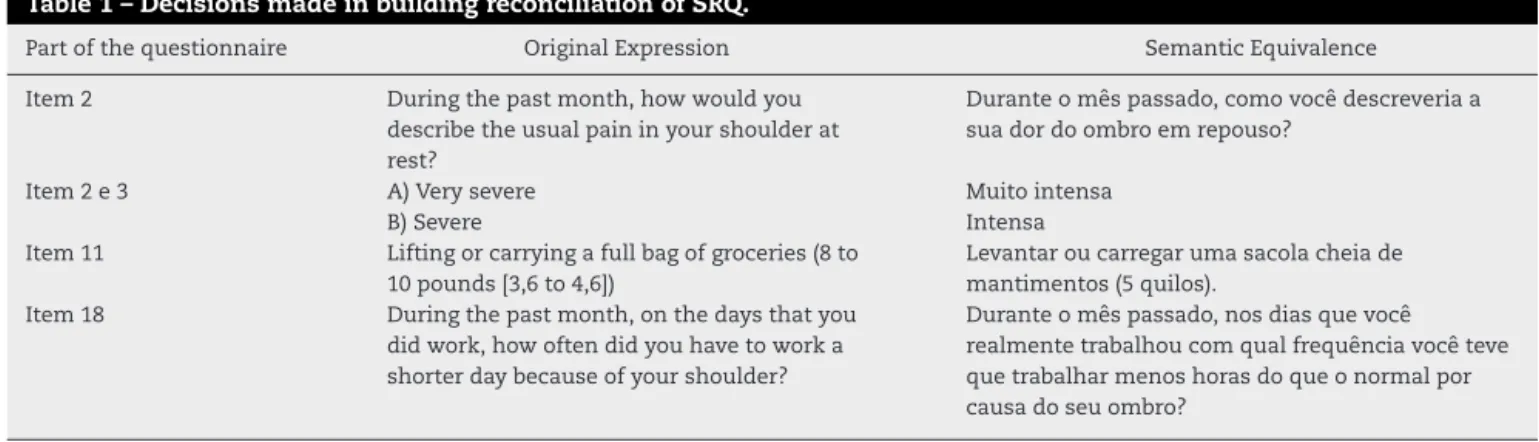
In spite of the similarity of the versions presented by thetranslators,thereweresomeconflictingissuesthatwere discussed and,afterarriving ataconsensus,reconciliation betweentheSRQinPortugueseandthe firstversionofthe ShoulderRatingQuestionnairewasachieved.Thedecisions aresummarizedinTable1.
Table1–DecisionsmadeinbuildingreconciliationofSRQ.
Partofthequestionnaire OriginalExpression SemanticEquivalence
Item2 Duringthepastmonth,howwouldyou
describetheusualpaininyourshoulderat rest?
Duranteomêspassado,comovocêdescreveriaa suadordoombroemrepouso?
Item2e3 A)Verysevere Muitointensa
B)Severe Intensa
Item11 Liftingorcarryingafullbagofgroceries(8to 10pounds[3,6to4,6])
Levantaroucarregarumasacolacheiade mantimentos(5quilos).
Item18 Duringthepastmonth,onthedaysthatyou didwork,howoftendidyouhavetoworka shorterdaybecauseofyourshoulder?
Duranteomêspassado,nosdiasquevocê realmentetrabalhoucomqualfrequênciavocêteve quetrabalharmenoshorasdoqueonormalpor causadoseuombro?
The interview with the target audience resulted in a consensusthatthequestionnairewasalittlelong,but under-standable;couldbeanswered;andwashelpful.Allpatients consideredtheextentappropriatetotheirconditions.Then weproceededwithanindividual analysisofeach question andanswer,tochecktheease/difficultyinunderstandingthe terms used, theinstructions, questions and their response options,aswellasthealternativesproposedbyrespondents whoalwaysidentifiedtheexistenceofanyproblem.
Thus,withregardtoclarity,threeindividualsconsidered the issueconfusing inthe question 21,and had toread it againtounderstandthetext.Becauseofthis,itwasdecided tochangetheanswerstothequestion21,whichare summa-rizedinTable3.Afterthisstep,aBrazilianversionoftheSRQ wasprepared(Appendix1).
Thefactoranalysisrevealedtheadequacyofthesample bymeansofboththeKMOtest(0.81inthe1st sub-sample,
and0.79inthe2ndsub-sample)andBartlett’stest(
2=490.25;
p<0.001in the 1st sub-sample,and 2=122.85;p<0.001 in
the2ndsub-sample).Moreover,itbecameclearthatthe
fac-torloadingswereabove0.30,rangingbetween0.43and0.97, whichindicatedahighdegreeofvalidityoftheitems(Table4). In the first sub-sample,the total variance explained by fourfactorswas74.84%,andthefactorloadingswereabove 0.30,rangingfrom0.43(item6)to0.97(item4).Thetotal vari-anceexplainedbyasinglefactorwas42.76%,andthefactor loadingswereabove0.30,rangingfrom0.31(item1)to0.78 (item6),whichindicatedahighdegreeofvalidityoftheitems inasinglefactor,thusjustifyingtheuseoftheoverallscale scoreasameasurefortheassessmentofshoulderfunction.In
thesecondsub-sample,withonlythequestionsthatinvolved workactivities(fouritems),thetotalvarianceexplainedwas 80.17%,andthefactorloadingswereabove0.30,rangingfrom 0.88(item16)to0.91(item17).Whenallitemswereused,the totalvarianceexplainedbyasinglefactorwas46.10%,andthe factorloadingswereabove0.30,rangingfrom0.43(item14)to 0.88(item17),whichindicatedahighdegreeofvalidityofthe itemsinasinglefactor,thusjustifyingtheuseofthe over-allscalescoreasameasurefortheassessmentofshoulder function.
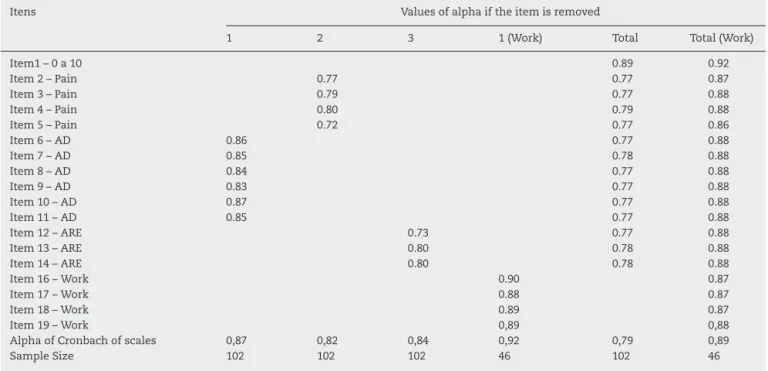
Asregards theresultsoftheinternalconsistencyofthe SRQ, it was observedthat in the overall assessmentof all the itemsthe Cronbach’salphainthe firstsub-samplewas 0.79, which is considered as good/reasonable. If item 1wasremoved,theinternalconsistencywas0.89.Inthesame way,theCronbach’salphawas0.89forthetotalscalewhen consideringonlythesecondsub-sample,andifitem1was removedtheinternalconsistencywas0.92(Table5).A simi-larindexofinternalconsistencywasfoundintheoriginal,in whichCronbach’salphawas0.86.
Inassessingthe reproducibilityoftheinstrument,there wasahighassociationofthefirstwiththesecond applica-tionoftheinstrumentwithaSpearmancorrelationcoefficient of0.82betweenthetotalscores(p<0.001)andanintraclass correlationof0.83(p<0.001).
In assessingthe correspondence betweenthe resultsof the SRQ with the ASES, there was a significant associa-tionbetweenthetotalscoresoftheinstrumentsinthefirst (r=0.49;p<0.001)and thesecondapplicationofthe instru-ment(r=0.67;p<0.001).Therewasalsoasignificantpositive
Table2–ChangesobtainedafterthebacktranslationofthePortugueseversionandthechangesproposedbytheexpert committeeofthenewversionofShoulderRatingQuestionnaire.
Item Consensusaftertheinitialtranslation Afterthecommitteemeeting
1 Muitobem Muitomal Muitobem109876543210Muitomal
7 Vestiroutirarumpulôveroucamisa. Colocaroutirarumcasacooucamisa.
12 Considerandotodasasformasquevocêusaseu ombroduranteatividadesrecreativasou desportivas(ex.:beisebol,golfe,atividades aeróbicas,jardinagem)comovocêdescreveriaa func¸ãodeseuombro?
Considerandotodasasformasquevocêusaoseu ombroduranteasatividadesesportivasoudelazer (ex.vôlei,natac¸ão,atividadesaeróbica,jardinagem, etc.),comovocêdescreveriaafunc¸ãodoseuombro?
13 Duranteomêspassado,quantadificuldadevocê teveemarremessarumabolasobreamãoou fazerumsaquenotênisporcausadeseuombro?
Table3–Changetothequestion21afteranalysisofthetargetaudience.
Item VersionReconciliation Afteranalysisofthetargetaudience
21 Dor MelhoradaDor
Atividadesdiáriaspessoaisedomésticas Melhorapararealizarasatividadesdiáriaspessoais easatividadesdecasa
Atividadesrecreativasouatléticas Melhorapararealizarasatividadesesportivasoude lazer
Trabalho MelhorapararealizarasatividadesdoTrabalho
associationbetweenthedomainsoftheSRQwiththeASES totalscore,rangingfrom0.27to0.66.OnlythefieldofGeneral Assessmentwasnotsignificantlyassociatedwithtotalscore ontheASES.
Notethat, afterthetreatmentperiod,thepatients expe-rienced a significant improvement in SRQ scores (t=-9.86, p<0.001).TheeffectsizeforthismeanmeasuredforCohen’s d was 1.057, indicating a very large effect, implying that the means are likely very different. This indicates that the instrument issuitable formonitoring and can identify improvementsinshoulderfunction.
Discussion
Assistancewithemphasisonlyonthecurativetreatmentof thedisease,basedonthebiomedicalmodel,hasalsoledto revealinghow the disease affects the individual and one’s socialfunctional levels. The model proposed bythe World Health Organization (WHO), which unifies the concept of functionanddysfunction,suggestsacommontaxonomyfor
classifyingtheimpactofthediseaseonpeople’slives,helping toestablishgoalsforrehabilitation.13Inthiscontext,theneed
foradequatefunctionalmeasuresinclinicalpracticebecomes apparent,inadditiontoresearchtodeterminedamage, pre-dictoutcomes,enablefunctionalrehabilitationplanning,and indicateanytreatmentandfunctionalchanges.
Themeasuresoffunctionalstatusareessentialtoassess theperformanceofactivitiesthatareimportantineveryday life.Runquistetal.havingthefunctionalityoftheshoulder as objectofevaluating,usedthe SRQin patientswithloss inthe range ofmotionofthisregion, because ofthe good psychometricpropertiesoftheinstrument.14
OtherauthorshaveshowntheadvantagesofusingtheSRQ compared withother instruments thatassess the function oftheshoulder,asitisaninstrumentwithgoodsensitivity toclinicalchange.15 Basedontheseadvantages,ithasbeen
usedtomonitortheresultsoftreatmentproposalsmadefora longerperiodoftime,ortofollow-upthestageofthechronic disease(eg.adhesivecapsulitis).16,17
Currently,therearemanyquestionnairesthathavebeen developedintheEnglishlanguagetoevaluatethesymptoms
Table4–LoadFactorandCommonalityoftheitems.
Items Factors Communality
1 2 3 4 1(Work)
Item1–0to10 0.92 0.86
Item2–Pain 0.69 0.74
Item3–Pain 0.55 0.67
Item4–Pain 0.97 0.85
Item5–Pain 0.83 0.86
Item6–AD 0.43 0.63
Item7–AD 0.81 0.68
Item8–AD 0.70 0.74
Item9–AD 0.90 0.79
Item10–AD 0.55 0.68
Item11–AD 0.85 0.74
Item12–ARE 0.91 0.80
Item13–ARE 0.81 0.73
Item14–ARE 0.86 0.71
Item16–Work 0.88 0.78
Item17–Work 0.91 0.83
Item18–Work 0.89 0.80
Item19–Work 0.89 0.80
SampleSize 102 102 102 102 46
Eigenvalues 5.99 2.21 1.29 1.01 3.21
%ofvarianceexplained 42.76 15.75 9.19 7.15 80.17
KMO(1thsub-sample)=0.81. KMO(2ndsub-sample)=0.79.
Bartlett’sTest=2=490.25;p<0.001inthefirstsub-sample.
Table5–Internalconsistencyofscalesandifanyitemremoved.
Itens Valuesofalphaiftheitemisremoved
1 2 3 1(Work) Total Total(Work)
Item1–0a10 0.89 0.92
Item2–Pain 0.77 0.77 0.87
Item3–Pain 0.79 0.77 0.88
Item4–Pain 0.80 0.79 0.88
Item5–Pain 0.72 0.77 0.86
Item6–AD 0.86 0.77 0.88
Item7–AD 0.85 0.78 0.88
Item8–AD 0.84 0.77 0.88
Item9–AD 0.83 0.77 0.88
Item10–AD 0.87 0.77 0.88
Item11–AD 0.85 0.77 0.88
Item12–ARE 0.73 0.77 0.88
Item13–ARE 0.80 0.78 0.88
Item14–ARE 0.80 0.78 0.88
Item16–Work 0.90 0.87
Item17–Work 0.88 0.87
Item18–Work 0.89 0.87
Item19–Work 0,89 0,88
AlphaofCronbachofscales 0,87 0,82 0,84 0,92 0,79 0,89
SampleSize 102 102 102 46 102 46
and/or functional status ofthe upper limb.Many of these questionnairesare appliedinspecific situations and disor-dersoftheshoulder,andforoverallevaluationoftheupper limb.18–20
ThesemanticvalidationandcontentoftheBrazilianSRQ was obtainedand revealed only a few adjustmentsin the areas of pain, daily activities and in sports and leisure. TheauthorsoftheDutchversionoftheSRQalsomadesome adjustmentsinsomeareas.21However,itdrawsattentionto
theareaofsportsandleisure,whichhaschanged,and sug-gestspossibledifferencesbetweentheAmerican,European andBrazilianculturewhenitcomestosportsandleisure.
In the first item of the semantic analysis, a numerical scalesuggestedbyclinicalexpertswasused,basedon stud-iesshowingthatthistypeofscalewaseasiertocompleteand evaluate.22Thismethodofpresentingthenumbershasshown
thatpatientstendtoremembertofillinthenumbers. StudiesconductedintheoriginallanguageoftheSRQhad internalconsistency coefficients ranging between 0.71 and 0.90,andreplicationratesthatrangedbetween0.94and0.98.23
Recently,inthecross-culturaladaptationoftheoriginalSRQ intototheDutchlanguage,theauthorsreportedlevelsof inter-nalconsistencyof0.89forthequestionnaire,andtotalvalues of0.81forthefieldofpain;0.80forthefieldofdailylife activ-ities;0.72forthefieldofsportsandleisureactivities;and0.84 forfieldwork.Theresultsofthetest-retestoftheDutch ver-sionoftheSRQanditssubscales(domains)rangedbetween 0.63and0.86.21Theseresultsareconsistentwiththeresults
oftheSRQinBrazil.
Currently,theSRQisavailableinEnglish,Dutchand Por-tuguesefrom Portugal.Duetoculturaldifferences between Brazil and Portugal, we translated the Questionnaire into Brazilian Portuguese, validated it, and establishedits psy-chometriccharacteristicsatthesametimeastheversionin PortuguesefromPortugalwasbeingvalidated.7,21,23
Whenthetwoversionsarecompared,thereareclear differ-encesbetweentheminallitems.IntheversionfromPortugal,
theitem1couldnotbeadaptedtouseanumericalscale,as itwasdoneintheBrazilianversion.Inthefieldofpain(items 2to5),dailyactivities(6to11)andsportsactivities(12to14),in theversionfromPortugal,usessomewordsthatarenotusual inBrazil,suchas“dorligeira”,whichisbesttranslatedas“dor leve”(lightpain)inBrazilianPortuguese.Intheitem15, sub-item“g”,theterm“reformado”isbesttranslatedintoBrazilian Portugueseas“aposentado”(retired).
Inthepresentstudy,anevaluationofthecorrespondence between theresultsofthe BrazilianSRQ andanother vali-datedinstrument(ASES),therewasasignificantassociation betweenthetotalscoresoftheinstrumentsandthoseofall theSRQdomainswiththeoverallASESscores.Theseresults aresimilartootherstudiesusingASES.24–28
Asregards the leveloftest-retest reliability,the present study showedhigh associationofthe firstwiththe second application(ICC=0.83).Whencomparedwithothershoulder assessmentinstruments,theSRQhadoneofthehighestlevels oftest-retestreliability.18
Painisanimportantparameterthathasbeenaddressed
by several shoulder scales and measured by various
methods.15–18,28Manyshoulderscalesincludeonlyonepain
question, whichisgenerally notspecificto activityor arm position. The SRQ has a field with four questions related to pain, which assesses pain in different situations. The pain subscale of the SRQ demonstrated excellent reliabil-ity.
Conclusion
Afteranalyzingallthedata,itcanbesaidthattheBrazilian versionofSRQhaspsychometricpropertiesthatallowforits useinfunctionalevaluationoftheshoulder.Inaddition,the questionnairewasclassifiedaseasytounderstandanduse, whichreinforcesitssuitability.
Conflicts
of
interest
Theauthorsdeclarethatthisworkisnotassociatedwithany financialnorotherrelationshipswhichmightleadtoconflict ofinterest.
Appendix
1.
SHOULDER
RATING
QUESTIONNAIRE
Porfavor,respondaàsseguintesquestõesarespeitodo ombroparaoqualvocêtemsidoavaliadooutratado. Se uma questãonão for aplicada a você,deixe-a em branco.
Se você indicou que ambos os ombros foram avali-ados ou tratados, por favor, complete um ques-tionárioseparado paracada ombro e marque o lado correspondente(esquerdooudireito)napartesuperior decadaquestionário.
Qualéoseubrac¸odominante? ()esquerdo()direito
Porqualombrovocêfoiavaliadooutratado? ()direito()esquerdo()ambos
1 Considerandotodasasmaneirasqueseuombrolheafeta, marqueumXsobreaescalaabaixoparasabercomovocê estásesentindo.
Muitobem0 1 2 3 4 5 6 7 8 9 10Muitomal Asquestõesseguintesreferem-seàdor.
2 Duranteomêspassado,comovocêdescreveriaasuador doombroemrepouso?
a) Muitointensa b) Intensa c) Moderada d) Leve e) Nenhuma
3 Duranteomêspassadocomovocêdescreveriaadorusual emseuombroduranteasatividades?
a) Muitointensa b) Intensa c) Moderada d) Leve e) Nenhuma
4 Duranteomêspassado,comquefrequênciaadoremseu ombrodificultouseusonoanoite?
a) Todososdias
b) Váriosdiasporsemana c) Umdiaporsemana
d) Menosdeumdiaporsemana e) Nunca
5 Durante o mêspassado, com que frequênciavocê teve doresfortesemseuombro?
a) Todososdias
b) Váriosdiasporsemana c) Umdiaporsemana
d) Menosdeumdiaporsemana e) Nunca
Asquestõesseguintesreferem-seàsatividadesdiárias. 6 Considerandotodasasformasquevocêusaoseuombro
duranteassuasatividadesdiáriaspessoaisedomésticas (p.ex.sevestir,tomarbanho,dirigir,astarefasdomésticas etc.),comovocêdescreveriaasuahabilidadeemutilizar seuombro?
a) Limitac¸ãomuitosevera;incapaz b) Limitac¸ãosevera
c) Limitac¸ãomoderada d) Limitac¸ãoleve e) Semlimitac¸ão
Questões7-11–Duranteomêspassado,quanta dificul-dade você teve em cada umadas seguintes atividades devidoaoseuombro?
7 Colocaroutirarumcasacooucamisa. a) Incapaz
b) Dificuldadesevera c) Dificuldademoderada d) Levedificuldade e) Semdificuldade
8 Pentearouescovarseucabelo. a) Incapaz
b) Dificuldadesevera c) Dificuldademoderada d) Levedificuldade e) Semdificuldade
9 Alcanc¸arprateleirasqueestãoacimadesuacabec¸a. a) Incapaz
b) Dificuldadesevera c) Dificuldademoderada d) Levedificuldade e) Semdificuldade
10 Coc¸arelavaraparteinferiordesuascostascomsuamão. a) Incapaz
b) Dificuldadesevera c) Dificuldademoderada d) Levedificuldade e) Semdificuldade
11 Levantaroucarregar umasacolacheiademantimentos (cincoquilos).
a) Incapaz
b) Dificuldadesevera c) Dificuldademoderada d) Levedificuldade e) Semdificuldade
Asseguintesquestõesreferem-seàsatividadesesportivas oudelazer.
a) Limitac¸ãomuitosevera;incapaz b) Limitac¸ãosevera
c) Limitac¸ãomoderada d) Limitac¸ãoleve e) Semlimitac¸ão
13 Duranteomêspassado,quantadificuldadevocêteveem arremessarumabolacom amãooualgum movimento parecidocomarremessodevidoaoseuombro?
a) Incapaz
b) Dificuldadesevera c) Dificuldademoderada d) Levedificuldade e) Semdificuldade
14 Escrevaumaatividade(esportivaoudelazer)quevocê par-ticularmentegostaeentãoselecioneograudelimitac¸ão quevocêtem,sealguma,devidoaoseuombro.
a) Atividade b) Incapaz
c) Limitac¸ãosevera d) Limitac¸ãomoderada e) Limitac¸ãoleve
f) Semlimitac¸ão
Asquestõesseguintesreferem-seaotrabalho.
15 Duranteomêspassado,qualfoiasuaprincipalformade trabalho?
a) Trabalho remunerado (liste o tipo de trabalho)
b) Trabalhoemcasa c) Trabalhoescolar d) Desempregado
e) Incapacitadodevidoaoseuombro
f) Incapacitadosecundariamenteaoutrascausas g) Aposentado
Sevocêrespondeud,e,f,ougnaperguntaacima,porfavor, puleasquestões16,17,18e19eváparaaquestão20. 16 Duranteomêspassado,com quefrequênciavocêficou
incapazdefazeralgumacoisadoseutrabalhohabitualpor causadoseuombro?
a) Todososdias
b) Váriosdiasporsemana c) Umdiaporsemana
d) Menosdeumdiaporsemana e) Nunca
17 Duranteomêspassado,nodiaemquevocêrealmente tra-balhou,comquefrequênciavocêficouincapazdefazerseu trabalhotão cuidadosamente oueficientemente quanto vocêgostariaporcausadoseuombro?
a) Todososdias
b) Váriosdiasporsemana c) Umdiaporsemana
d) Menosdeumdiaporsemana e) Nunca
18 Duranteomêspassado,nosdiasemquevocêrealmente trabalhou,com qualfrequênciavocêteveque trabalhar menoshorasdoqueonormalporcausadoseuombro? a) Todososdias
b) Váriosdiasporsemana c) Umdiaporsemana
d) Menosdeumdiaporsemana e) Nunca
19 Duranteomêspassado,nosdiasemquevocêrealmente trabalhou, com qualfrequência vocêteve que mudara formacomoseutrabalhohabitualéfeitoporcausadoseu ombro?
a) Todososdias
b) Váriosdiasporsemana c) Umdiaporsemana
d) Menosdeumdiaporsemana e) Nunca
Asquestõesseguintesreferem-seasatisfac¸ãoeáreasde melhoria.
20 Durante o mês passado, como você avaliaria seu grau médiodesatisfac¸ãocomseuombro?
a) Ruim b) Razoável c) Bom d) Muitobom e) Excelente
21 Por favor,marque abaixoduas áreas em quevocê mais gostariadeveramelhora(coloqueonúmero1paraomais importanteeonúmero2paraosegundomaisimportante).
a) Melhoradador
b) Melhora pararealizar asatividadesdiáriaspessoaiseas atividadesdecasa
c) Melhorapararealizarasatividadesesportivasoudelazer
d) Melhorapararealizarasatividadesdotrabalho
Muitoobrigadopelasuacooperac¸ão!
r
e
f
e
r
e
n
c
e
s
1.KnautLA,MoserADL,MeloSA,RichardsRR.Traduc¸ãoe adaptac¸ãoculturalàlínguaportuguesadoAmerican ShoulderandElbowSurgeonsStandardizedShoulder AssessmentForm(ASES)paraavaliac¸ãodafunc¸ãodoombro. RevBrasReumatol.2010;50:176–83.
2.Mendonc¸aJuniorH,Assunc¸ãoA.Associac¸ãoentredistúrbios doombroetrabalho:breverevisãodeliteratura.RevBras Epidemiol.2005;8:167–76.
3.GrootenWJ,MulderM,JosephsonM,AlfredssonL,Wiktorin C.Theinfluenceofwork-relatedexposuresontheprognosis ofneck/shoulderpain.EurSpineJ.2007;16:2083–91.
4.HooftmanWE,WestermanMJ,VanderBeekAJ,BongersPM, VanMechelenW.Whatmakesmenandwomenwith musculoskeletalcomplaintsdecidetheyaretoosicktowork? ScandJWorkEnvironHealth.2008;34:107–12.
5.LopesAD,StadnikySP,MasieroD,CarreraEF,CiconelliRM, GriffinS.Traduc¸ãoeadaptac¸ãoculturaldoWORC:um questionáriodequalidadedevidaparaalterac¸õesdo manguitorotador.RevBrasFisioter.2006;10: 309–15.
6.PugaO,LopesD,CostaP.Avaliac¸ãodasadaptac¸ões transculturaisepropriedadesdemedidadequestionários relacionadosàsdisfunc¸õesdoombroemlínguaportuguesa: umarevisãosistemática.RevBrasFisioter.2012;16:85–93.
Disponívelem:http://www.ifisionline.ips.pt/media/2jan vol1n2/pdfs/artigo1voln2.pdf.[Acessoem8junho2013].
8. MeadowsK,BentzenN,Touw-OttenF.Cross-culturalissues: anoutlineoftheimportantprinciplesinestablishing cross-culturalvalidityinhealthoutcomeassessment.In: HutchinsonA,BentzenN,König-ZahnC,editors.Cross culturalhealthoutcomeassessment;auser’sguide. Germany:ERGHO;1997.p.34–40,1.
9. FerreiraP,MarquesF.Avaliac¸ãoPsicométricaeAdaptac¸ão CulturaleLinguísticadeInstrumentosdeMedic¸ãoemSaúde: PrincípiosMetodológicosGerais.Coimbra:CentrodeEstudos eInvestigac¸ãoemSaúdedaUniversidadedeCoimbra.;1998.
10.SilvaM.Medidasderesultados(OutcomeMeasures). Essfisioonline.2005;2:59–75.
11.PasqualiL.Análisefatorialparapesquisadores.Brasília: LabPAM-IP-DF;2001.
12.HillMM,HillA.Investigac¸ãoporquestionário.Lisboa:Silabo; 2000.
13.SampaioRF,ManciniMC,FonsecaST.Atuac¸ãoProfissional: aspectosquelimitamessaintegrac¸ãonaFisioterapiaena TerapiaOcupacional.RevBrasFisioter.2002;6:113–8.
14.RundquistPJ,LudewingPM.Correlationof3-dimensional shoulderkinematicstofunctioninsubjectswithidiopathic lossofshoulderrangeofmotion.PhysTher.2005;85: 636–47.
15.PaulA,LewisM,ShadforthMF,CroftPR,VanDerWindt DAWM,HayEM.Acomparisonoffourshoulder-specific questionnairesinprimarycare.AnnRheumDis. 2004;63:1293–9.
16.VermeulenHM,RozingPM,ObermannWR,CessieS,Vlieland TPV.Comparisonofhigh-gradeandlow-grademobilization techniquesinthemanagementofadhesivecapsulitisofthe shoulder:randomizedcontrolledtrial.PhysTher.
2006;86:355–68.
17.NawoczenskiDA,Ritter-SoronenJM,WilsonCM,HoweBA, LudewigPM.Clinicaltrialofexerciseforshoulderpainin chronicspinalinjury.PhysTher.2006;86:1604–18.
18.LegginBG,MichenerLA,ShafferMA,BrennemanSK,Lannotti JP,WilliamsRG.ThePennshoulderscore:reliabilityand validity.JOrthopSportsPhysTher.2006;36:138–51.
19.MoserADM,KnautLAM,ZotzTG,ScharanKO.Validadee confiabilidadedaversãoemportuguêsdoAmericanShoulder andElbowSurgeonsStandardizedShoulderAssessment Form.RevBrasReumatol.2012;52:348–56.
20.PugaVO,LopesAD,ShiwaSR,AloucheSR,CostaLO. Clinimetrictestingsupportstheuseof5questionnaires adaptedintoBrazilianPortugueseforpatientswithshoulder disorders.JOrthopSportsPhysTher.2013;43:404–13.
21.VermeulenHM,BoonmanDC,SchüllerHM,ObermannWR, VanHouwelingenHC,RozingPM,etal.Translation, adaptationandvalidationoftheShoulderRating
Questionnaire(SRQ)intotheDutchlanguage.ClinRehabil. 2005;19:300–11.
22.ChanquesG,VielE,ConstantinJM,JungB,deLattreS,CarrJ, etal.Themeasurementofpaininintensivecareunit: comparisonof5self–reportintensityscales.International AssociationfortheStudyofPain.2010;151:711–21.
23.L’InsalataJC,WarrenRF,CohenSB,AltchekDW,PetersonMG. Aself-administeredquestionnaireforassessmentof symptomsandfunctionoftheshoulder.JBoneJointSurgAm. 1997;79:738–48.
24.LopesAD,CiconelliRM,DosReisFB.Medidasdeavaliac¸ãode qualidadedevidaeestadodesaúdeemortopedia.RevBras Ortop.2007;42:355–9.
25.LopesAD,CiconelliRM,CarreraEF,GriffinS,FaloppaF,Dos ReisFB.ValidityandreliabilityoftheWesternOntarioRotator CuffIndex(WORC)foruseinBrazil.ClinJSportMed. 2008;18:266–72.
26.LemeL,SaccolM,BarbosaG,EjnismanB,FaloppaF,CohenM. Validac¸ão,reprodutibilidade,traduc¸ãoeadaptac¸ãocultural daescalaAthleticShoulderOutcomeRatingScaleparaa línguaportuguesa.RevBrasMed.2010;67:29–38.
27.ChengHM,SampaioRF,ManciniMC,FonsecaST,CottaRM. Disabilitiesofthearm,shoulderandhand(DASH):factor analysisoftheversionadaptedtoPortuguese/Brazil.Disabil Rehabil.2008;30:1901–9.