REVISTA
BRASILEIRA
DE
REUMATOLOGIA
ww w . r e u m a t o l o g i a . c o m . b r
Brief
communication
Characterization
of
the
pain,
sleep
and
alexithymia
patterns
of
patients
with
fibromyalgia
treated
in
a
Brazilian
tertiary
center
Lazslo
A.
Avila,
Gerardo
M.
de
Araujo
Filho
∗,
Estefano
F.U.
Guimarães,
Lauro
C.S.
Gonc¸alves,
Paola
N.
Paschoalin,
Fabia
B.
Aleixo
DepartmentofPsychiatryandMedicalPsychology,FaculdadedeMedicinadeSãoJosédoRioPreto,SãoJosédoRioPreto,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20December2013 Accepted26March2014
Keywords:
Fibromyalgia Sleepcomplaints Qualityoflife Alexithymia
PittsburghSleepQualityIndex TorontoAlexithymiaScale
a
b
s
t
r
a
c
t
Objectives: Fibromyalgia(FM)isacomplexsyndromethatischaracterizedbylastingand diffusechronicmusculoskeletalpain,derivedfromnon-inflammatorycausesandclassically associatedwiththepresenceofspecifictenderpoints.However,studieshavehighlighted other importantsymptomsassociatedwitha lowerqualityoflife(QOL) inFM,suchas sleepdisturbancesandalexithymia.Thisstudyaimedtoinvestigatethepain,sleepand alexithymiapatternsofFMpatientstreatedinaBraziliantertiarycenter.
Methods:20patientswithFMwhowerefollowed-upintheRheumatologyoutpatientclinic ofaBraziliantertiarycenter(FaculdadedeMedicinadeSãoJosédoRioPreto–FAMERP, SãoPaulo,Brazil)and20patientswithoutFMfromotheroutpatientservicesoftheFAMERP completedaclinicalandsocio-demographicquestionnaire,theFibromyalgiaImpact Ques-tionnaire(FIQ),thePittsburghSleepQualityIndex(PSQI),theTorontoAlexithymiaScale (TAS-20)andtheSF-36(WHOQOL).
Results:ThepatientswithFMpresentedworseperformancesinallQOLdimensionsofthe SF-36andhigherscoresonthePSQI(p=0.01),andtheTAS-20(p=0.02).PatientswithFM alsoscoredsignificantlyhigherinallspecificdomainsofPSQIandTAS-20.
Discussion: Thepresentdatawereinaccordancewithliterature,disclosingaworse per-formance ofpatients withFMon pain impact,sleepcomplains andmorepresence of alexithymia.
Conclusion: Studieshavedisclosedthe presenceofimportantandfrequently underdiag-nosedsymptomsbeyondpaincomplaintsinFM,suchassleepcomplaintsandalexithymia, andabetterknowledgeofsuchdisturbancesmightimproveFMpatients’approachand treatment.
©2014ElsevierEditoraLtda.Allrightsreserved.
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rbr.2014.03.017.
∗ Correspondingauthor.
E-mail:[email protected](G.M.deAraujoFilho).
http://dx.doi.org/10.1016/j.rbre.2014.03.017
Caracterizac¸ão
dos
padrões
de
dor,
sono
e
alexitimia
em
pacientes
com
fibromialgia
atendidos
em
um
centro
terciário
brasileiro
Palavras-chave:
Fibromialgia Queixasdesono Qualidadedevida Alexitimia
PittsburghSleepQualityIndex TorontoAlexithymiaScale
r
e
s
u
m
o
Objetivos: Fibromialgia(FM)éumasíndromecomplexa,caracterizadaporumador mus-culoesquelética crônica duradoura e difusa, derivada de causas não inflamatórias e classicamenteassociadaàpresenc¸adepontossensíveisespecíficos.Noentanto,estudos destacaramoutros sintomasimportantesassociados àmáqualidadedevida (QDV)em pacientescomFM,porexemplo,distúrbiosdosonoealexitimia.Esseestudotevepor obje-tivoinvestigarospadrõesdedor,sonoealexitimiadepacientescomFMemumcentro terciáriobrasileiro.
Métodos: 20pacientescomFMacompanhadosnaclínicaambulatorialdereumatologiade umcentroterciáriobrasileiro(FaculdadedeMedicinadeSãoJosédoRioPreto–FAMERP, SãoPaulo,Brasil)e20pacientessemFMprovenientesdeoutrosservic¸osambulatoriaisda FAMERPcompletaramumquestionárioclínicoesociodemográfico,oFibromyalgiaImpact Questionnaire(FIQ),oPittsburghSleepQualityIndex(PSQI),oTorontoAlexithymiaScale(TAS-20) eoSF-36(WHOQOL).
Resultados: OspacientescomFMtiveramdesempenhospioresemtodasasdimensõesde QDVdoSF-36eescoresmaisaltosnoPSQI(P=0,01)enoTAS-20(P=0,02).PacientescomFM tambémtiveramescoressignificativamentemaisaltosemtodososdomíniosespecíficosdo PSQIeTAS-20.
Discussão: Ospresentesdadosconcordavamcomaliteratura,evidenciandopior desem-penhode pacientescomFMno impactoda dor,queixasdesono emaiorpresenc¸a de alexitimia.
Conclusão: Estudosevidenciaram,alémdasqueixasdedor,apresenc¸adesintomas impor-tantesefrequentementesubdiagnosticados,empacientescomFM,comoqueixasrelativas aosonoealexitimia.Umconhecimentomaisaprofundadodessesdistúrbiospoderia mel-horaraabordagemeotratamentodospacientescomFM.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Fibromyalgia (FM) is a complex syndrome that is charac-terizedbylastinganddiffusechronicmusculoskeletalpain, derivedfromnon-inflammatorycausesandclassically asso-ciatedwiththepresenceofspecifictenderpoints.1–5Itisthe
secondmostcommonrheumatologicdisease,witha world-wideprevalenceof0.5%to5%.Womenagedbetween40and55 yearsarepredominantlyaffected,withaprevalence approx-imatelysevenfoldhigherthaninmen.1,4,5Thediagnosisof
FMremainsessentiallyclinical,althoughtheaidofsubsidiary examscanbeusefulforassociateddiagnosis.5–7
Recentstudies havehighlighted other important symp-tomsassociatedwithalowerqualityoflife(QOL)inFM,suchas sleepdisturbancesandalexithymia.8–10Themajorsleep
com-plaintsreportedbypatientsincludeinsomnia,feelingtired uponwaking,decreasedsleeptimeandanincreasednumber ofsleepinterruptionspernight.Inaddition,thehigh preva-lence of sleep disorders in patients with FMimpairs their QOLintwo ways:difficulty obtainingrestorativesleep and increasedsleepinessduringtheday,characterizedbydifficulty maintainingwakefulness.8–10
Inaccordance withthe definitionprovided byCampbell (1996),“alexithymia”ischaracterizedbydifficultyidentifying one’sownemotionalstate,withtheinabilitytofocuson exter-nalandsomaticinterestsandtoproductivelyfantasize.11–15
StudieshavereportedthatFMpatientshaveaspecific diffi-cultyinrecognizingtheirownemotionsinassociationwith more complaints of increasedpain, fatigue and decreased physical function.14–16 In addition to alexithymia, patients
exhibit “sensoryamplification”,which consistsofa greater sensitivity andresponsiveness todifferentsensory stimuli, including pain.17 Based on these definitions and previous
studiesofFM,thepresentstudyaimedtoinvestigate,inamore detailedmanner,thepain,sleepandalexithymiapatternsof FMpatientstreatedinaBraziliantertiarycenter.
Patients
and
methods
Participants
Table1–Demographicdataofpatientswithfibromyalgiaandacontrolgroup.
Demographicdata FM CG P
Numberofsubjects 20 20
-Ageinyears(mean±SD) 32.7±9.1 32.2±7.1 0.82
Numberoffemales(%) 19(95) 18(90) 0.85
Yearsofschooling(mean±SD) 9.2±6.3 12.8±5.1 0.12
CG,controlgroup;FM,fibromyalgiagroup;SD,standarddeviation.
olderthan65years,thosewithpainsyndromesnotdiagnosed asFMandwithanyotherrheumatologicdiseaseinadditionto FMwereexcluded.Thestudysampleincluded40individuals dividedintotwogroups:20patientswithFM(patientgroup –PG)and20 patientsfromother outpatientservices ofthe FAMERP(controlgroup–CG).Thesegroupswerecreated to includepatientsexposedtosimilarlevelsofhospitalstressin bothgroups,eliminatingthispossiblebias.
Procedures
A clinical and socio-demographic questionnaire including age, gender, schooling,psychiatricfamily history and drug treatment was administered. The FM patients were then administeredspecificquestionnaires:
a) FibromyalgiaImpactQuestionnaire(FIQ)–toanalyzespecific aspectsofthepaincomplaints.Thisinstrument hasten domains(functionalcapacity,well-being,workabsences, abilitytowork,pain,fatigue,sleep,morningstiffness, anx-ietyanddepression),andthegeneralscorecanrangefrom 0to80.Patientswithhigherpainimpactpresenthigher scores;
b) Pittsburgh SleepQuality Index (PSQI)– to analyze aspects associatedwithsleep.Thisinstrumenthassevendomains (subjective sleep quality, sleep latency, sleep duration, habitualsleep efficiency,sleepdisorders,useof medica-tionsforsleepanddaytimedysfunction).Themaximum totalscoreis21points,andthehigherthevalue,thelower thequalityofsleepevidenced.Totalscoresgreaterthan5 areindicativeofpoorsleepquality;
c) TorontoAlexithymiaScale(TAS-20)–toassessthepresenceof symptomsassociatedwithalexithymia.Thisinstrument examinesthreemaindomains:abilitytoidentifyand to describefeelings,andtodistinguishfeelingsofbodily sen-sations,abilitytodaydreamandpreferenceforfocusingon externaleventsratherthaninnerexperiences.Thescore indicatedbytheinstrumentrangesfrom26to130.Values lowerthan62donotindicatesymptomsofalexithymia, andvalueshigherthan74indicatethepresenceofthese symptoms.Valuesbetween63and73areinconclusive; d) The SF-36 (WHOQOL) – to analyze the QOL in eight
domains:functional,limitationsduetophysicalaspects, bodily pain, general health, vitality, social functioning, emotionalhealthandmentalhealth.Thelowerthescore is,theworsetheQOL.
Statistics
Demographic data are presented as the mean±standard deviation.Age and gender matchingbetweenpatients and
controlswereevaluatedusingthetwoindependentsamples t-testandFisher’sexacttest,respectively.Datafromthe ques-tionnaireswereanalyzedusingnonparametrictests(unpaired t-test, Mann-Whitney Test and Spearmancorrelation). The statisticalsignificancelevelwassetat5%.
Results
Thirty-sevenfemales (19from the PG and18 from theCG) and three males (one from the PG and two from the CG) were enrolled in the study. Groups were matched by gen-der (p=0.85), age (p=0.82) and years ofschooling (p=0.12) (Table1).
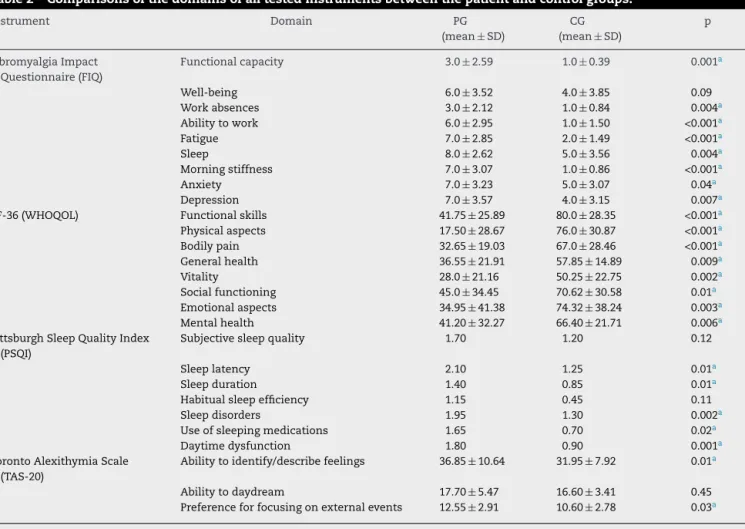
RegardingtheimpactofFMasassessedbytheFIQ,there weresignificantdifferencesbetweenthePGandtheCG.The meangeneralscorewas52.0±13.54forthePGand26.0±16.06 fortheCG(p<0.0001).HigherscoreswereobservedinthePGin all10domains.TheSF-36alsoshowedsignificantdifferences between both groups, with the PG presenting significantly lower meanscoresinall eightdomainscomparedwiththe CG.RegardingthesleepaspectsassessedbythePSQI,there wasasignificantdifferencebetweenthetotalscoresofthe CG (6.65±4.46) and the PG (11.65±4.48) (p=0.01). The PG scoredhigherinallsevendomainsofthePSQI.Regardingthe symptomsofalexithymiaassessedbytheTAS-20,themean totalscorewas67.10±9.34forthePGand59.15±8.70forthe CG (p=0.03). Comparisonsbetween thetwo groupsfor the domainsofalloftheinstrumentsareshowninTable2.
Discussion
FMisacomplexdiseasewithasignificantprevalenceamong the general population and ischaracterized bycomplaints of pain that are often underdiagnosed. Moreover, the cur-rent literaturehighlights the existence of other important and underdiagnosedsymptoms, suchassleepdisturbances andalexithymia,whichcouldbeassociatedwithlowerQOL among patients with FM. Thus, the investigation of these aspectsandthesearchfortoolstoassesssuchcomplaintsare necessary.6–18
Inthepresentstudy,theFIQdifferentiatedtheimpactof painbetweenthePGandtheCG,disclosingahigherimpact inthe PG comparedtotheCGinall 10fields,asoriginally expected.Otherstudieshaveconfirmedthisfinding,reporting impairmentsofthesameskillsinpatientswithFM.6–10,18,19In
Table2–Comparisonsofthedomainsofalltestedinstrumentsbetweenthepatientandcontrolgroups.
Instrument Domain PG
(mean±SD)
CG (mean±SD)
p
FibromyalgiaImpact Questionnaire(FIQ)
Functionalcapacity 3.0±2.59 1.0±0.39 0.001a
Well-being 6.0±3.52 4.0±3.85 0.09
Workabsences 3.0±2.12 1.0±0.84 0.004a
Abilitytowork 6.0±2.95 1.0±1.50 <0.001a
Fatigue 7.0±2.85 2.0±1.49 <0.001a
Sleep 8.0±2.62 5.0±3.56 0.004a
Morningstiffness 7.0±3.07 1.0±0.86 <0.001a
Anxiety 7.0±3.23 5.0±3.07 0.04a
Depression 7.0±3.57 4.0±3.15 0.007a
SF-36(WHOQOL) Functionalskills 41.75±25.89 80.0±28.35 <0.001a
Physicalaspects 17.50±28.67 76.0±30.87 <0.001a
Bodilypain 32.65±19.03 67.0±28.46 <0.001a
Generalhealth 36.55±21.91 57.85±14.89 0.009a
Vitality 28.0±21.16 50.25±22.75 0.002a
Socialfunctioning 45.0±34.45 70.62±30.58 0.01a
Emotionalaspects 34.95±41.38 74.32±38.24 0.003a
Mentalhealth 41.20±32.27 66.40±21.71 0.006a
PittsburghSleepQualityIndex (PSQI)
Subjectivesleepquality 1.70 1.20 0.12
Sleeplatency 2.10 1.25 0.01a
Sleepduration 1.40 0.85 0.01a
Habitualsleepefficiency 1.15 0.45 0.11
Sleepdisorders 1.95 1.30 0.002a
Useofsleepingmedications 1.65 0.70 0.02a
Daytimedysfunction 1.80 0.90 0.001a
TorontoAlexithymiaScale (TAS-20)
Abilitytoidentify/describefeelings 36.85±10.64 31.95±7.92 0.01a
Abilitytodaydream 17.70±5.47 16.60±3.41 0.45 Preferenceforfocusingonexternalevents 12.55±2.91 10.60±2.78 0.03a
CG,controlgroup;PG,patientgroup;SD,standarddeviation.
a p<0.05.
impactofFMonpatients, reducingtheirQOLandaffecting boththeirphysicalandmentalhealth.6,8,18–21
TheresultsofthePSQIdemonstratedmorefrequentsleep complaints among patients with FM. These results are in accordancewiththemostrecentlypublishedstudies,which havehighlightedtheimportanceofsleepdisordersinthe clin-icalconditionandintheQOLofpatientswithFM.15–18,22,23
Amongtheaspects studied,the domain “using medica-tionstosleep”suggeststhatFMpatientsrelyonmedicationsto aidsleepanddonotreach“habitualsleepefficiency”or “sub-jectivesleep quality”.In addition,thedomains of“daytime dysfunction”and“sleepamendment”suggestthepersistence ofnon-restorativesleep,resultinginaconsiderabledeficitin theabilitytoperformdailyactivities.15–18,22,23However,even
withsignificantdifferencesinscoresbetweenthePGandthe CGonthePSQI,bothgroupsshowedlowsleepquality(scores above5).Thisfindingcanbeexplainedbythestresscaused bybothdiseaseandtreatmentinatertiarycenter,towhich thetwogroupswereexposedatthetimeofthestudy.Other studieshavealsoobservedsucheffectswhenpatientswithFM werecomparedwithpatientswithotherchronicanddisabling disorders,suchasrheumatoidarthritisanddepression.20,21
Regarding the presenceof alexithymia symptoms mea-suredusing the TAS, the PG presentedsignificantlyhigher scoresthantheCG.However,bothgroupsscoredverycloseto
theaverage,withvaluesadjacenttothe“inconclusive inter-val”oftheinstrument.Thisfindingcouldbeaconsequence ofthesmallnumberofparticipants,whichisanimportant limitationofthisstudy.15,23,24LaneandSechrest(1998)
admin-isteredtheTAS-20to380individualsstratifiedbyage,gender, socioeconomicstatusandyearsofeducation,andtheyalso observedthatthisinstrumenthadatendencytoreportworse results for patients with advanced age, male gender, low socioeconomicstatusandfeweryearsofeducation.23
There-fore,onecaninferthatthepresentresultsarealsoaffectedby lowsocioeconomicstatusandfewyearsofeducation,which werepresentinbothgroups,thusnarrowingtheexpected dif-ferencebetweenthePGandtheCG.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
TheauthorsthankMr.JoseAntonioCordeiroforprovidinghelp withthestatisticalanalysis.
r
e
f
e
r
e
n
c
e
s
1. FitzcharlesMA,Ste-MariePA,GoldenbergDL,PereiraJX, AbbeyS,ChoinièreM,etal.NationalFibromyalgiaGuideline AdvisoryPanel.CanadianGuidelinesforthediagnosisand managementoffibromyalgiasyndrome:Executivesummary. PainRes&Man.2013;18:119–26.
2. HeymarnRE,PaivaES,HelfensteinJrM,PollakDF,MartinezJE, ProvenzaJR,etal.BrazilianconsensusonFibromyalgia treatment.RevBrasReumatol.2010;50:56–66.
3. CamposRP,RodriguezMIV.Health-relatedqualityoflifein womenwithfibromyalgia:clinicalandpsychologicalfactors associated.ClinRheumatol.2012;31:347–55.
4. LachaineJC,BeaucheminC,LandryPA.Clinicalandeconomic characteristicsofpatientswithfibromyalgiasyndrome.ClinJ Pain.2010;26:284–90.
5. WalittB,FitzcharlesM,HassettA,KatzR,HauserW,WolfeF. ThelongitudinalOutcomeoffibromyalgia:astudyof1555 patients.JRheumatol.2011;38:2238–46.
6. RiveraJ,Rejas-GutierrezJ,VallejoMA,Esteve-VivesJ,De Salas-CansadoM.Prospectivestudyoftheuseofhealthcare resourcesandeconomiccostsinpatientswithfibromyalgia aftertreatmentinroutinemedicalpractice.ClinExperim Rheumatol.2012;30:S31–8.
7. HamiltonNA,AtchleyRA,KarlsonCW,TaylorD,McCurdyD. TheRoleofSleepandAttentionintheEtiologyand MaintenanceofFibromyalgia.CognTherapyRes. 2012;36:81–93.
8. WagnerJS,DiBonaventuraMD,ChandranAB,CappelleriJC. Theasssociationofsleepdifficultieswithhealth-related qualityoflifeamongpatientswithfibromyalgia.BMCMusc Dis.2012;13:199.
9. ConsoliG,MarazzitiD,CiapparelliA,BazzichiL,Massimetti G,GiacomelliC,etal.Theimpactofmood,anxiety,andsleep disorderesonfibromyalgia.ComprPsychiatry.2012;53:962–7.
10.MartinsMRI,PolveroL,RochaCE,FossMH,DosSantosJrR. Usodequestionáriosparaavaliaramultidimensionalidadee
aqualidadedevidadofibromiálgico.RevBrasReumatol. 2012;52:21–6.
11.ChoyE,PerrotS,LeonT,KaplanJ,PeterselD,GinovkerA, etal.Apatientsurveyoftheimpactoffibromyalgiaand thejourneytodiagnosis.BMCHealthServRes.2010; 10:102.
12.MartinezJE.Fibromyalgia:thepitfallofthecorrectdiagnosis. RevBrasReumatol.2006;46:2.
13.BerberJSS,KupekE,BerberSC.Prevalenceofdepressionand itsassociationwithFibromyalgia.RevBrasReumatol. 2005;45:47–54.
14.WolfeF,SmytheHA,YunusMB,BennettRM,BombardierC, GoldenbergDL,etal.TheAmericanCollegeofRheumatology 1990CriteriafortheClassificationofFibromyalgia:Reportof theMulticenterCriteriaCommittee.ArthritisRheum. 1990;33:160–72.
15.SobrinhoDGR,RoinzenblattS,LopesAC,TeixeiraRCA,Tufik S.Estudodacapacidadedemanteroalertaempacientescom fibromialgiapormeiodotestedamanutenc¸ãodavigília.Rev BrasReumatol.2008;48:12–6.
16.JacominiLCL,daSilvaNA.Disauthonomy:naemerging conceptinfibromyalgia.RevBrasReumatol.2007;47:354–61.
17.SusanM,ChandranA,ZografosL,ZlatevaG.Evaluationsof theimpactoffribromyalgiaonpatients’sleepandthe contentvalidityoftwosleepscales.HealthQualLife Outcomes.2009;7:64.
18.GeisserME,StraderDonellC,GracelyRH,ClawDJ,Williams DA.Comorbidsomaticsymptomsandfunctionalstatusin patientswithfibromyalgiaandchronicfatiguesyndrome: sensoryamplificationasacommonmechanism. Psychosomatics.2008;49:235–42.
19.YoshikawaGT,HeymanRE,HelfensteinMJr,PollackDF.A Comparisonofqualityoflife,demographicandclinical characteristicsofBrazilianmenwithfibromyalgiasyndrome withmalepatientswithdepression.RheumatolInt. 2010;30:473–8.
20.TanderB,CengizK,AlayliG,IlhanlyI,CanbazS,CanturkF.A comparativeevaluationofhealthrelatedqualityoflifeand depressioninpatientswithfibromyalgiasyndromeand rheumatoidarthritis.ReumatolInt.2008;28:859–65.
21.LeiteACS,SalesNC,OliveiraRM.Evidênciasdealterac¸õesno padrãodesonoemmulherescomfibromialgia.Nursing(São Paulo).2009;12:166–70.
22.BigattiSM,HernandezAM,CronanTA,RandKL.Sleep disturbancesinfibromyalgiasyndrome:relationshiptopain anddepression.ArthritisRheum.2008;59:961–7.
23.LaneRD,SechrestL,RiedelR.Sociodemographiccorrelatesof alexithimya.ComprPsychiatry.1998;39:377–85.