w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Age-adjusted
international
prognostic
index
is
a
predictor
of
survival
in
gastric
diffuse
B-cell
non-Hodgkin
lymphoma
patients
Marcia
Torresan
Delamain
a,
Maria
Gomes
da
Silva
b,
Eliana
Cristina
Martins
Miranda
a,∗,
Joana
Desterro
b,
Stefano
Luminari
c,
Anna
Fedina
c,
Francesco
Merli
d,
Carlos
Sergio
Chiattone
e,
Katia
Borgia
Barbosa
Pagnano
a,
Massimo
Federico
c,
Carmino
Antonio
de
Souza
aaUniversidadedeCampinas(Unicamp),Campinas,SP,Brazil
bInstitutoPortuguêsdeOncologia,DepartamentodeHematologia,Lisboa,Portugal
cUniversitàdiModenaeReggioEmilia,ClinicaediSanitàPubblica,DepartmentofDiagnosticMedicine,Modena,Italy
dArcispedaleSantaMariaNuova–IRCCS,ReggioEmilia,Italy
eSantaCasadeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19April2016 Accepted25April2016 Availableonline18May2016
Keywords:
DiffuselargeB-celllymphoma Gastric
Prognosis
a
b
s
t
r
a
c
t
Background:Theclinicalcourseofgastriclymphomaisheterogeneousandclinical symp-tomsandsomefactorshavebeenrelatedtoprognosis.
Objective:ThepresentstudyaimstoidentifyprognosticfactorsingastricdiffuseB-cell non-Hodgkinlymphomadiagnosedandtreatedindifferentcountries.
Methods:AconsecutiveseriesofgastricdiffuseB-cellnon-Hodgkinlymphomapatients diag-nosedandtreatedinBrazil,PortugalandItaly,betweenFebruary2008andDecember2014 wasevaluated.
Results:Of104patients,57werefemaleandthemedianagewas69years(range:28–88).The distributionoftheage-adjustedinternationalprognosticindexwas12/95(13%)highrisk, 20/95(21%)high-intermediateriskand63/95(66%)low/low-intermediaterisk.Symptoms includedabdominalpain(63/74),weightloss(57/73),dysphagia(37/72)andnausea/vomiting (37/72).Bulkydiseasewasfoundin24%ofthecases,anemiain33of76patientsandbleeding in22of72patients.Themedianfollow-uptimewas25months(range:1–77months),with 1-and5-yearsurvivalratesof79%and76%,respectively.ThemultivariateCoxRegression identifiedtheage-adjustedinternationalprognosticindexasapredictorofdeath(hazard risk:3.62;95%confidenceinterval:2.21–5.93;p-value<0.0001).
Conclusions: Thisseriesidentifiedtheage-adjustedinternationalprognosticindexas pre-dictiveofmortalityinpatientstreatedwithconventionalimmunochemotherapy.
©2016Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthorat:CentrodeHematologiaeHemoterapia,UniversidadeEstadualdeCampinas(Unicamp),RuaCarlosChagas480,
CidadeUniversitária“ZeferinoVaz”,13083-878Campinas,SP,Brazil. E-mailaddress:[email protected](E.C.M.Miranda).
http://dx.doi.org/10.1016/j.bjhh.2016.04.010
Introduction
Gastriclymphomaisthemostcommonextranodaldiffuse B-cellnon-Hodgkinlymphoma(DLBCL)andaccountsfor30% ofcasesoflymphomainthestomach.1Accordingtothe
cur-rent WHO lymphomaclassificationcriteria, gastric DLBCLs areclassifiedwithorwithoutfeaturesofMALT.2Recent
stud-iesrevealedthatHelicobacterpylori-relatedgastricDLBCLisa distinctlessaggressiveentitywithgreaterchemosensitivity, therebyhighlightingtheheterogeneityoftheselymphomas. Theclinicalpresentationand courseare alsovariable with clinical symptoms, laboratorialabnormalities and H. pylori, hepatitisB,and C infections,inaddition toclassical inter-nationalprognosticindex(IPI)factorshavingbeenrelatedto prognosis.3 Differentclinical behaviorsmay reflect distinct
unidentified pathogenic mechanisms.4 A better
characteri-zationofprognosticfactorsisrequiredinordertodiscover newpotentialdiseasemechanisms, improve outcomesand individualizetreatmentapproaches.Thepresentstudyaims toidentifyprognosticfactorsinpatientswithgastricDLBCL diagnosed and treated in different countries by analyzing demographicand clinicalcharacteristics,responseto treat-mentandoutcome.
Patients
Aretrospectivestudyof104consecutivepatientswithDLBCL diagnosedandtreatedinhematologycentersinBrazil,Italy andPortugalbetweenFebruary2008andDecember2014was performed. The inclusion criteria were age >18 years old, lymphomaprimarilylocatedinthestomach,withor with-outtheinvolvementofotherintra-abdominalstructuresand withaconfirmedDLBCLhistology.Allcaseswerediagnosed accordingtoWorldHealthOrganization(WHO)classification criteria.2 Patientswithtransformationfromanothertypeof
lymphomatoDLBCLwereexcluded.Patientswereconsidered
H.pyloripositivewhentheirhistologyresultswerepositive. Datawereretrievedfrompatient’schartswithallpatients havingsignedaconsentformsubmittedtothe localethics committeeinthediagnosisperiod.Allpatientsweresubjected toadetailedphysicalevaluationincludinganinvestigation ofBsymptoms(pain, nausea,dysphagia,bleeding, obstruc-tion),routinebloodexams(hemoglobin,totalanddifferential leukocyte counts, platelet count and peripheral smear for abnormal/blast cells), biochemical exams [liver function tests,serumlactatedehydrogenase(LDH),2microglobulin,
albumin,urea,creatinineanduricacid]andserologic investi-gationsforhepatitisBandCandHIV.Uppergastrointestinal endoscopic examinations were performed in 95% of the patients.Imagingstudiesincludedchestradiographsand/or computedtomographyscansandabdominalandpelvic com-putedtomography scans orultrasonography. Bulkydisease wasdefinedaslesionswithadiameter>10cm.Allpatients underwentbonemarrowaspirationandbiopsyaspartofthe stagingprocedure. Theinternational prognosticindex (IPI), age-adjustedIPI(aaIPI)5andAnnArborstage6,7 were
calcu-latedforeachpatient.
Allpatientsweretreatedbysystemicchemotherapymostly consistingofsixcyclesoftherituximab,cyclophosphamide,
doxorubicin, vincristine and prednisone (R-CHOP) regimen with the intention tocure.8 Patients withresidual disease
receivedlocalradiotherapy.Imagingstudiesandendoscopic examinationswereusedtoevaluateresponse.
Theinfluenceofthefollowingparameterswereevaluated intheresponsetotreatmentandsurvival:LDH,2
microglob-ulin,albumin,presenceofbulkydisease,Bsymptoms(fever, weightloss,pain,nausea,vomiting),aaIPI,typeoftreatment (surgeryplus chemotherapy,chemotherapy alone), anemia, dysphagia,bleeding,obstructionandpresenceofH.Pyloriat diagnosis.Anemiawasdefinedashemoglobin<12.0g/dLand elevatedLDHlevelsas>240U/L.
Allpatientsunderwentimagingandfollow-upendoscopic examinations (witha biopsy ofsuspicious lesions) to doc-ument treatment response. At the end of chemotherapy, response was classified as complete remission (CR), par-tialresponse(PR),stabledisease(SD)orprogressivedisease (PD) accordingtotheInternationalWorkingGroupcriteria.6
PatientswhofailedinitialtherapywithR-CHOP(PR,SDand PD)receivedhigh-dosechemotherapytogetherwith autolo-gousstemcelltransplant.PatientswithH.pyloriatdiagnosis alsoreceivedantibiotictherapy.
Statistical
analysis
SurvivalwasestimatedusingtheKaplan–Meiermethodand compared using the log-rank test. Theprognostic valueof thedifferentvariablesforclinicaloutcomewasestimatedby univariateandmultivariateanalyses,applyingtheCox propor-tionalhazardsregressionmodel.Two-sidedp-value<0.05was consideredsignificant.TheStatisticalPackagefortheSocial Sciences(SPSSversion15.0)software(Chicago,IL,USA)was usedfordataanalysis.
Results
Clinicalandhistologicalfeatures
Theclinicpathologiccharacteristicsofthe47male(45%)and 57 female(55%)patientswithgastricDLBCLwithamedian ageof69years(range:28–88years)arelistedinTable1.The mainpresentingsymptomwasabdominalpain(85%ofthe cases) and the two mostcommon serum alterations were elevationsin2 microglobulinandLDH in71%and 41%of
thecases,respectively.Hypoalbuminemiawasfoundin26/83 (31%)patients.Bleedingandobstructionwereuncommonat presentationandanemiawasonlypresentin43%(33/76)of cases.Amongthe45patientswhoweretestedforH.pylori, 13werepositive.Localizeddisease(AnnArborstagesIorII) waspresentin46%ofthecases,andmostpatients(67%)were inthelow/lowintermediateriskgroupaccordingtotheaaIPI; 48%hadgoodperformancestatus[EasternCooperative Oncol-ogyGroup(ECOG)score0].
Treatment,outcomeandprognosticfactors
Table1–Characteristicsofpatientsatdiagnosis.
Variable 104cases
Gender(male)–n(%) 47(45.2)
Ageatdiagnosis(median,range) 69(28–88) Presentingsymptoms–n/total(%)
Abdominalpain 63/74(85)
Weightloss 57/73(78)
Nausea/vomiting 37/72(51)
Bleeding 22/72(30.5)
Anemia–n/total(%) 33/76(43)
Dysphagia–n/total(%) 37/72(51) Helicobacterpyloriinfection–n/total(%) 13/45(29) HepatitisB(Anti-HBc/HBsAg+)a–n/total(%) 45/97(46.4)
Stage–n/total(%)
I–II 48/100(46)
III–IV 52/100(54)
ECOG–n/total(%)
0 49/101(48.5)
1–2 43/101(42.6)
≥3 09/101(8.9)
Bulkydisease(yes)–n/total(%) 25(24)
Bsymptoms–n/total(%) 45/102(44.1)
aaIPI–n/total(%)
0–1 64/95(67.3)
2–3 31/95(32.7)
Hypoalbuminemia–n/total(%) 26/83(31) Elevatedˇ2microglobulin–n/total(%) 57/80(71.2)
ElevatedLDH–n/total(%) 41/99(41.4) Typeoftreatment:R-CHOP–n/total(%) 87/100(87)
Alive–n/total(%) 82/104(78.8)
Medianfollow-upn/range(months)censoredgroup 25(1–77)
ECOG: Eastern Cooperative Oncology Group score; aaIPI: age-adjusted international prognostic index; LDH: lactate dehy-drogenase;R-CHOP: Rituximab,cyclophosphamide,doxorubicin, vincristineandprednisone.
a 5patientswithactivedisease.
almost all patients received chemotherapy (87–87/100) and justonepatientreceivedlocalradiotherapy.
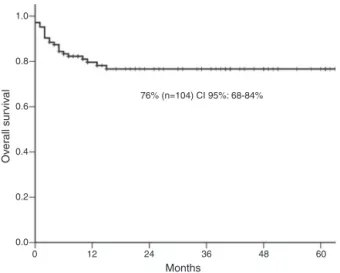
The five-year overall survivalwas 76% [95% confidence interval(CI):68–84%](Figure1)and46/71(64%)achieved com-pleteresponse.Overamedianfollow-upof25months(range:
1.0
0.8
0.6
76% (n=104) CI 95%: 68-84%
0.4
Ov
er
all sur
viv
al
0.2
0.0
0 12 24 36
Months
48 60
Figure1– The5-yearoverallsurvival.
Table2–Five-yearsurvivalrateaccordingtoclinical featuresatdiagnosis.
Variable No.ofcases Five-yearfollow-up
n Survivalrate p-Valuea
AnnArborstage
I-II 48 44 91 0.003
III-IV 52 35 64
Age-adjustedIPI
0–1 63 58 91 <0.0001
2–3 32 16 44
LDHlevels
Normal 58 54 92 <0.0001
Abnormal 41 24 50
Anemia(Hb<12g/dL)
No 43 36 83 0.007
Yes 33 19 54
Bsymptoms
No 57 53 91 <0.0001
Yes 45 27 56
Nausea/vomiting
No 35 29 82 0.04
Yes 37 23 60
Bulkydisease
No 79 66 82 0.02
Yes 25 16 57
IPI:internationalprognosticindex;LDH:lactatedehydrogenase. a Log-ranktest.
1–77months),the1-and5-yearsurvivalrateswere79%and 76%,respectively.Therewere22deaths.OnlyfourstageI–II cases (18%) had progressivedisease compared to 18 (82%) patients withadvanced disease hence,patientswith local-izedlymphoma(I–II)hadasignificantlyhigher5-yearsurvival probability(91%)comparedwiththosewithadvanced-stage (64%; p-value=0.003). The5-yearsurvivalofhigh-riskaaIPI patients wassignificantlyinferiortolow-risk patients(91% versus44%;p-value<0.0001:Table2).
In the univariate analysisusing Cox regression, several variables were associatedtothehazard risk(HR)fordeath (Table3).However,inthemultivariateanalysisjusttheaaIPI
Table3–Univariateanalysisofhazardriskfordeath.
Variable HR 95%CI p-Value
Bulkydisease 2.34 0.99–5.54 0.05
Hypoalbumenia 3.08 1.27–7.47 0.01
StageIII–IV 4.67 1.57–13.9 0.006
BMinvolvement 4.07 1.55–10.7 0.004
Bsymptoms 6.21 2.09–18.4 0.001
LDHabnormal 8.89 2.95–26.8 <0.0001
aaIPI 3.62 2.21–5.93 <0.0001
HR:hazardrisk;95%CI:95%confidenceinterval;BM:bonemarrow; LDH:lactatedehydrogenase;aaIPI:age-adjustedinternational pro-gnosticindex.
remainedaspredictiveofmortality(HR:3.62;95%CI:2.21–5.93;
p-value<0.0001).
Discussion
AnunexpectedhighincidenceofprimarygastricDLBCLwas foundin this multicenter series of patients treatedat ter-tiary care centers. Advanced stage was present in half of thepatientsandonethirdhadhigh-riskaaIPI.Regardlessof the prevalenceoffactors considered to beassociated with poorprognosis(advancedstage,Bsymptoms,bulkydisease, elevatedLDH and high-riskaaIPI),the outcomes compared favorablywithregistrydata.9
The majority of the published data showed that pri-marygastricDLBCLpredominatesinmen.10,11 Interestingly,
inthis cohortofBrazilianandEuropeanpatients, aslightly higherincidencewasobservedinwomen.Mostpatientshad advancedstagediseaseandahigh-riskaaIPIatdiagnosis.The medianagewas69yearsold,rangingbetween28and88years, whichisinagreementwithothersstudies.12,13InnodalDLBCL,
anagehigherthan 60yearsisaconfirmedpoorprognostic factor.Similar toanotherstudy, norelationshipwas found betweenageandsurvival.14
The main clinical presentations of the disease were non-specific gastrointestinal symptoms, including abdomi-nalpain, nausea, vomitingand weight loss.Some authors identified abdominal pain, gastrointestinal bleeding and nausea/vomiting as the most common symptoms in large cohortsofpatients.12,15 Theresultsofthisstudywere
sim-ilar with 85% of evaluable patients developing abdominal pain, 75% had weight loss and 51% had nausea. Ane-mia, detected in 43% of the evaluable patients, was also common. In general, the clinical manifestationsof gastric lymphomaare non-specificwhich may resultin adelayed diagnosis.
Lowalbuminlevelshavebeensuggestedasanimportant predictorofsurvivalinelderlylymphomapatientsand par-ticularlyingastricDLBCL.16Inthisstudy,31%ofthepatients
hadhypoalbuminemia,nevertheless,thishypothesiswasnot confirmedinthemultivariateanalysis.
Thirteenofthe45patientswhowere testedforH.pylori
werepositive.Thisisnotahighincidence,butH.pylori infec-tionplaysaroleinDLBCL.17Hence,thesepatientswerealso
treatedforH.pyloriinfection.
Univariate analysis confirmed published data regarding the prognostic impact of the aaIPI, ECOG, elevated DHL, advancedstage,Bsymptoms,anemia,bulkydiseaseand albu-min levels.10,15 Nevertheless, multivariate analysis showed
that onlyaaIPIretained its significanceasan independent predictorofoutcome.Almostonequarterofthepatientshad bulkydiseaseatdiagnosisandthisturnedouttobeanegative impactfactor,andalthoughrituximabdecreasedtheadverse prognosticvalue ofbulky disease,it did noteliminate the effectcompletely.18
One ofthe limitations of this study is its retrospective designhoweverthiswasthebestwaytogetarelevant num-berofthepatientswithsimilarclinicalfeatures.TheaaIPIwas identifiedasapredictorofsurvivalinpatientstreatedwith conventionalimmunochemotherapy.
Authors’
contributions
M.T.Delamain,M.G.DaSilva,J.DesterroandS.Luminari con-ceivedanddesignedallstudy.M.G.DaSilva,J.Desterro,E.C.M. Miranda,A.Fedina,andC.S.Chiattonewereresponsiblefor thedataacquisition.E.C.M.Mirandaappliedallanalyses.M.T. Delamain,M.G.DaSilva,J.Desterro,andS.Luminari,F.Merli, C.S.Chiattone,K.B.Pagnano,M.Federico,C.A.DeSouzawere responsibleforinterpretation,manuscriptdraftingandcritical revision.Allauthorsapprovedthemanuscript.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.D’AmoreF,BrinckerH,GronbaekK,ThorlingK,PedersenM, JensenMK,etal.Non-Hodgkin’slymphomaofthe
gastrointestinaltract:apopulation-basedanalysisof incidence,geographicdistribution,clinicopathologic presentationfeatures,andprognosis.DanishLymphoma StudyGroup.JClinOncol.1994;12(8):1673–84.
2.SwerdlowSH,CampoE,HarrisNL,JaffeES,PileriSA,SteinH, etal.WHOclassificationoftumorsofhematopoieticand lymphoidtissues.fourthed.Lyon:IARCPress;2008.
3.CohenS,SchoryPC.Clinicalpresentationanddiagnosisof primarygastrointestinallymphomas.UptoDate.2001;9:2.
4.Medina-FrancoH,GermesSS,MaldonadoCL.Prognostic factorsinprimarygastriclymphoma.AnnSurgOncol. 2007;14(8):2239–45.
5.SehnLH,BerryB,ChhanabhaiM,FitzgeraldC,GillK, HoskinssP,etal.TherevisedInternationalPrognosticIndex (R-IPI)isabetterpredictorofoutcomethanthestandardIPI forpatientswithdiffuselargeB-celllymphomatreatedwith R-CHOP.Blood.2007;109(5):1857–61.
6.ChesonBD,HorningSJ,CoiffierB,ShippMA,FisherRI, ConnorsJM,etal.ReportofanInternationalWorkshopto standardizedresponsecriteriafornon-Hodgkin’s lymphomas.JClinOncol.1999;17(4):1244–53[Erratumin:J ClinOncol.2000:18(11);2351].
7.CarbonePP,KaplanHS,MusshoffK,SmithersDW,TubianaM. ReportoftheCommitteeofHodgkin’sDiseaseStaging classification.CancerRes.1971;31(11):1860–1.
8.SehnLH,DonaldsonJ,ChhanabhaiM,FitzgeraldC,KillK, KlasaR,etal.IntroductionofcombinedCHOPplusrituximab therapydramaticallyimprovedoutcomeofdiffuselarge B-celllymphomainBritishColumbia.JClinOncol. 2005;23(22):5027–33.
9.CastroFA,JansenL,KrilaviciuteA,KatalinicA,PulteD,SirriE, etal.SurvivalofpatientswithgastriclymphomainGermany andintheUnitedStates.JGastroenterolHepatol.
2015;30(10):1485–91.
10.RotaruI,GãmanGD,StãnescuC,GãmanAM.Evaluationof parameterswithpotentialprognosisimpactinpatientswith primarygastricdiffuselargeB-celllymphoma(PG-DLBCL). RomJMorpholEmbryol.2014;55(1):15–21.
11.HuangJ,JiangW,XuR,HuangH,LvY,XiaZ,etal.Primary gastricnon-Hodgkin’slymphomainChinesepatients:clinical characteristicsandprognosticfactors.BMCCancer.
2010;10:358.
non-Hodgkinlymphomainadults:clinicopathologicand survivalcharacteristics.CollAntropol.2010;34(2):413–7.
13.FerreriAJ,MontalbanC.PrimarydiffuselargeB-cell lymphomaofthestomach.CritRevOncolHematol. 2007;63(1):65–71.
14.HosseiniS,DehghanP.Primarynon-Hodgkinlymphomaof thestomach:clinicopathologicalcharacteristicsand prognosticfactorsinIranianpatients.IranJCancerPrev. 2014;7(Fall(4)):219–24.
15.DingD,PeiW,ChenW,ZuoY,RenS.Analysisofclinical characteristics,diagnosis,treatmentandprognosisof46 patientswithprimarygastrointestinalnon-Hodgkin lymphoma.MolClinOncol.2014;2:259–64.
16.ChiharaD,OkiY,IneS,KatoH,OnodaH,TajiH,etal.Primary gastricdiffuselargeB-cellLymphoma(DLBCL):analysesof
prognosticfactorsandvalueofpretreatmentFDG-PETscan. EurJHaematol.2010;84(6):493–8.
17.KuoSH,YehKH,WuMS,LinCW,HsuPN,WangHP,etal. Helicobacterpylorieradicationtherapyiseffectiveinthe treatmentofearly-stageH.pylori-positivegastricdiffuselarge B-celllymphomas.Blood.2012;119(21):4838–44.