164
Original Articles
Profile of elderly persons with metabolic syndrome and factors
associated with possible drug interactions
Daniela Santos Tavares1
Nayara Cândida Gomes2
Leiner Resende Rodriguês3
Darlene Mara dos Santos Tavares3
1 Universidade Federal do Triângulo Mineiro, Instituto de Ciências da Saúde, Curso de Graduação em
Medicina. Uberaba, Minas Gerais, Brasil.
2 Universidade Federal do Triângulo Mineiro, Instituto de Ciências da Saúde, Programa de Pós-graduação
Stricto Sensu em Atenção à Saúde. Uberaba, Minas Gerais, Brasil.
3 Universidade Federal do Triângulo Mineiro, Instituto de Ciências da Saúde, Departamento de Enfermagem
em Educação e Saúde Comunitária. Uberaba, Minas Gerais, Brasil.
Correspondence
Darlene Mara dos Santos Tavares [email protected]
Abstract
Objectives: To describe the sociodemographic, clinical and pharmacotherapy characteristics of elderly persons with metabolic syndrome and to identify factors associated with drug interactions among these individuals. Method: A quantitative, analytical and transversal study was carried out among 263 elderly people with metabolic syndrome in the urban area of Uberaba, Minas Gerais, Brazil. Possible drug interactions were identified and classified according to the Micromedex® DrugReax System. The chi-squared test and the multiple logistic regression model were used for analysis (p<0.05). Results: The majority of the individuals were female (70.7%); aged 60 to 74 years (72.3%); lived with a spouse/
partner (63.9%); had some schooling (74.1%); an individual monthly income of ≤ one
minimum wage (77.1%); lived with others (88.2%); had five or more morbidities (89.7%) and exhibited polypharmacy (73.0%); used potentially inappropriate medications (54.4%) and had possible drug interactions (75.3%). Associated with the possible presence of drug interactions were: age range (p=0.005), polypharmacy (p<0.001) and use of potentially inappropriate medications (p=0.006). Conclusion: Possible drug interactions were associated with increased age, polypharmacy and the use of potentially inappropriate medications. This study contributes to knowledge of these possible interactions among elderly people with metabolic syndrome, and as such can be considered an important tool for planning actions to ensure the safety of these individuals who, due to the complexity of their treatment, use multiple medications.
165
INTRODUCTION
Metabolic Syndrome (MS) consists of the concomitance of metabolic and hemodynamic disorders, such as hyperglycemia, systemic arterial hypertension (SAH), abdominal obesity and dyslipidemia. It becomes more prevalent as age increases and among individuals with a determined disease, such as type 2 diabetes mellitus (DM2) and SAH1.
Increasingly prevalent, MS is present in approximately 20 to 30% of the adult population, with a significant increase from 60 years of age when it affects almost 60% of the global population2. Among
the elderly population in regions of Brazil, prevalence
varies from 18 to 64.1%3-5. Population aging
has brought about an increase in the prevalence of MS in the global population4. This syndrome is therefore
of great importance among the elderly population, as it is directly related to the increase in death rates due to cardiovascular events, mobility disorders, cognitive deficit and depression in this group3.
Elderly patients with MS are more susceptible to the occurrence of polypharmacy, which consists
of the concomitant use of five or more drugs6
and is associated with a higher risk of use of potentially inappropriate medications (PIM) and the occurrence of adverse events related to medications and drug interactions (DI), resulting in increased hospitalization and mortality in this population7.
The presence of DI is one of the main risks involved in the use of drugs by the elderly8. The
physiological changes that occur with the aging process, the presence of chronic diseases and the large number of medications used by this population, can mask the occurrence of DI, which can be confused with the worsening of health status or treatment ineffectiveness7.
In the study conducted among elderly persons in the community in Timóteo (Minas Gerais), the prevalence of DI was 55.6%9. In a survey conducted
in Scotland, the prevalence among the elderly was 34.1%10. These percentages indicate that DI among
the elderly is a public health problem and must be carefully monitored.7.
DI is the pharmacological or clinical response that arises from the interference of the action of a particular drug, food or any chemical on the effect of another drug, administered prior or concomitantly to the first medication11. It can be classified according
to severity, such as: severe when potentially resulting in life-threatening and/or irreversible damage, requiring urgent medical intervention to minimize adverse effects; moderate when they can cause a worsening of the patient's clinical condition and/or may require additional treatment, hospitalization, or if the patient is already hospitalized, lead to longer hospitalization; and minor when the clinical effects are mild and the consequences may result in discomfort for the individual but do not require major changes in therapy12.
Thus, DI may compromise patient safety, making it necessary to evaluate and monitor drug therapy in the elderly. The use of adequate tools that facilitate the identification of the occurrence of possible DI can contribute to the efficiency of pharmacological prescription, such as the Micromedex® DrugReax System, which is available online and free of charge12,13.
In Brazil, there is a lack of knowledge about the occurrence of DI among outpatients14. The present
study is therefore important as when caring for patients, health professionals should consider the relationship between costs and benefits based on scientific evidence.
In view of the above, the present study aims to describe the sociodemographic, clinical and pharmacotherapy characteristics of elderly persons with metabolic syndrome and to identify factors associated with possible drug interactions among these individuals.
METHOD
166
elderly people. The sample size calculation considered a prevalence of adhesion of 56%15, a precision of
6% and a confidence interval of 95%, resulting in a sample of 263 subjects, who were selected by means of a random draw. For the present study, the inclusion criteria were an age of 60 years or over, having been diagnosed with MS at the UFTM Metabolic Syndrome outpatient clinic in accordance with the criteria of the International Diabetes Federation16;
and residing in the urban area of Uberaba, Minas Gerais. The exclusion criteria were to have suffered cognitive decline as evaluated by the Mini-Mental State Exam (MMSE), translated and validated for Brazil17, which provides information on different
cognitive parameters based on the following cut-off points: ≤13 for illiterates, ≤18 for a medium level of schooling (one to 11 years) and ≤26 for a high level of schooling (<11 years)12; have communication
problems such as deafness (not corrected with the assistance of devices) and serious speech disorders.
Data collection was performed from January to March 2015 and the data were obtained through home interviews conducted by a previously trained interviewer (including training on ethical research issues).
An instrument prepared by the researchers of the Research Group on Public Health/UFTM was used to obtain sociodemographic data. The number of morbidities was obtained through data relating to the 26 items included in the Brazilian Questionnaire on Functional and Multidimensional Assessment18.
The use of regular medications was determined through the question "Could you show me the medications you are currently using?" The elderly persons were asked to provide the packaging of the medicines and the prescription. Also registered were: the pharmaceutical form of the drugs, the amount consumed and the number of ingestions per day. A pilot study was carried out to verify the adequacy of the instrument developed by the authors to collect the data relating to medications in regular use. The analysis of the medical prescriptions of the elderly was based on the following parameters: existence of polypharmacy; presence of possible DI (drug-drug), use of PIM and self-medication data. Polypharmacy was considered to be the simultaneous use of five or more drugs6. The presence of possible DI
(drug-drug) was identified and classified according to severity (severe, moderate and minor), according
to Micromedex's DrugReax System®. This tool
is recognized worldwide and is ideal for health professionals who require unbiased information. It is also supported by systematic reviews about medications12,13. The updated version of the Beers
criteria of 2012 was used for the evaluation of PIM, with the PIM and the classes to be avoided in the elderly identified19. Data on self-medication
were obtained through the question: "Do you take medicines on your own?"; if yes, "Which medicines?" Home remedies, teas, herbal and homeopathic treatment were not considered.
The sociodemographic variables considered were: gender (female, male); age group (60 to 74, 75 or more); schooling (no schooling, schooling); income (≤1 minimum wage, >1 minimum wage); living arrangements (alone, with others); marital status (with partner, without partner). The clinical variables were: number of self-reported morbidities (0 to 4, 5 or more); polypharmacy (yes, no); possible DI (yes, no); self-medication (yes, no) and PIM (yes, no).
The following statistical analyzes were performed: descriptive and bivariate using the chi-squared test, prevalence ratios and odds ratios for categorical variables. The variables that met the criterion of
p<0.1 were included in the multiple logistic regression model with a significance level (α) of 95%. The factors associated with the presence of possible DI were identified using the multiple logistic regression model (saturated model), considering a significance level of 5% (p<0.05) and a 95% confidence interval (CI).
To verify the factors associated with the presence of possible DI, the following variables were considered as predictors: gender; age group; number of morbidities; polypharmacy, self-medication and use of PIM.
167
where the objectives and the Form of Free and Informed Consent were presented and pertinent information was provided. Only after the consent of the interviewee and signature of the said consent form was the interview conducted, following the precepts established by Ministry of Health Resolution 466/1220.
RESULTS
In all, 282 individuals were approached to compose the study sample. Of these, nine exclusions
occurred (four because of cognitive decline and five because they were not found after three attempts) and there were ten losses (one incomplete interview, three deaths and six refusals) (Figure 1).
Among the elderly persons interviewed (263), the majority were female (186, 70.7%); aged 60 to 74 years (190, 72.3%); had a partner (168; 63.9%); some schooling (195, 74.1%); an individual monthly income of up to one minimum wage (205, 77.1%) and lived with others (232, 88.2%). Table 1 shows the sociodemographic variables of the elderly with MS.
Figure 1. Sample composition. Uberaba, Minas Gerais, 2015.
Table 1. Distribution of frequency of sociodemographic variables among elderly persons with metabolic syndrome.
Uberaba, Minas Gerais, 2015.
Variables n (%)
Gender
Male 77 (29.3)
Female 186 (70.7)
Age group (years)
60-74 190 (72.3)
75 or more 73 (27.7)
Marital status
With partner 168 (63.9)
Without partner 95 (36.6)
168
Among the five criteria for the diagnosis of MS according to the International Diabetes Federation16,
the highest percentages of disorders were abdominal circumference (263; 100.0%), which is the primary criteria for the diagnosis of MS; and fasting glycemia, in which 241 (91.6%) of elderly persons had levels over 100 mg/dL. Systemic blood pressure was next, with 168 (63.9%) individuals having levels above those considered normal (≥130x85mmHg). In terms of lipid profile, 180 individuals (68.4%) had altered HDL-C levels (men below 50mg/dL and women below 40mg/dL) and 120 individuals (45.6%) had triglycerides levels above 150mg/dL.
A total of 236 (89.7%) elderly persons had five or more morbidities. With respect to polypharmacy, 192 (73.0%) used five or more drugs. Regarding self-medication, 85 (32.3%) reported taking medicines on their own. It was found that 143 (54.4%) elderly patients used PIM. Of these, 78 (54.5%) used one, 49 (34.3%) two, and 16 (11.2%) from three to seven.
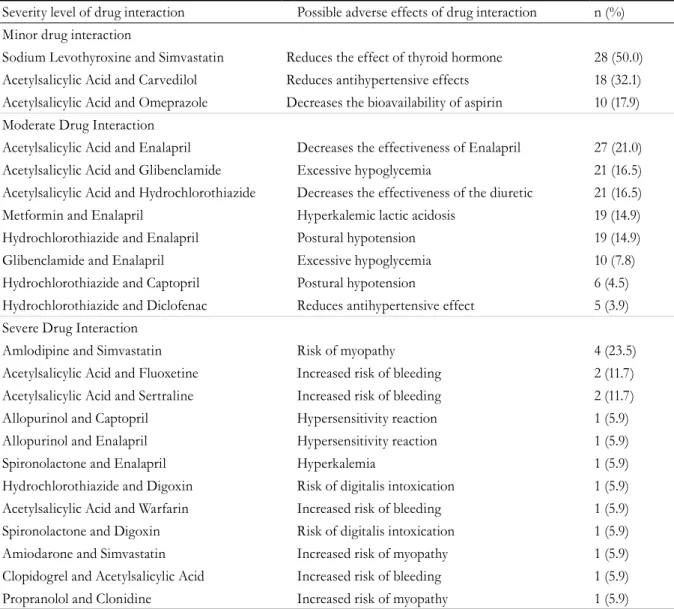
The presence of potential DI was identified in 198 (75.3%) elderly persons. Of these, 56 (27.9%) were classified as minor, 128 (63.7%) as moderate and 17 (8.4%) as severe. Of the minor DI, the most frequent combination in the present study was that of Sodium Levothyroxine and Simvastatin (28;
50.0%). In the moderate group, the most frequent association was between Acetylsalicylic Acid and Enalapril (27; 21.0%), while of the severe interactions the association between Amlodipine and Simvastatin was most frequent (4; 23.5%) (Table 2).
The possible DI identified in the prescriptions and their clinical implications, according to Drug-Reax®8,13, are set out in Table 2.
Higher prevalences of potential DI were found in elderly women (146; 78.1%), those aged 75 years or more (72; 98.6%), those with five or more morbidities (Table 1), those with polypharmacy (178, 93.2%), and those who performed self-medication (73, 85.9%) and used PIM (135, 94.4%).
The variables of the preliminary bivariate analysis submitted to multivariate analysis in the multiple binomial logistic regression model were: gender (p=0.46), age group (p<0.001), number of morbidities (p<0.001), polypharmacy (p<0.001), self-medication (p=0.006), PIM use (p<0.001).
The presence of polypharmacy (p<0.001) and the use of PIM (p=0.006) were consolidated factors associated with the presence of potential DI among elderly persons with MS aged 75 years or more (p=0.005) (Table 4).
Variables n (%)
Education
No schooling 68 (25.9)
With schooling 195 (74.1)
Income (in minimum salaries) *
<1 205 (77.1)
>1 58 (22.1)
Living arrangement
Lives alone 31 (11.8)
Lives with others 232 (88.2)
169
Table 2. Distribution of possible adverse drug interaction events and the frequency of possible drug interactions,
according to Drug-Reax®, identified in the prescriptions of elderly persons with metabolic syndrome. Uberaba,
Minas Gerais, 2015.
Severity level of drug interaction Possible adverse effects of drug interaction n (%) Minor drug interaction
Sodium Levothyroxine and Simvastatin Reduces the effect of thyroid hormone 28 (50.0) Acetylsalicylic Acid and Carvedilol Reduces antihypertensive effects 18 (32.1) Acetylsalicylic Acid and Omeprazole Decreases the bioavailability of aspirin 10 (17.9) Moderate Drug Interaction
Acetylsalicylic Acid and Enalapril Decreases the effectiveness of Enalapril 27 (21.0) Acetylsalicylic Acid and Glibenclamide Excessive hypoglycemia 21 (16.5) Acetylsalicylic Acid and Hydrochlorothiazide Decreases the effectiveness of the diuretic 21 (16.5) Metformin and Enalapril Hyperkalemic lactic acidosis 19 (14.9) Hydrochlorothiazide and Enalapril Postural hypotension 19 (14.9) Glibenclamide and Enalapril Excessive hypoglycemia 10 (7.8) Hydrochlorothiazide and Captopril Postural hypotension 6 (4.5) Hydrochlorothiazide and Diclofenac Reduces antihypertensive effect 5 (3.9) Severe Drug Interaction
Amlodipine and Simvastatin Risk of myopathy 4 (23.5)
Acetylsalicylic Acid and Fluoxetine Increased risk of bleeding 2 (11.7) Acetylsalicylic Acid and Sertraline Increased risk of bleeding 2 (11.7) Allopurinol and Captopril Hypersensitivity reaction 1 (5.9) Allopurinol and Enalapril Hypersensitivity reaction 1 (5.9)
Spironolactone and Enalapril Hyperkalemia 1 (5.9)
Hydrochlorothiazide and Digoxin Risk of digitalis intoxication 1 (5.9) Acetylsalicylic Acid and Warfarin Increased risk of bleeding 1 (5.9) Spironolactone and Digoxin Risk of digitalis intoxication 1 (5.9) Amiodarone and Simvastatin Increased risk of myopathy 1 (5.9) Clopidogrel and Acetylsalicylic Acid Increased risk of bleeding 1 (5.9) Propranolol and Clonidine Increased risk of myopathy 1 (5.9)
Table 3. Distribution of sociodemographic, clinical and pharmacotherapy variables of elderly persons with
metabolic syndrome, according to the presence of potential drug interactions. Uberaba, Minas Gerais, 2015.
Variables Presence
of DI
Absence of DI
n (%) n (%) PR* (CI)** OR*** (CI)** p**** Sex
Male 51 (67.1) 25 (35.9) 0.85 (0.72-1.02) 0.57 (0.31-1.03) 0.046 Female 146 (78.1) 41 (21.9)
Age group
75 or more 72 (98.6) 1 (1.4) 0.27 (0.00-0.19) 0.66 (0.60-0.74) 0.000 60-74 125 (65.8) 65 (34.2)
Number of morbidities
5 or more 190 (80.5) 46 (19.5) 3.10 (1.63-5.89) 11.80 (4.70-29.58) 0.000
0 to 4 7 (25.9) 20 (74.1)
170
DISCUSSION
The higher percentage of female subjects is consistent with investigations among elderly people with MS3,4. As women attend health services more,
they are more likely to be diagnosed and treated for possible morbidities, including MS. In addition, the hormonal changes that occur in menopause make them more susceptible to increased waist circumference and the risk of cardiovascular diseases1.
In terms of age, a study conducted among elderly persons residing in the community in São Paulo found that those aged 60 to 69 years were approximately 11 times more likely to have MS (OR=10.945; p<0.001)22.
Therefore, younger people should be advised of the risks of cardiovascular diseases, since morbidity can affect their quality of life and damage their health during aging22. This finding will help health teams to
prioritize health promotion and actions that prevent disease with the aim of keeping these elderly people independent as long as possible.
Regarding marital status, partners can play a key role in health care, as they can contribute to the continuity of treatment, through encouragement, health care and assistance with physical activities and medication15.
In the present study, the higher percentages of MS among elderly persons with some education are consistent with a survey conducted among elderly people with this condition living in the community
in Porto Alegre (Rio Grande do Sul) (91.7%)15.
Schooling can interfere with the understanding of therapeutic behaviors and learning about self-care, such as problems with drug use and dieting. Health professionals must communicate effectively with the elderly and their families through clear and objective
Table 4. Multiple logistic regression model for the variables associated with the presence of potential drug
interactions among the elderly with metabolic syndrome. Uberaba, Minas Gerais, 2015.
Variables OR* CI95%** p***
Women 1.29 (0.49–3.42) 0.597
Aged 75 years and over 21.71 (2.54-185.66) 0.005
Five or more morbidities 0.61 (0.17–2.18) 0.447
Presence of polypharmacy 0.08 (0.03–0.20) 0.000
Self-medication 0.54 (0.21–1.43) 0.221
Use of PIM**** 0.24 (0.08–0.66) 0.006
*OR: Odds Ratio; **CI: Confidence interval; ***p<0.05, in multiple logistic regression model; **** Potentially inappropriate drug.
Variables Presence
of DI
Absence of DI
n (%) n (%) PR* (CI)** OR*** (CI)** p**** Polypharmacy
Yes 178 (93.2) 13 (6.8) 3.53 (2.39-5.20) 38.19 (17.69-82.42) 0.000
No 19 (26.4) 53 (73.6)
Self-medication
Yes 73 (85.9) 12 (14.1) 1.23 (1.08-1.40) 2.64 (1.33-5.27) 0.006
No 124 (69.7) 54 (30.3)
Potentially inappropriate drug
Yes 135 (94.4) 8 (5.6) 1.82 (7.10-35.06) 15.78 (1.53-2.18) 0.000
No 62 (51.7) 58 (48.3)
171
language about the care needed to improve the health of this population15.
It is noteworthy that 38.3% of elderly persons in Brazil have a monthly income between half and
one minimum wage23, which can contribute to the
understanding of the results found. The low income of the elderly in this study represents a challenge for maintaining basic needs and health care. Income is considered a factor that influences access to health services, as well as income satisfaction21. In this
context, actions in public health should be appropriate for the economic conditions of the elderly, seeking effective and quality treatment.
The living arrangement data of the present study diverged from that of a survey of elderly people from a specialist outpatient clinic in Vitória (Espirito Santo), where the majority lived alone (32.3%)24. It is
important to study the composition of the households in which the elderly live, as other relatives can help with transportation, medical care and domestic services, as well as providing company and emotional support for both parties24.
In relation to the components of MS, there are divergences between the present study and investigations among elderly people with MS living in the community in Porto Alegre (Rio Grande do Sul), where SAH was the most frequent component (83.6%)15; and a study carried out in the
north of Finland, in which SAH was also the most prevalent component, among both women (89.0%) and men (91.8%)25. It is important to observe the
relationship of the various risk factors associated with cardiovascular events, such as changes in glycemia, elevated triglycerides, abdominal obesity and increased values of systemic arterial pressure.
The number of self-reported morbidities in the present study was higher than that of the elderly resident in the community in Bagé (Rio Grande do Sul), in which 50.0% of respondents reported having two or more morbidities26, although the diagnosis
of MS was not specified. The higher values found in the present study can be attributed, in part, to the characteristics of the group, namely elderly persons with MS. It is noteworthy that no studies of the number of self-reported morbidities of elderly persons with MS were found in Brazilian or non-Brazilian literature.
Brazilian studies have identified a prevalence of polypharmacy of between 11.0% and 71.1%, with the highest frequency among elderly persons with MS 27-30.The higher prevalence of chronic illnesses among
elderly persons leads to an ongoing increase in the consumption of medications in this age range. The practice of polypharmacy is therefore often necessary. However, the use of multiple medications increases the risk of DI. Therefore, the implications of this consumption need to be measured and evaluated for their risks/benefits8.
In the present study, the prevalence of the practice of self-medication is similar to a study of the elderly living in the community in Goiânia (Goias) (35.7%)31. Lower values were identified in a study
the among elderly from the community in Recife (Pernambuco) (6.7%)28 and higher prevalances were
found in a study with elderly in the community of Teresina (Piaui) (62.5%)30. The elderly population
carries out self-medication to treat some symptoms such as headaches; and studies indicate that easy access to these drugs is a contributing factor to this practice31. The improper use of medications
has consequences for the life and health of the elderly, such as delayed treatment, failure to achieve the expected results, aggravation of the signs and symptoms of the diseases, and potentiating adverse drug reactions caused by greater use of the medication than is required30,31.
The percentage of PIM found in this study was similar to that among elderly persons in the community of Ibiraiaras (Rio Grande do Sul) (44.7%)30. This value is higher than the studies among
elderly in the community in the city of São Paulo (28.0%)7, and in Goiânia (Goiás) (24.6%), in which
the drugs considered to be inappropriate were long-acting benzodiazepines (34.2%) and antidepressants (16.0%)31. A study developed in India identified
greater values than the present study (87.3%)32.
However, the diagnosis of MS was not reported in any of the aforementioned surveys. There is evidence that the prescription of PIM is associated with the triggering of DI and hospitalizations and, when combined with the presence of comorbidities and polypharmacy, exposes the elderly to a high risk of mortality7. The lack of cost-effective therapeutic
172
to the severity and prevalence of possible DI33.
The association between the presence of possible DI and age found in the present study diverged from an investigation of elderly persons living in the community in the city of Rio de Janeiro11.
The relationship between increasing age and the occurrence of DI deserves further investigation10,11,
as the aging process may contribute to the increase in the prevalence of chronic diseases, which causes the elderly to use more drugs7, resulting in a greater
possibility of DI10,27.
The treatment of MS is complex, as it requires the use of several drugs, which increases the risk of
DI34. The association between polypharmacy and
the occurrence of DI corroborates other Brazilian studies11,33. Thus, as DI is a constant risk, especially
among elderly people who use polypharmacy, knowledge about the subject is vital in order to avoid greater risks to the health of these individuals11.
Polypharmacy is associated with the risk of the use of PIM, which increases the risk of DI among the elderly, who are more vulnerable due to their pharmacokinetic and pharmacodynamic characteristics35. The use of PIM and the presence of
DI are factors that are directly related to the quality of life of the elderly, either acting alone or in association with physiological changes and comorbidities, which reinforces the need for evaluation of the therapeutic plan, since the greater the number of drugs prescribed, the greater the risk of the use of PIM and exposure to DI35. It is essential to assess the risks and benefits
related to prescribed pharmacotherapy, with doses monitored and/or reduced, as many interactions may reduce the effectiveness of medications27.
Thus, health professionals should be aware of information about DI and propose appropriate interventions when necessary. It is also the responsibility of these professionals to use the available literature in relation to DI and to individualize recommendations based on the specific characteristics of each elderly person35.
The results of the present study are useful for the development of mechanisms to evaluate the prescription process in order to reduce failings in the pharmacotherapy of the elderly. Misuse of medicines in the elderly is a significant public health The frequency of potential DI did not differ
from that described in scientific literature. These values can vary greatly and high prevalence is found among the elderly9,33.
The medications most frequently involved in DI are those used in the everyday management of the chronic diseases of the elderly. These conditions require constant monitoring, since their effects can worsen the clinical condition of the elderly, which may result in the need for additional treatment, hospitalization, costs to the health system, or if the elderly person is already hospitalized, lead to a longer hospitalization period. One way to address this is by selecting drugs that do not produce interactions, however, if there is no such possibility, the drugs that interact with each other should be monitored27.
Similar results in relation to the severity of DI were obtained in studies of the elderly in the
community in Ribeirão Preto (São Paulo)33, in
Timóteo (Minas Gerais)9, and among elderly
patients attending the geriatric outpatient clinic at the Hospital Universitário de Belém (Pará), in which the majority had moderate severity.
Studies developed in the states of São Paulo33 and
Minas Gerais9 obtained divergent data regarding the
most frequent DI. In the former, the most frequent severe DI was between the medicines Amlodipine and Simvastatin (15.0%) and the most common moderate DI was between Acetylsalicylic Acid and Enalapril (42.5%). In the second study, the most frequent severe DI involved Amlodipine and Simvastatin (26.7%), the most common moderate DI was between Acetylsalicylic Acid and Hydrochlorothiazide (26.7%) and the most prevalent mild DI was between Amlodipine and Ibuprofen (21.7%).
DI are frequent and need to be prevented, especially in the elderly, who are more sensitive to the therapeutic and toxic effects of medications27.
Thus, understanding the interactions between the medicines indicated for the control of MS allows such risks to be avoided and safer medications to be prioritized, with less risk of triggering undesirable effects and allowing better therapeutic responses34.
173
problem as it exposes them to the potential risks of medication. Health professionals can improve care through the implementation of protocols and procedures that aim to minimize and avoid inadequacies in prescriptions.
Limitations of the present study include the non-evaluation of clinical symptoms related to the presence of potential DI or PIM use, since the data were collected in a single period, which did not allow follow-up monitoring of related clinical symptoms.
CONCLUSION
In the present study the majority of respondents were female; aged 60 to 74 years; lived with a partner; had some schooling; an individual monthly income of up to one minimum wage and lived with others; presented five or more morbidities; used five or more drugs; took medicines on their own; used potentially inappropriate drugs and had potential drug interactions.
The presence of potential drug interactions among elderly persons with metabolic syndrome was associated with an age of 75 years or older, polypharmacy and the use of potentially inappropriate medications.
The present study therefore contributes to knowledge of drug interactions among elderly persons with metabolic syndrome, representing an important tool for the planning of actions to ensure the safety of those individuals who use multiple medications due to the complexity of the treatment of this syndrome.
ACKNOWLEDGEMENTS
The authors would like to thank the Ministry of Education, the Coordination for the Improvement of Higher Education Personnel (CAPES), the Research Support Foundation of Minas Gerais (FAPEMIG) and the Universidade Federal do Triângulo Mineiro (UFTM).
REFERENCES
1. Barbalho SM, Bechara MD, Quesada K, Gabaldi MR, Goulart RA, Tofano RJ, et al . Síndrome metabólica, aterosclerose e inflamação: tríade indissociável? J Vasc Bras [Internet]. 2015 [acesso em 12 dez. 2017];14(4):319-27. Disponível em: http://www. scielo.br/scielo.php?script=sci_arttext&pid=S1677-54492015000400319&lng=pt&tlng=pt
2. Wu TT, Chen IJ, Cho SL, Chiou AF. The
Relationship between health-promoting behaviors and metabolic syndrome in community-dwelling older adults. Biol Res Nurs [Internet]. 2016 [acesso em 21 mar. 2018];18(5):549-57. Disponível em: http:// journals.sagepub.com/doi/abs/10.1177/10998004166 55882?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref. org&rfr_dat=cr_pub%3dpubmed
3. Saad MAN, Cardoso GP, Martins WA, Velarde LGC, Cruz FRA. Prevalência de síndrome metabólica em idosos e concordância entre quatro critérios diagnósticos. Arq Bras Cardiol [Internet]. 2014 [acesso em 21 mar. 2018];102(3):263-9. Disponível em: http://www.scielo.br/ scielo.php?script=sci_arttext&pid=S0066-782X2014000 300008&lng=en&nrm=iso&tlng=pt
4. Calixto SCS, Vinagre RMFD, Rocha GF, França TG. Prevalência da Síndrome Metabólica em idosos. Saúde Foco [Internet]. 2016 [acesso em 21 mar. 2018];3(2):119-35. Disponível em: http://www.scielo. br/pdf/abc/2014nahead/0066-782X-abc-20140013.pdf
5. Zoraski H, Fiametti M, Santos R, Gregoletto MLO, Cremonese C. Síndrome metabólica em idosos de Nova Roma do Sul, RS: prevalência e fatores associados. ABCS Health Sci [Internet]. 2017 [acesso em 14 out. 2017];42(3):147-55. Disponível em: https:// www.portalnepas.org.br/abcshs/article/view/955
6. Hovstadius B, Petersson G. Factors leanding to excessive polypharmacy. Clin Geriatr Med [Internet]. 2012 [acesso em 15 out. 2017];28(2):159-72. Disponível em: https://www.sciencedirect.com/ science/article/pii/S074906901200002X?via%3Dihub
174
8. Garske CCD, Assis MP, Schneider APH, Machado EO, Morsch L. Interações medicamentosas
potenciais na farmacoterapia de idosos atendidos em farmácia básica do sul do Brasil. Saúde (Santa Maria) [Internet]. 2016 [acesso em 14 dez. 2017];42(2):97-105. Disponível em: https://periodicos.ufsm.br/ revistasaude/article/view/21751
9. Gotardelo D, Fonseca L, Masson E, Lopes L, Toledo V, Faioli M, et al. Prevalência e fatores associados a potenciais interações medicamentosas entre idosos em um estudo de base populacional. Rev Bras Med Fam Comunidade [Internet]. 2014 [acesso em 22 dez. 2017];9(31):111-8. Disponível em: https://rbmfc.org. br/rbmfc/article/view/833
10. Guthrie B, Makubate B, Hernandez-Santiago V, Dreischulte T. The rising tide of polypharmacy and drug-drug interactions: population database analysis 1995-2010. BMC Med [Internet]. 2015 [acesso em 21 mar. 2018];13(74):1-10. Disponível em: https:// bmcmedicine.biomedcentral.com/articles/10.1186/ s12916-015-0322-7
11. Mibielli P, Rozenfeld S, Matos GC, Acurcio FA. Interações medicamentosas potenciais entre idosos em uso dos anti-hipertensivos da Relação Nacional de Medicamentos Essenciais do Ministério da Saúde do Brasil. Cad Saúde Pública [Internet]. 2014 [acesso em 15 nov. 2017];30(9):1947-56. Disponível em: http://www. scielo.br/scielo.php?script=sci_arttext&pid=S0102-311X2014000901947&lng=pt&tlng=pt
12. Micromedex Healthcare Series [Internet]. Greenwood Village: Thomson Reuters (Healthcare); 2011 [acesso em 21 mar. 2018]. Disponível em: https://www. thomsonhc.com/hcs/librarian/
13. Drug Interactions Checker. Drug Information [Internet]. [sem local]: Dugs.com; 2000- [acesso em 21 mar. 2018 ]. Disponível em: http://www.drugs.com
14. Leão LDF, Moura CS, Medeiros DS. Avaliação de interações medicamentosas potenciais em prescrições da atenção primária de Vitória da Conquista (BA). Ciênc Saúde Coletiva [Internet]. 2014 [acesso em 10 jan. 2018];19(1):311-8. Disponível em: http://www. scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232014000100311&lng=en&nrm=iso&tlng=pt
15. Jacondino CB. Adesão ao tratamento medicamentoso e não medicamentoso em idosos portadores de síndrome metabólica acompanhados na estratégia saúde da família [Dissertação]. Porto Alegre: Pontifícia Universidade Católica do Rio Grande do Sul, Instituto de Geriatria e Gerontologia; 2013.
16. Alverti KG, Zimmet P, Shaw J. Metabolic syndrome: a new world-wide definition. A consensus statement of the International Diabetes Federation. Diabet Med [Internet]. 2006 [acesso em 10 out. 2016];23(5):469-80. Disponível em: https://www.ncbi.nlm.nih.gov/ pubmed/16681555
17. Bertolucci PHF, Brucki SMD, Campacci SR, Juliano Y. O mini exame do estado mental em uma população geral: impacto da escolaridade. Arq Neuropsiquiatr [Internet]. 1994 [acesso em 10 jan. 2016];52(1):1-7. Disponível em: http://www.scielo.br/pdf/anp/ v52n1/01.pdf
18. Ramos LR, Perracini M, Rosa TE, Kalashe A. Significance and management of disability among urban elderly residents in Brazil [abstract]. J Cross-Cult Gerontol [Internet]. 1998 [acesso em 12 jan. 2016];8(4):313-23. Disponível em: https://www.ncbi. nlm.nih.gov/pubmed/24389964
19. Fick D, Semla T, Beizer J, Brandt N, Dombrowski, DuBeau CE, et al. American Geriatrics Society Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. The American Geriatrics Society 2012 Beers Criteria Update Expert Panel. J Am Geriatr Soc [Internet]. 2012 [acesso em 21 mar. 2018];60(4):1-10. Disponível em: https://www. ncbi.nlm.nih.gov/pubmed/22376048
20. Brasil. Resolução n. 466, de 12 de dezembro de 2012. Aprova diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. Diário Oficial da União. 13 jun. 2013. Disponível em: http:// conselho.saude.gov.br/resolucoes/2012/reso466.pdf
21. Levorato CD, Mello LM, Silva AS, Nunes AA. Fatores associados à procura por serviços de saúde numa perspectiva relacional de gênero. Ciênc Saúde Coletiva [Internet]. 2014 [acesso em 10 out. 2017];19(4):1263-74. Disponível em: http://www. scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232014000401263&lng=en&nrm=iso&tlng=pt
22. Leitão MP, Martins IS. Prevalência e fatores associados à síndrome metabólica em usuários de Unidades Básicas de Saúde em São Paulo – SP. Rev Assoc Med Bras [Internet]. 2013 [acesso em 17 dez. 2017];58(1):60 9. Disponível em: http:// www.scielo.br/scielo.php?script=sci_arttext&pid =S0104-42302012000100016
23. Instituto Brasileiro de Geografia e Estatística. Síntese de indicadores sociais- uma análise das condições de vida da população brasileira [Internet]. Rio de Janeiro: IBGE; 2016 [acesso em 21 mar. 2018]. (Estudos e Pesquisas), (Informação Demográfica e Socioeconômica, n. 36). Disponível em: https:// biblioteca.ibge.gov.br/visualizacao/livros/liv98965.pdf
175
25. Saukkonen T, Jokelainen J, Timonen M, Cederberg H, Laakso M, Härkönen P, et al. Prevalence of metabolic syndrome components among the elderly using three different definitions: a cohort study in Finland. Scand J Prim Health Care [Internet]. 2012 [acesso em 12 nov. 2017]:30(1):29-34. Disponível em: https://www.tandfonline.com/doi/full/10.3109/028 13432.2012.654192
26. Tavares NUL, Bertoldi ET, Facchini LA, França GVA, Mengue SS. Fatores associados à baixa adesão ao tratamento medicamentoso em idosos. Rev Saúde Pública [Internet]. 2013 [acesso em 14 nov. 2017];47(6):1092-1101. Disponível em: https://scielosp. org/scielo.php?script=sci_arttext&pid=S0034-89102013000901092&lng=pt&nrm=iso&tlng=pt
27. Cuentro VS, Andrade MA, Gerlack LF, Bós AJG, Silva MVS, Oliveira AF. Prescrições medicamentosas de pacientes atendidos no ambulatório de geriatria de um hospital universitário: estudo transversal descritivo. Ciênc Saúde Coletiva [Internet]. 2014 [acesso em 16 nov. 2017];19(8):3355-64. Disponível em: http://www.scielo.br/scielo.php?pid=S1413-81232014000803355&script=sci_abstract&tlng=pt
28. Neves SJF, Marques APO, Leal MCC, Diniz AS, Medeiros TS, Arruda IKG. Epidemiologia do uso de medicamentos entre idosos em área urbana do Nordeste do Brasil. Rev Saúde Pública [Internet]. 2013 [acesso em 16 nov. 2017];47(4):759-68. Disponível em: http://www. scielo.br/scielo.php?script=sci_arttext&pid =S0034-89102013000400759
29. Monteiro ORB, Figueiredo NR, Marreiros MOC, Figueiredo MLF, Carvalho ADL, Carvalho Júnior JAM. The occurrence of polypharmacy among elderly assisted by the family health strategy. Rev Enferm UFPI [Internet]. 2014 [acesso em 13 nov. 2017];3(2):56-61. Disponível em: http://www.ojs.ufpi. br/index.php/reufpi/article/view/1419/1430
30. Guadagnin AMP, Sgnaolin V. Identificação de problemas relacionados aos medicamentos em idosos atendidos em um laboratório de análise clínicas. PAJAR [Internet]. 2014 [acesso em 10 out. 2017];2(1):23-8. Disponível em: http:// revistaseletronicas.pucrs.br/ojs/index.php/pajar/
31. Santos TRA, Lima DM, Nakatani ADYK, Pereira LV, Leal GS, Amaral RG. Consumo de medicamentos por idosos, Goiânia, Brasil. Rev Saúde Pública [Internet]. 2013 [acesso em 12 set. 2017];47(1):94-103. Disponível em: http://www.scielo.br/scielo.php?script=sci_arttex t&pid=S0034-89102013000100013
32. Jhaveri BN, Patel TK, Barvaliya MJ, Tripathi C. Utilization of potentially inappropriate medications in elderly patients in a tertiary care teaching hospital in India. Perspect Clin Res [Internet]. 2014 [acesso em 10 jan. 2017];5(4):184-9. Disponível em: https://www. ncbi.nlm.nih.gov/pmc/articles/PMC4170537/
33. Pinto N, Vieira L, Pereira F, Reis A, Cassiani S. Interações medicamentosas em prescrições de idosos hipertensos: prevalência e significância clínica. Rev Enferm UERJ [Internet]. 2014 [acesso em 10 set. 2017];22(6):735-41. Disponível em: http://www. epublicacoes.uerj.br/index.php/enfermagemuerj/ article/view/7111
34. Bandeira CAV, Oliveira KR. Potenciais interações entre medicamentos usados na síndrome metabólica. Sci Med [Internet]. 2014 [acesso em 17 nov. 2017];24(2):156-64. Disponível em: http://revistaseletronicas.pucrs.br/ojs/ index.php/scientiamedica
35. Cuentro VS, Modesto T, Andrade MA, Silva MVS. Prevalência e fatores associados à polifarmácia entre idosos de um hospital público. Rev Contexto & Saúde [Internet]. 2016 [acesso em 22 dez. 2017];16(30):28-35. Disponível em: https://revistas.unijui.edu.br/index. php/contextoesaude/article/viewFile/4448/4981