www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Transcanal
endoscopic
myringoplasty:
a
case
series
in
a
university
center
夽
Leandro
de
Borborema
Garcia,
Guilherme
Figner
Moussalem,
José
Santos
Cruz
de
Andrade,
João
Mangussi-Gomes,
Oswaldo
Laércio
Mendonc
¸a
Cruz
∗,
Norma
de
Oliveira
Penido,
José
Ricardo
Gurgel
Testa
DepartmentofOtorhinolaryngologyandHeadandNeckSurgery,EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo (UNIFESP),SãoPaulo,SP,Brazil
Received23January2015;accepted23May2015 Availableonline6November2015
KEYWORDS
Tympanoplasty; Myringoplasty; Naturalorifice endoscopicsurgery; Middleear
Abstract
Introduction:Transcanalmyringoplastyhastheadvantagesofdemandingloweroperativetime and minimal external incisions. It can be performed using the microscopic or endoscopic approach.Inthelastdecade,theuseofendoscopesinearsurgeryhasincreasedsignificantly. Thistechniquemayallow‘‘aroundthecorner’’visualizationofsmallrecesses,throughnarrow spaces,withouttheaidofcanalplastyinunfavorableearcanals.
Objective: Todescribe acaseseriesoftranscanalendoscopicmyringoplasty performedina universityservice.The characteristics,advantages, anddisadvantagesofthistechniqueare alsodiscussed.
Methods:A caseseriesstudy,basedonthechartreviewofpatients submittedtotranscanal endoscopicmyringoplastyintheperiodfromJanuaryof2012toOctoberof2014.
Results:Datafrom22patientswereanalyzed.Tympanicperforationclosurethreemonthsafter surgerywasobservedin86.4%ofallpatients.Therewasstatisticallysignificantimprovement inpuretoneaveragethresholdsaftersurgery(p<0.001).
Conclusion: Transcanalendoscopicmyringoplastyisafeasible,safe,andeffectiveprocedure; itcanbeanalternativetomicroscopicsurgery.
© 2015Associac¸˜aoBrasileira de Otorrinolaringologiae CirurgiaC´ervico-Facial.Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:GarciaLB,MoussalemGF,deAndradeJSC,Mangussi-GomesJ,CruzOLM,PenidoNO,etal.Transcanalendoscopic
myringoplasty:acaseseriesinauniversitycenter.BrazJOtorhinolaryngol.2016;82:321---5.
∗Correspondingauthor.
E-mail:[email protected](O.L.M.Cruz).
http://dx.doi.org/10.1016/j.bjorl.2015.05.012
PALAVRAS-CHAVE
Timpanoplastia; Miringoplastia; Cirurgiaendoscópica pororifícionatural; Orelhamédia
Miringoplastiaendoscópicatranscanal:sériedecasosemumservic¸ouniversitário
Resumo
Introduc¸ão:Amiringoplastiarealizadaporviatranscanalpossuicomovantagensamaiorrapidez doprocedimentoemenorincisãoexterna,podendoserrealizadacomauxíliodemicroscópio ouendoscópio.Naúltimadécadatemsidoobservadoumaumentodousodeendoscópiosna cirurgia otológica.Essa técnicapodepermitirmelhor visibilizac¸ão deespac¸os encobertose estreitos,semnecessidadecanaloplastiaemmeatosdesfavoráveis.
Objetivo:Descrever uma série de casos de miringoplastia endoscópica transcanal, em um servic¸ouniversitário,discutindosuasparticularidades,vantagensedesvantagens.
Método: Estudodesériedecasos,baseadonarevisãodeprontuáriosdospacientessubmetidosa miringoplastiacomusoexclusivodeendoscópiorígido,noperíododeJaneirode2012aOutubro de2014.
Resultados: Foram analisados os dados de 22 pacientes. Na otoscopia pós-operatória, foi observadofechamento da perfurac¸ãotimpânica em 86,4% dos pacientes, após3 mesesda intervenc¸ão.Paraaamostraestudada,foiobservadamelhorafuncionalestatisticamente sig-nificantedamédiadoslimiarestonais(PTA)apósacirurgia(p<0,001).
Conclusão:Amiringoplastiaendoscópicatranscanaléumprocedimentoseguro,factívele efe-tivo,podendoserrealizadocomoalternativaàcirurgiamicroscópica.
©2015Associac¸˜aoBrasileira deOtorrinolaringologiaeCirurgiaC´ervico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Myringoplasty (tympanoplasty type I)is usually the treat-ment of choice for tympanic perforations, whether or not associated with non-suppurative chronic otitis media (COM).1,2 The surgical goal is the total closure of the
perforation and, secondly, an improvement of auditory thresholds.2,3 Transcanal myringoplasty has advantages:
it demands lower operative time and minimal external incision.2,3Whenperformedwiththeaidofasurgical
micro-scope,thetranscanalproceduredependsonawideexternal auditory canal (EAC) andon a favorable angle for proper observationofallbordersofthetympanicperforation.3
Con-ventionalmyringoplastywithretroauricularincision,withor without canalplasty,is the classic alternative for casesof unfavorableEACintranscanalapproacheswithmicroscope. Inthelastdecade,therehasbeenanincreaseintheuse of endoscopes in otologic surgery, not just as an adjunct method, but exclusively.3,4 This approach has the
poten-tial to allow ‘‘around the corner’’ visualization of small recesses, through narrow spaces, without the need for canalplasty,evenincasesofunfavorableEAC.5,6
The teachingof otologic surgeriesduring the otolaryn-gologist’strainingperiodistraditionallydonewiththeuse ofmicroscopes.Despiterecentreportsofseveralauthors, whodescribe the performance of myringoplasty withthe useofopticalfiber,3,5thereisascarcityofstudiesinBrazil
assessingtheresultsofendoscopictechniquesinthecontext ofuniversityhospitals.
Theaimofthisstudyistodescribeacaseseriesof tran-scanal myringoplasty using a rigid endoscope, evaluating surgical outcomesin a university service. Aspects specifi-callyassociatedwiththeuseofendoscopesinotologyand particularitiesrelated tosurgical teachingwill befurther discussed.
Methods
A case series, cross-sectional historical cohort study was conducted, based on the analysis of medical records of patients submittedtomyringoplastywithexclusive use of rigidendoscopeinauniversityservicewithamedical resi-dencyprograminotorhinolaryngologyfromJanuary2012to October2014.
Allpatientsolderthan12yearswithadiagnosisof non-suppurative, non-cholesteatomatousCOMsequela,orwith traumatic perforationswithout spontaneousresolutionfor more thanthreemonths,wereincluded in thestudy.The diagnosis was based on anamnesis, physical examination, audiometry,andimpedanceaudiometry.
Medical records with incomplete data, without pre-and/or postoperative audiometry, and patients lost to follow-upwereexcludedfromthestudy.
Thesurgerieswereperformedunderhypotensivegeneral anesthesia,withpatientsplacedintheconventionalposition forotologicsurgeryperformedwithamicroscope.Surgical procedures were performed by resident physicians of the third year and/or graduatestudents ofthe otorhinolaryn-gologydepartmentoftheservice.
Cottonpadssoakedinepinephrine1:1000wereplacedin theEACincaseofbleedingthatwouldmakeoperativefield visualizationdifficult.Regardlessofwhichwasthesurgeon’s dominanthandor thelateralityoftheeartobeoperated upon,therigidendoscopewasusedwiththenon-dominant hand andthe instruments (stylus,delicate tissueforceps, andsuctioncannulas)inthedominanthand.
In all cases, the procedure was performed by tran-scanalendoscopic approach. The tympanicreconstruction technique used was inlay tragus cartilage myringoplasty, previously described by other authors,7,8 but adapted for
exclusiveendoscopicapproach.
Initially, the perforation borders were scarified with a straightand/orcurvedtipstylus.Then,theperforationsize wasmeasuredforcorrectpreparationofthecartilagegraft. Atragusfragmentwasobtained,maintainingthe perichon-drium of both sidesof the cartilage. After measurement, thecartilagewasshapedandincisedarounditsperimeter tocreateagrooveallowingthegraftfittingintothe perfo-ration.The graft wasthen positionedandtheperforation wasclosed.
Prophylactic postoperative antibiotic therapy was pre-scribedtoallpatients,usingfirst-generationcephalosporin (cephalexinorcefadroxil),forsevendays.Thepatientswere dischargedonthedayaftertheprocedureandfollowedat regularoutpatientfollow-up.
The following data were collected and analyzed: age, gender, pre-andpostoperativeaudiometry,andpuretone average(PTA)thresholdsat500,1000,and2000Hz.Patients wereexaminedatone,four,and12weekspostoperatively, and the incorporation (or not) of the graft and/or the presence ofresidual perforationwere observed.The final postoperativeaudiometrywascarriedoutbetweentwoand threemonthsaftertheprocedure.
Statistical analyses were performed using SPSS v. 17, Minitabv.16,andExcelOffice2010.Non-parametric tests wereuseddue tothesmall samplesize (<30 individuals). Thehypothesistestsutilizedinthisstudyconsidereda sig-nificanceof5%,i.e.,thenullhypothesiswasrejectedwhen thep-valuewas≤0.05.
The project was submitted to and approved by the ResearchEthicsCommitteeoftheinstitutionoforigin,under No.936.194(CAAE40682114.7.0000.5505).
Results
During the study period, 22 patients were assessed. The meanageofpatientswas32.2±6.0years.Thirteen(59.1%) patientswerefemalesandnine(40.1%)weremales.Asfor the laterality, in 13 (59.0%) patients the perforation was locatedonthe left,in eight(36.3%)patients the perfora-tionwaslocatedontheright, andone(4.5%) patienthad bilateralperforations.
Mostpatientswereundergoingsurgeryforthefirsttime; patientsundergoingreoperationaccountedfor9.1%ofcases (n=2).Therewerenocasesthatrequiredsurgical conver-siontoretroauricularapproachoruseofthemicroscopein thisseries.
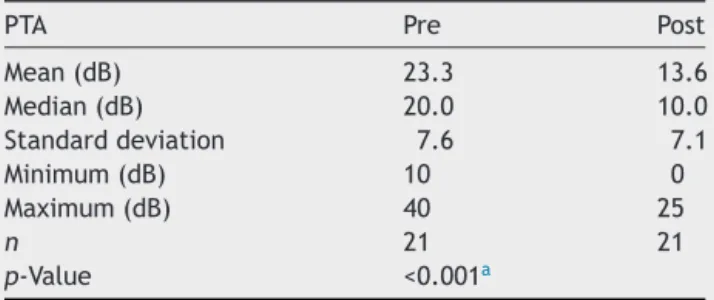
Audiometrically, an improvement in the pure tone average(PTA)hearingthresholdswasobservedfromthe pre-operativetothepostoperativeperiod(Table1andFig.1).
Table1 Descriptivecomparisonbetweenpre-and postop-erativePTAvalues.
PTA Pre Post
Mean(dB) 23.3 13.6
Median(dB) 20.0 10.0
Standarddeviation 7.6 7.1
Minimum(dB) 10 0
Maximum(dB) 40 25
n 21 21
p-Value <0.001a
PTA,puretoneaverage---averageauditorythresholdsat500, 1000,and2000Hz;Pre,pre-operativePTA;Post,post-operative PTA.
a Statisticallysignificantdifference.
0 5 10 15 20 25 30 35 40 45
Pre-Op Post-Op
PTA Pre-Op and Post-Op
*
Figure1 Comparison betweenPTA valuesindecibels(dB),
pre-and post-operatively(n=21).PTA: puretone average ---averageauditorythresholdsat500,1000,and2000Hz;Pre-Op, pre-operative;Post-Op,post-operative.*Statisticallysignificant difference.
Thisdifferencewasstatisticallysignificant(p<0.001).One ofthepatientshadpreandpostoperativeanacusis;this sub-jectwasexcludedfromPTAcalculation(n=21).
As for thesurgical outcome at postoperative otoscopy, completeclosureoftheperforationwasobservedin86.4% (n=19)ofpatientsthreemonthsafterintervention.
Discussion
The present study assessed the feasibility and surgical outcomesof 22 transcanalendoscopic myringoplasty pro-ceduresusingtraguscartilage,inauniversityservice with aresidencyprograminotorhinolaryngology.Theprocedure provedtobeapossiblealternativetomyringoplastyunder microscopic visualization, considering the surgical results (perforation closure) and the proportion of audiometric improvementatthreemonthsoffollow-up.
COM is a heterogeneous disease, with a wide, varied clinical and pathological spectrum. This heterogeneity is apparently determined by the combination of different cytokinesandinflammatorymediators.9Innon-suppurative,
outcomes tend to be good, regardless of the surgical techniqueemployed,andarenotdramaticallyaffectedby changes in the surgical visualization mode, providing the basic technicalprinciplesaremaintained. Infact, studies show that hearing threshold improvement after myringo-plasty essentially depends on graft incorporation to the tympanicmembrane, the integrityof the ossicular chain, theabsenceofresidualperforation,andgraftlateralization ormedialization.Therefore,theapproach,whetheritisthe traditional microscopic or the endoscopic method, would havelittleinfluenceonfunctionalandsurgicaloutcomes.10
Fordecades theuse of endoscopes in otology was pri-marilyfor anatomicalstudiesofthemiddleearandusein humanswaslimited,tosimpleobservationsofthetympanic cavity from pre-existing perforations or as an adjunctive methodtoaidtraditionalmicroscopicprocedures.4,11
How-ever,inthelasttwodecadesithasbeenusedasanexclusive technique for otologic surgery in procedures classically performedonly withamicroscopeincluding: myringoplas-ties,ossiculoplasties,stapedotomies,andsurgeriestotreat
COM.11---13 The exploration of covered recesses, which are
difficult to visualize microscopically --- such as the tym-panicsinus,theprotympanum,andtheanteriorepitympanic recess--- isfacilitatedbytheuseofendoscope.4,14
In a study comparing endoscopic with microscopic myringoplasty, Dündar et al. evaluated 60 pediatric patientsundergoingtype1tympanoplasty usinga condro-perichondralgraft,reportingadecreaseintheair-bonegap inbothgroupsandgraftincorporationrateof87.5%(28of 32patientsintheendoscopicgroup).15Thisrateissimilarto
thatfound inthepresent study(86.4%).The sameauthors found no statistically significant differences between the groups regardingthe audiometric gainand/or graft incor-poration.However,a shorteroperative timewasreported withthe use of the endoscope.15 Ayache et al., in turn,
reportedasuccessrateof96%forcartilagegraft incorpora-tion,placedwiththeaidoftherigidendoscope,considering theprocedureasminimallyinvasive,safe,andeffective.3
The microscope characteristically allows a broad and excellent image quality, with a direct and stereoscopic visualization.10 However,thereareinherent limitations to
theequipment,suchas:decreaseofbrightnessproportional tothemagnification;limitationofthesurgicalfield-of-view, especiallyinnarrowspacessuchastheEACandthemiddle ear.Endoscopes,inturn,providein-depthimagesinnarrow recesses,whilemaintainingbrightnessandallowing differ-entvisualizationangles.6
Disadvantages associated with the endoscope involve working with only one hand and the absence of stereo-scopicview,whichmanyauthorsconsidercrucialforotologic surgery.4,6,11,14Othercriticismsofendoscopeuseinotologic
surgeryrefertothedelicatenatureofthesurrounding struc-tures,withpotentialriskofmechanicalandthermaltrauma, andthe space conflict in the surgical fieldbetween opti-calfiberandthesurgicalinstrument.Thelearningcurveis anotherdetermining factor of surgical outcomeswiththe useofendoscopes,asobservedinsinonasalandskullbase surgery.16
Thisstudyhastheintentiontodescribetheinitialsurgical outcomesofauniversityservicewitharesidencyprogram inrelation toanew techniquein otology.However,there arelimitations. Duetomaterials unavailability,the 4-mm
diameter,0◦ angle, 18-cmlong endoscope(usuallyusedin sinonasalendoscopicsurgery)wastheonlyoneused. Unfor-tunately,itwasnotpossibletouseopticalfibersofdifferent angles,diameters,and/or lengthsfor comparisonsofeasy handlingoftheinstrumentalandvisualizationofthesurgical field.
Therewasnoneedforsurgicalconversiontothe retroau-ricularapproachormicroscopeuse,orotherintraoperative complicationsinanyofthestudiedcases.However,further studieswithlargersamplesofpatientsareneededforproper comparison ofthese twotympanicmembrane reconstruc-tiontechniques.
Conclusion
Transcanalendoscopicmyringoplastyisasafeandfeasible procedure, withgood success rates for tympanic perfora-tionclosure andrecovery ofhearing thresholds.It canbe performedandtaughtinacademicserviceswitharesidency programinotorhinolaryngology,inadditiontoconventional surgeryusingamicroscope.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.TawabA,GharibF,ElSharkawyL,AlgarfT.Myringoplastywith and without cortical mastoidectomy in treatment of non-cholesteatomatouschronicotitismedia:acomparativestudy. ClinMedInsightsEarNoseThroat.2014;7:19---23.
2.HongP,BanceM,GratzerPF.Repairoftympanicmembrane per-forationusingnoveladjuvanttherapies:acontemporaryreview ofexperimentaland tissueengineeringstudies.IntJPediatr Otorhinolaryngol.2013;77:3---12.
3.Ayache S. Cartilaginous myringoplasty: the endoscopic tran-scanal procedure. Eur Arch Otorhinolaryngol. 2013;270: 853---60.
4.Marchioni D, Molteni G, Presutti L. Endoscopic anatomy of the middle ear. Indian J Otolaryngol Head Neck Surg. 2011;63:101---13.
5.FurukawaT,WatanabeT,ItoT,KubotaT,KakehataS.Feasibility andadvantages oftranscanalendoscopicmyringoplasty.Otol Neurotol.2014;35:e140---5.
6.KarchierEB,NiemczykK,OrłowskiA.Comparisonof visualiza-tionofthemiddleear bymicroscopeand endoscopesof30◦ and45◦throughposteriortympanotomy.VideosurgMiniinvasive Tech.2014;9:276---81.
7.EaveyRD.Inlaytympanoplasty:cartilagebutterflytechnique. Laryngoscope.1998;108:657---61.
8.MendesNetoJA,NeivaFC,BrodskynF,PalumboM,BittarACV, PetrilliRNB,et al. Plugcartilagetympanoplasty in children. BrazJOtorhinolaryngol.2008;74:890---5.
9.JuhnSK,JungM-K,HoffmanMD,DrewBR,PreciadoDA,Sausen NJ,etal.Theroleofinflammatorymediatorsinthe pathogen-esisofotitismediaand sequelae.ClinExpOtorhinolaryngol. 2008;1:117.
10.LadeH,ChoudharySR,VashishthA.Endoscopicvsmicroscopic myringoplasty:adifferentperspective.EurArch Otorhinolaryn-gol.2014;271:1897---902.
12.MohindraS,PandaNK. Earsurgery withoutmicroscope: isit possible?IndianJOtolaryngolHeadNeckSurg.2010;62:138---41.
13.JúniorJFN, MartinsMJB, Aguiar CV,PinheiroAI. Fully endo-scopicstapessurgery(stapedotomy):techniqueandpreliminary results.BrazJOtorhinolaryngol.2011;77:721---7.
14.PollakN, Azadarmaki R, Ahmad S. Feasibilityof endoscopic treatmentofmiddleear myoclonus: a cadaveric study.ISRN Otolaryngol.2014:175268.
15.Dündar R, Kulduk E, Soy FK, Aslan M, Hanci D, Muluk NB, et al. Endoscopic versus microscopic approach to type 1 tympanoplasty in children. Int J Pediatr Otorhinolaryngol. 2014;78:1084---9.