Novos achados comparativos de biomicroscopia ultra-sônica entre olhos
contralaterais com fechamento angular agudo e olhos glaucomatosos
com ângulo estreito
Trabalho realizado no Serviço de Glaucoma do Hospi-tal São Geraldo (HospiHospi-tal das Clínicas) da Faculdade de Medicina da Universidade Federal de Minas Gerais -UFMG - Belo Horizonte (MG) - Brasil.
1Pós-graduando, nível doutorado, da Faculdade de Me-dicina da Universidade Federal de Minas Gerais - UFMG - Belo Horizonte (MG) - Brasil.
2Livre-docente, Professor Titular da Disciplina de Oftal-mologia da Faculdade de Medicina da UFMG - Belo Horizonte (MG) - Brasil.
3Pós-graduando, nível doutorado, da Faculdade de Me-dicina da UFMG - Belo Horizonte (MG) - Brasil. 4Livre-docente, Professor Titular da Disciplina de
Oftal-mologia da Faculdade de Medicina da UFMG - Belo Horizonte (MG) - Brasil.
Endereço para correspondência: Rafael Vidal Mérula. Rua Espírito Santo, 1.315 - Apto. 402 - Juiz de Fora (MG) CEP 36016-200
E-mail: [email protected] Recebido para publicação em 28.07.2008 Aprovação em 29.10.2008
Rafael Vidal Mérula1 Sebastião Cronemberger2 Alberto Diniz Filho3 Nassim Calixto4
findings between fellow eyes of acute angle closure
and glaucomatous eyes with narrow angle
Keywords: Eye/anatomy & histology; Microscopy/methods; Ultrasonography/methods;
Biometry; Anterior chamber/anatomy & histology; Anterior chamber/ultrasonography; An-terior eye segment/anatomy & histology; AnAn-terior eye segment/ultrasonography
Purpose: To compare morphometric features between fellow acute primary
angle-closure (APAC) eyes and glaucomatous or suspect eyes with narrow angle (NA). Methods: Fellow eyes of 30 patients with unilateral APAC and 30 with NA were evaluated by ultrasound biomicroscopy (UBM) under light and dark conditions. UBM parameters such as anterior chamber depth (ACD), angle opening distance at 250 µm/500 µm from the scleral spur (AOD250/AOD500), trabecular ciliary process distance (TCPD) and iris-lens contact distance (ILCD) were measured in the superior (SQ) and inferior (IQ) quadrants. Results: Significant differences between APAC fellow and NA eyes were found in ACD, P<0.001; AOD250 at SQ and IQ, P<0.001; AOD500 at SQ and IQ, P<0.001; TCPD light, P=0.010 and TCPD dark at SQ, P=0.031; and TCPD light at IQ, P=0.010. Significant differences between light and dark examinations of APAC fellow eyes were found in ILCD (P=0.009) at SQ and ILCD at IQ (P=0.006), and of NA eyes in ILCD at SQ (P=0.047) and ILCD at IQ (P<0.001). Conclusions: APAC fellow eyes have a more crowded anterior segment and shallower ACD than NA eyes. ILCD decreases in both groups when the illumination conditions change from light to dark.
ABSTRACT
INTRODUCTION
The most common mechanism in the development of acute primary angle closure (APAC) is an increased resistance caused by relative pupil-lary block, preventing the aqueous from flowing through the pupil(1-2). A
laser peripheral iridotomy (LPI) would relieve this block and open the angle. Eyes with angle closure have important biometric differences from healthy eyes, such as a shallower anterior chamber, a thicker lens, and a shorter axial length(3). Ultrasound biomicroscopy (UBM) permits
noninva-sive examination of the anterior segment at high resolution (40 µm)(4). The
efficacy of UBM has been demonstrated in relation to the mechanism of angle closure in eyes with primary angle closure glaucoma (PACG)(5), and
the morphologic changes after laser iridotomy(6).
suspect characteristics of primary open-angle glaucoma (POAG) with narrow angle (NA) and fellow eyes of APAC patients.
METHODS
This was a prospective comparative observational case se-ries. Patients with APAC and NA were consecutively recruited from the Glaucoma Service of São Geraldo Hospital/Federal University of Minas Gerais from September 2005 to June 2007. The study was carried out after approval by the Federal Uni-versity of Minas Gerais Research Ethics Committee. Informed consent was obtained from all the participants. The following criteria were used to define APAC cases: 1) presence of at least two of the following symptoms: ocular or periocular pain, nau-sea and/or vomiting, antecedent history of intermittent blurring of vision with halos; and 2) presenting intraocular pressure (IOP) of more than 28 mmHg (Goldmann applanation tonometry) and the presence of at least three of the following signs: con-junctival injection, corneal epithelial edema, mid-dilated no reactive pupil, and shallow anterior chamber; and 3) the pre-sence of an occluded angle in the affected eye (gonioscopy). The enrollment criteria for the fellow group were: 1) contra-lateral eyes of patients who had developed APAC; 2) narrow angle; 3) no previous ocular surgery or laser therapy; 4) no medications in use that affect pupillary reactions or diameter; 5) no abnormalities in cornea and iris; 6) no signs of secondary angle closure glaucoma; 7) no signs of plateau iris configura-tion (PIC) (the diagnosis of PIC requires normal central anterior chamber depth (ACD), peripheral iris anteriorly and centrally angled, and a flat or slightly convex iris by biomicroscopy, narrow angle under gonioscopic examination and the sign of double hump with the indentation gonioscopy. To confirm the diagnosis of PIC, the UBM examination shows the ciliary pro-cesses anteriorly located, closing the ciliary sulcus, and provi-ding structural support behind the peripheral iris; 8) IOP that did not exceed 20 mmHg; and 9) no nuclear sclerosis defined as Lens Opacities Classification System (LOCS) II less than grade 2 (NC2, NO2)(7). Once the acute attack was broken, the fellow
eye was evaluated clinically and by UBM. The group of NA was composed of patients with the diagnosis or suspect charac-teristics of POAG with NA. The criteria used to define POAG with NA were: 1) IOP higher than 21 mmHg; and 2) presence of glaucomatous optic neuropathy defined by at least two of the following items, cup/disc ratio (C/D) asymmetry between fellow eyes greater than 0.2, rim thinning, notching, C/D equal or more than 0.7, optic disc haemorrhage or retinal nerve fiber layer defect; and 3) glaucomatous visual field defects by automated perimetry (Octopus 1-2-3). The visual field was considered ab-normal if two of the following three criteria were met on at least two consecutive examinations: (a) an abnormal Bebbie curve (deviation more than 0.0); (b) 3 contiguous nonedge points (allowing the two nasal step edge points) on a Octopus pro-gram G1 visual field with P<0.05 on the probability plot, with at least 1 point at P<0.01; and (c) a corrected loss variance
P<0.05); and 4) narrow angle on gonioscopy. The criteria used
to define eyes with suspect characteristics of POAG with NA were: the presence of the item 4, and the presence of aforementioned item 1 or 2 to define POAG with NA; however, the definition of item 2 was modified here (presence of one of the characteristics described above to define glaucomatous optic neuropathy). Exclusion criteria for NA were: nuclear sclerosis defined as LOCS II more than grade 2 (NC2, NO2) in both eyes; secondary glaucoma; PIC; signs of previous glaucoma crisis; corneal opacity in both eyes; necessity of surgical procedure to control IOP; previous surgical procedure in both eyes; and closed angle under dark gonioscopic exami-nation. If one or more than one of the exclusion criteria for NA were identified in one eye, the other eye was evaluated clinically and by UBM before beginning the medication. If no exclusion criteria were found, the right eye was preferably evaluated. Clinical examination consisted of history, visual acuity with and without optical correction, biomicroscopy, gonioscopy and C/D examination. Gonioscopy was done by one of the authors (RVM) and confirmed by another investi-gator (SC), using a Goldmann 3 mirror goniolens (Volk Optical Inc, Mentor, Ohio, USA), and afterwards, a Zeiss 4-mirror go-niolens (Carl Zeiss Meditec AG, Oberkochen, Germany) for indentation gonioscopy, in the undilated state under room light illumination (approximately 240 lux), and dark (appro-ximately 0.1 lux) (the room was darkened in 5 minutes), both conditions previously measured with an illuminance meter [Minolta T10 Illuminance Meter, Konica Minolta Sensing Inc., Osaka, Japan]), the conditions being uniform for the whole examination. The gonioscopy classification currently used by the Glaucoma Service, both in primary gaze and under inden-tation, was adopted for this study and applied under room light illumination: 1) wide open angle (angle totally open); 2) interme-diate open angle (when it was possible to see until scleral spur, but it was not possible to identify the ciliary band); 3) narrow open angle (when it was only possible to identify the anterior part of the trabecular meshwork); 4) closed angle (it was not possible to identify any structure). The angle was fully gonios-copically evaluated (360°), and the widest quadrant was adop-ted to label the angle of each eye.
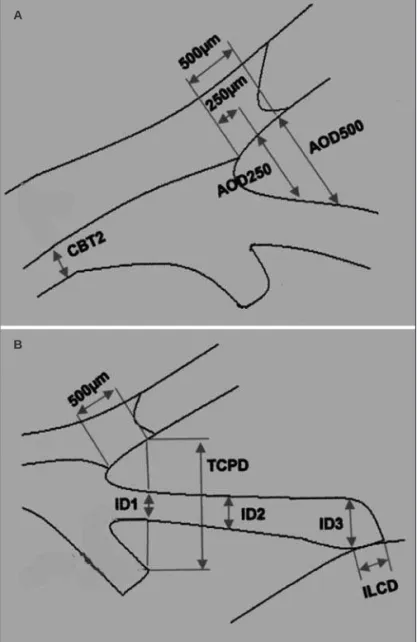
clear and representative images per quadrant of the angle of each eye were selected for further analysis. The various parameters listed below were measured by a single observer (RVM) to rule out interobserver variability(8) on the images of
the superior and inferior quadrants (SQ and IQ) using previously published methodology(9) (Figure 1).
1. The central ACD, measured on a line extending from the corneal endothelium to the anterior lens surface perpen-dicularly to both mentioned anatomical structures.
2. The angle opening distance (AOD250) is the distance between the posterior corneal surface and the anterior iris surface measured on a line perpendicular to the trabecular meshwork, 250 µm from the scleral spur (Figure 1A).
3. The angle opening distance (AOD500) is the same as AOD250, however, 500 µm from the scleral spur (Figure 1A).
4. The trabecular ciliary process distance (TCPD), measured on a line extending from the corneal endothelium at 500 µm from the scleral spur perpendicularly through the iris to the ciliary processes (Figure 1B).
5. The iris thickness 1 (ID1), the iris thickness measured along the same line as the TCPD (Figure 1B).
6. Iris thickness 2 (ID2), the iris thickness 2 mm from the iris root (Figure 1B).
7. Iris thickness 3 (ID3), the maximum iris thickness near the pupillary edge (Figure 1B).
8. Ciliary body thickness 2 (CBT2), the ciliary body thick-ness measured at 2 mm from scleral spur (Figure 1A).
9. The iris-lens contact distance (ILCD), measured along the iris pigmented epithelium from the pupillary border to the point where the anterior lens surface leaves the iris (Figure 1B). Statistical analyses were performed using 13.0 SPSS. We have used frequency histograms and the following tests: one-sample Kolmogorov-Smirnov, Student’s t, paired Student’s t, Mann-Whitney U, Wilcoxon and Pearson’s chi-square. A P value of less than 0.05 was considered statistically significant.
RESULTS
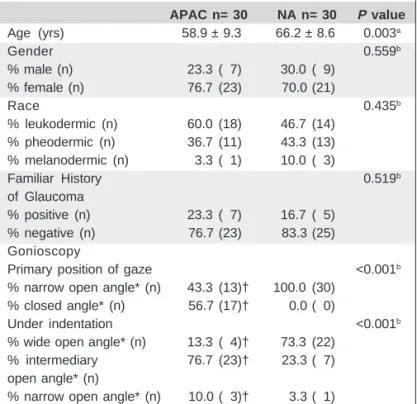
Table 1 shows the demographic features of the 60 studied subjects. We assessed 30 fellow APAC eyes and 30 NA eyes. Twenty-one (70%) patients of the NA group had the diagno-sis of POAG with narrow angle and 9 (30%) suspect characte-ristics. NA patients were older than APAC patients (P=0.003), however, no difference was found between the two groups when gender (P=0.559), race (P=0.435) and history of glaucoma (P=0.519) were compared. The statistical difference of gonios-copic classification was evident between groups (P<0.001).
Table 2 shows the UBM parameters in APAC fellow eyes and NA eyes. Significant differences between APAC fellow and NA eyes were found in the ACD light (P<0.001), ACD dark (P<0.001), AOD250 at SQ light (P<0.001), AOD250 at SQ dark (P=0.001), AOD500 at SQ light (P<0.001), AOD500 at SQ dark (P<0.001), TCPD at SQ light (P=0.010), TCPD at SQ dark (P=0.031), ID3 at SQ dark (P=0.035), AOD250 at IQ light (P<0.001), AOD250 at IQ dark (P<0.001), AOD500 at IQ light (P<0.001), AOD500 at IQ dark (P<0.001) and TCPD at IQ light (P=0.010).
Table 3 shows the comparison between light and dark UBM measurements of APAC fellow and NA eyes. Significant dif-ferences between light and dark examinations of APAC fellow eyes were found in the ILCD at SQ (P=0.009) and ILCD at IQ (P=0.006); and between light and dark measurements of NA eyes were found in ID1 at SQ (P=0.008), ID2 at SQ (P=0.017), ILCD at SQ (P=0.047) and ILCD at IQ (P<0.001).
DISCUSSION
To the best of our knowledge, this is the first study that compared eleven UBM measurements between APAC fellow and NA eyes. Except for the age, both groups had similar demogra-phic characteristics. The APAC patients had a mean age of 58.9 ± 9.3 years which was lower than that of the NA
B A
patients (66.2 ± 8.6 years) (P=0.003). This difference could be considered a limitation of this study owing to the fact that some changes in the structure of the eye occur when people get old(10). However, the differences in the anatomical features
between the 6th and 7th decades, which are the decades of the
majority of patients included in this study, are not so signi-ficant(10-11).
It has already been reported that fellow eyes of acute PACG have different topologic features and a higher inciden-ce of appositional angle closure than normotensive narrow-angled eyes(12). Our UBM data demonstrated quite clearly
that APAC fellow eyes are characterized by a more crowded anterior segment and a shallower ACD compared to NA eyes (Table 2). A shallower ACD in eyes with angle closure has already been reported previously, not only in biometric stu-dies that compared these eyes with normal subjects(13-14), or
with narrow angles(15), or with occludable angles(16), or with
POAG(17), but also in UBM studies that compared angle closure
eyes with normal subjects(18-19). Subgroups of studied primary
angle closure glaucoma using UBM(18) presented a shallower
ACD in the acute/intermittent form when compared to the chronic form.
The TCPD is a parameter of primary importance since it indicates the gap available for the iris between the trabecular meshwork and the ciliary process(9). In this series, TCPD
va-lues were higher in NA eyes compared to APAC fellow eyes, in light or dark conditions (Table 2). However, no significant difference was detected regarding ID1 (Table 2). These diffe-rences in TCPD have an effect on the AOD250 and AOD500,
which were particularly short in APAC eyes (Table 2). Some studies evaluated the difference of TCPD between PACG and normal eyes in the South Indian population, but in subjects with PACG after LPI(19), between acute/intermittent PACG and
chronic PACG eyes(18), and between primary angle closure
suspects (PACS) and normal eyes(20), and the lower values
were found in PACG, acute/intermittent PACG eyes and PACS, respectively. Some studies verified that contralateral eyes of acute angle closure and PACS eyes had lower values of AOD500 compared to healthy controls(20-21). Marchini et
al.(18) showed statistically significant difference in AOD500
between acute/intermittent and chronic PACG eyes. The pre-sence of a difference in TCPD in APAC fellow eyes compared to NA eyes could give an indication about the pathogenesis of the acute disease in the absence of a considerable opales-cent lens.
For the first time, the iris thickness comparison between APAC fellow and NA eyes is being reported. The thickness of the iris (ID1, ID2 and ID3) was the same as that in APAC fellow eyes and in NA eyes, except for ID3 at SQ in dark conditions that showed marginal significance (P=0.035) with minor difference which could be an incidental situation. Probably, the iris thickness was not responsible for the narro-wing of the angle. No difference in the ID1 between patients with PACG and normal subjects was found in one study(18)
however it was noticed in another study with marginal dif-ference(19). The finding of a thicker iris has been reported in
Eskimos(22). In our study, unexpected findings were verified
when comparison between light and dark examinations of iris thickness in NA group was performed; ID1 at SQ (P=0.008) and ID2 at SQ (P=0.017) were thicker in dark conditions (Table 3); these results were not evident in APAC fellow eyes. Re-garding the CBT2, our data did not show any statistically sig-nificant difference either between the two groups or within the groups between light and dark conditions. Gohdo et al.(23),
found a thinner ciliary body in narrow angle eyes in compari-son to normal control eyes, and suggested that this thinning could be an age-related change.
The APAC fellow group in comparison to the NA group showed no statistically significant difference in the ILCD. However, when this parameter was evaluated between light and dark circumstances it had higher values in light condi-tions (Table 3). Probably, when mid-dilation occurs resul-ting in a pupillary block (simulated by the dark examina-tion), the iris convexity increases according to a shallower ACD and older age(24), and, subsequently, ILCD appears to
decrease. In our study, no difference was found in the iris thickness of the APAC group between light and dark con-ditions (Table 3).
In conclusion, this study demonstrates that APAC fellow eyes have a more crowded anterior segment, especially the entrance of the angle, as well as the decrease of ILCD when the illumination conditions change from light to dark. Lon-gitudinal comparisons are required to further understand the differences in pathology of angle closures.
Table 1. Demographic characteristics of APAC and NA patients
APAC n= 30 NA n= 30 P value
Age (yrs) 58.9 ± 9.3 66.2 ± 8.6 0.003a
Gender 0.559b
% male (n) 23.3 (07) 30.0 (09) % female (n) 76.7 (23) 70.0 (21)
Race 0.435b
% leukodermic (n) 60.0 (18) 46.7 (14) % pheodermic (n) 36.7 (11) 43.3 (13) % melanodermic (n) 3.3 (01) 10.0 (03)
Familiar History 0.519b
of Glaucoma
% positive (n) 23.3 (07) 16.7 (05) % negative (n) 76.7 (23) 83.3 (25) Gonioscopy
Primary position of gaze <0.001b
% narrow open angle* (n) 43.3 (13)† 100.0 (30) % closed angle* (n) 56.7 (17)† 0.0 (00)
Under indentation <0.001b
% wide open angle* (n) 13.3 (04)† 73.3 (22) % intermediary 76.7 (23)† 23.3 (07) open angle* (n)
% narrow open angle* (n) 10.0 (03)† 3.3 (01)
Table 2. Ultrasound biomicroscopy characteristics of APAC-Fellow and NA eyes
APAC-fellow eye n= 30 NA eye n= 30 P value
ACD light (mm) 1.851 ± 0.228 2.206 ± 0.264 < 0.001a
ACD dark (mm) 1.860 ± 0.242 2.197 ± 0.253 < 0.001b
AOD250 at SQ light (mm) 0.007 ± 0.030 0.056 ± 0.066 < 0.001a
AOD250 at SQ dark (mm) 0.003 ± 0.018 0.043 ± 0.067 0.001a
AOD500 at SQ light (mm) 0.003 ± 0.014 0.079 ± 0.078 < 0.001a
AOD500 at SQ dark (mm) 0.006 ± 0.028 0.059 ± 0.065 < 0.001a
TCPD at SQ light (mm) 0.560 ± 0.153 0.669 ± 0.163 0.010b
TCPD at SQ dark (mm) 0.565 ± 0.160 0.651 ± 0.143 0.031b
ID1 at SQ light (mm) 0.321 ± 0.076 0.322 ± 0.065 0.984b
ID1 at SQ dark (mm) 0.340 ± 0.082 0.358 ± 0.074 0.365b
ID2 at SQ light (mm) 0.434 ± 0.103 0.425 ± 0.064 0.669b
ID2 at SQ dark (mm) 0.445 ± 0.114 0.458 ± 0.087 0.625b
CBT2 at SQ light (mm) 0.269 ± 0.056 0.283 ± 0.083 0.706a
CBT2 at SQ dark (mm) 0.271 ± 0.045 0.284 ± 0.085 0.929a
ID3 at SQ light (mm) 0.573 ± 0.113 0.622 ± 0.095 0.073b
ID3 at SQ dark (mm) 0.574 ± 0.121 0.632 ± 0.084 0.035b
ILCD at SQ light (mm) 0.488 ± 0.147 0.494 ± 0.136 0.941a
ILCD at SQ dark (mm) 0.427 ± 0.180 0.444 ± 0.119 0.209a
AOD250 at IQ light (mm) 0.014 ± 0.050 0.061 ± 0.065 < 0.001a
AOD250 at IQ dark (mm) 0.000 ± 0.000 0.062 ± 0.063 < 0.001a
AOD500 at IQ light (mm) 0.026 ± 0.053 0.089 ± 0.069 < 0.001a
AOD500 at IQ dark (mm) 0.017 ± 0.046 0.092 ± 0.089 < 0.001a
TCPD at IQ light (mm) 0.594 ± 0.142 0.673 ± 0.130 0.030b
TCPD at IQ dark (mm) 0.626 ± 0.159 0.677 ± 0.136 0.182b
ID1 at IQ light (mm) 0.353 ± 0.085 0.352 ± 0.066 0.956b
ID1 at IQ dark (mm) 0.361 ± 0.085 0.348 ± 0.050 0.480b
ID2 at IQ light (mm) 0.432 ± 0.097 0.429 ± 0.069 0.894b
ID2 at IQ dark (mm) 0.439 ± 0.114 0.451 ± 0.088 0.665b
CBT2 at IQ light (mm) 0.283 ± 0.053 0.298 ± 0.083 0.389b
CBT2 at IQ dark (mm) 0.297 ± 0.042 0.312 ± 0.069 0.337b
ID3 at IQ light (mm) 0.510 ± 0.100 0.544 ± 0.112 0.213b
ID3 at IQ dark (mm) 0.525 ± 0.087 0.570 ± 0.094 0.060b
ILCD at IQ light (mm) 0.478 ± 0.120 0.520 ± 0.136 0.267a
ILCD at IQ dark (mm) 0.416 ± 0.101 0.417 ± 0.119 0.967b
Values are means±SD.
APAC= acute primary angle closure; NA= narrow angle eyes; ACD= anterior chamber depth; SQ= superior quadrant (12 o’clock); IQ= inferior quadrant (6 o’clock); AOD250= angle opening distance 250 µm from the scleral spur; AOD500= angle opening distance 500 µm from the scleral spur; TCPD= trabecular ciliary process distance; ID1= iris thickness 1; ID2= iris thickness 2; CBT2= ciliary body thickness 2; ID3= iris thickness 3; ILCD= the iris-lens contact distance; a= Mann Whitney test; b= independent samples Student’s t test
RESUMO
Objetivo: Comparar características morfométricas entre olhos
contralaterais com fechamento angular primário agudo (FAPA) e olhos glaucomatosos ou suspeitos com ângulo estreito (AE).
Métodos: Olhos contralaterais de 30 pacientes com FAPA
unilateral e olhos de 30 pacientes com AE foram avaliados através da biomicroscopia ultra-sônica (BUS) no claro e escu-ro. Parâmetros da BUS como a profundidade central de câmara anterior (PCA), distância da abertura angular a 250 µm/500 µm do esporão escleral (AOD250/AOD500), distância entre o pro-cesso ciliar e o trabeculado (TCPD) e distância do contato iris-cristalino (ILCD) foram medidos nos quadrantes superior (QS) e inferior (QI). Resultados: Diferenças significativas entre olhos contralaterais de FAPA e olhos com AE foram encontradas na
PCA, p<0,001; AOD250 no QS e QI, p<0,001; AOD500 no QS e QI, p<0,001; TCPD no claro, p=0,010 e TCPD no escuro no QS,
p=0,031; e TCPD no claro no QI, p=0,010. Diferenças
significa-tivas entre exames no claro e escuro realizados em olhos con-tralaterais com FAPA foram encontradas na ILCD (p=0,009) no QS e ILCD no QI (p=0,006), e em olhos com SE na ILCD no QS (p=0,047) e ILCD no QI (p<0,001). Conclusões: Olhos contra-laterais de FAPA apresentam um segmento anterior mais aglo-merado e uma PCA menor que olhos com AE. ILCD diminui em ambos os grupos quando as condições de iluminação mu-dam do claro para o escuro.
Descritores: Olho/anatomia & histologia;
anterior/ultra-sonogra-Table 3. Ultrasound biomicroscopy characteristics of APAC-Fellow and NA eyes (light x dark)
APAC-fellow APAC-fellow P NA eye NA P
eye light eye dark value light eye dark value
n= 30 n= 30 n= 30 n= 30
ACD (mm) 1.851 ± 0.228 1.860 ± 0.242 0.510c 2.206 ± 0.264 2.197 ± 0.253 0.416c
AOD250 at SQ (mm) 0.007 ± 0.030 0.003 ± 0.018 0.593c 0.056 ± 0.066 0.043 ± 0.067 0.408c AOD500 at SQ (mm) 0.003 ± 0.014 0.006 ± 0.028 1.000c 0.079 ± 0.078 0.059 ± 0.065 0.131c TCPD at SQ (mm) 0.560 ± 0.153 0.565 ± 0.161 0.851d 0.669 ± 0.163 0.651 ± 0.143 0.502d ICPD at SQ (mm) 0.226 ± 0.100 0.225 ± 0.100 0.837c 0.244 ± 0.120 0.221 ± 0.083 0.171c ID1 at SQ (mm) 0.321 ± 0.076 0.340 ± 0.082 0.166d 0.322 ± 0.065 0.358 ± 0.074 0.008d ID2 at SQ (mm) 0.434 ± 0.103 0.445 ± 0.114 0.424d 0.425 ± 0.064 0.458 ± 0.087 0.017d CBT2 at SQ (mm) 0.269 ± 0.056 0.271 ± 0.045 0.905c 0.283 ± 0.083 0.284 ± 0.085 0.861c ID3 at SQ (mm) 0.573 ± 0.113 0.574 ± 0.121 0.951d 0.622 ± 0.095 0.632 ± 0.084 0.335d ILCD at SQ (mm) 0.488 ± 0.147 0.427 ± 0.180 0.009c 0.494 ± 0.136 0.444 ± 0.119 0.047c AOD250 at IQ (mm) 0.014 ± 0.050 0.000 ± 0.000 0.109c 0.061 ± 0.065 0.062 ± 0.063 0.835c AOD500 at IQ (mm) 0.026 ± 0.053 0.017 ± 0.046 0.374c 0.089 ± 0.069 0.092 ± 0.089 0.988c TCPD at IQ (mm) 0.594 ± 0.142 0.626 ± 0.159 0.187d 0.673 ± 0.130 0.677 ± 0.136 0.843d ID1 at IQ (mm) 0.353 ± 0.085 0.361 ± 0.085 0.592d 0.352 ± 0.066 0.348 ± 0.050 0.777d ID2 at IQ (mm) 0.432 ± 0.097 0.439 ± 0.114 0.608d 0.429 ± 0.069 0.451 ± 0.088 0.142d CBT2 at IQ (mm) 0.283 ± 0.053 0.297 ± 0.042 0.155d 0.298 ± 0.083 0.312 ± 0.069 0.277d ID3 at IQ (mm) 0.510 ± 0.100 0.525 ± 0.087 0.290d 0.544 ± 0.112 0.570 ± 0.094 0.067d ILCD at IQ (mm) 0.478 ± 0.120 0.416 ± 0.101 0.006c 0.520 ± 0.136 0.417 ± 0.119 <0.001c
Values are means±SD.
APAC= acute primary angle closure; NA= narrow angle eyes; ACD= anterior chamber depth; SQ= superior quadrant (12 o’clock); IQ= inferior quadrant (6 o’clock); AOD250= angle opening distance 250 µm from the scleral spur; AOD500= angle opening distance 500 µm from the scleral spur; TCPD= trabecular ciliary process distance; ID1= iris thickness 1; ID2= iris thickness 2; CBT2= ciliary body thickness 2; ID3= iris thickness 3; ILCD= the iris-lens contact distance; c= Wilcoxon test; d= paired Student’s t test
fia; Segmento anterior do olho/anatomia & histologia; Seg-mento anterior do olho/ultra-sonografia
REFERENCES
1. Barkan O. Glaucoma: classification, causes, and surgical control. Results of microgonioscopic research. Am J Ophthalmol. 1938;21:1099-117. 2. Sugar HS. Newer concepts in classification of glaucomas. Am J Ophthalmol.
1949;32(3):425-33.
3. Lowe RF. Primary angle closure glaucoma: a review of ocular biometry. Aust NZ J Ophthalmol. 1977;5:9-17.
4. Pavlin CJ, Sherar MD, Foster FS. Subsurface ultrasound microscopic ima-ging of the intact eye. Ophthalmology. 1990;97(2):244-50.
5. Ritch R, Liebmann JM. Role of ultrasound biomicroscopy in the differentia-tion of block glaucomas. Curr Opin Ophthalmol. 1998;9(2):39-45. 6. Gazzard G, Friedman DS, Devereux JG, Chew P, Seah SK. A prospective
ultrasound biomicroscopy evaluation of changes in anterior segment morpho-logy after laser iridotomy in Asian eyes. Ophthalmomorpho-logy. 2003;110(3):630-8. 7. Chylack LT Jr, Leske MC, McCarthy D, Khu P, Kashinagi T, Sperduto R. Lens
opacities classification system II (LOCS II). Arch Ophtahlmol. 1989;107(7):991-7. 8. Tello C, Liebmann J, Potash SD, Cohen H, Ritch R. Measurement of ultra-sound biomicroscopy images: intraobserver and interobserver reliability. Invest Ophthalmol Vis Sci. 1994;35(9):3549-52.
9. Pavlin CJ, Harasiewicz K, Foster FS. Ultrasound biomicroscopy of anterior segment structures in normal and glaucomatous eyes. Am J Ophthalmol. 1992; 113(4):381-9.
10. Lim KJ, Hyung SM, Youn DH. Ocular dimensions with aging in normal eyes. Korean J Ophthalmol. 1992;6(1):19-31.
11. Markowitz SN, Morin JD. Angle closure glaucoma: relation between lens thickness, anterior chamber depth and age. Can J Ophthalmol. 1984;19(7):300-2. 12. Sawada A, Sakuma T, Yamamoto T, Kitazawa Y. Appositional angle closure in eyes with narrow angles: comparison between the fellow eyes of acute angle closure glaucoma and normotensive cases. J Glaucoma. 1997;6(5):288-92.
13. Saxena S, Agrawal PK, Pratap VB, Nath R. Anterior chamber depth and lens thickness in primary angle closure glaucoma: a case-control study. Indian J Ophthalmol. 1993;41(2):71-3.
14. Sihota R, Gupta V, Agarwal HC, Pandey RM, Deepak KK. Comparison of symptomatic and asymptomatic, chronic, primary angle closure glaucoma, open-angle glaucoma, and controls. J Glaucoma. 2000;9(3):208-13. 15. Lee DA, Brubaker RF, Illstrup DM. Anterior chamber dimensions in patients
with narrow angles and angle closure glaucoma. Arch Ophthalmol. 1984; 102(1):46-50.
16. George R, Paul PG, Baskaran M, Ramesh SV, Raju P, Arvind H, et al. Ocular biometry in occludable angles and angle closure glaucoma: a population based survey. Br J Ophthalmol. 2003;87(4):399-402.
17. Calixto N, Cronemberger S. Glaucoma simples x glaucoma agudo: estudo eco-biométrico. Arq Bras Oftalmol. 1986;49(1):1-8.
18. Marchini G, Pagliarusco A, Toscano A, Tosi R, Brunelli C, Bonomi L. Ultra-sound biomicroscopic and conventional ultrasonographic study of ocular dimensions in primary angle closure glaucoma. Ophthalmology. 1998;105(11):2091-8. 19. Garudadri CS, Chelerkar V, Nutheti R. An ultrasound biomicroscopic study of
the anterior segment in Indian eyes with primary angle closure glaucoma. J Glaucoma. 2002;11(6):502-7.
20. Ramani KK, Mani B, Ronnie G, Joseph R, Lingam V. Gender variation in ocular biometry and ultrasound biomicroscopy of primary angle closure sus-pects and normal eyes. J Glaucoma. 2007;16(1):122-8.
21. Friedman DS, Gazzard G, Foster P, Devereux J, Broman A, Quigley H, et al. Ultrasonographic biomicroscopy, Scheimpflug photography, and novel provo-cative tests in contralateral eyes of Chinese patients initially seen with acute angle closure. Arch Ophthalmol. 2003;121(5):633-42.
22. Alsbirk PH. Primary angle closure glaucoma. Oculometry, epidemiology, and genetics in a high risk population. Acta Ophthalmol Suppl. 1976;(127):5-31. 23. Gohdo T, Tsumura T, Iijima H, Kashiwagi K, Tsukahara S. Ultrasound bio-microscopic study of ciliary body thickness in eyes with narrow angles. Am J Ophthalmol. 2000;129(3):342-6.