w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Case
Report
Gastrointestinal
stromal
tumor
of
rectum
diagnosed
by
three-dimensional
anorectal
ultrasound
夽
Raphael
Ferreira
Ratin
a,∗,
Suelen
Melão
a,
Doryane
Maria
dos
Reis
Lima
b,
Univaldo
Etsuo
Sagae
b,
Gustavo
Kurachi
baHospitalSãoLucas,FaculdadeAssisGurgacz(FAG),Cascavel,PR,Brazil
bAnorectalPhysiologySector,GastroclínicaCascavel,Cascavel,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14February2014 Accepted3March2015
Availableonline20December2015
Keywords:
Gastrointestinalstromaltumor CD34
CD117
a
b
s
t
r
a
c
t
Gastrointestinalstromaltumors(GIST)arerelativelyrarelesionsofmesenchymalorigin, beingmorefrequentinthestomachandsmallintestine.Theseareclinicallyasymptomatic lesions,andinadvancedstagesmaypresentwithnausea,vomiting,bleeding,abdominal pain,apalpablemass,andevenintestinalobstruction.Theonlyeffectivetreatmentconsists ofacompletetumorresection.WereporttwocasesofGISTlocatedinthedistalrectumand evaluatedwiththree-dimensionalanorectalultrasonography,aprocedureofgreatvaluein identifyingthesizeofthelesion,itsinvolvementtowardnearbystructuresandlymphnode invasion.
©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
Tumor
estromal
gastrointestinal
de
reto
diagnosticado
por
ultra-sonografia
anorretal
tridimensional
Palavras-chave:
Tumorestromalgastrointestinal CD34
CD117
r
e
s
u
m
o
Ostumoresestromaisdotratogastrointestinal(GIST)sãolesõesrelativamenterarasde origemmesenquimal,sendomaisfrequentesnoestômagoeintestinodelgado. Clinica-mente, são lesõesassintomáticas eem estados avanc¸adospodem cursarcomnáusea, vômito,sangramento,dorabdominal,massapalpáveleatéobstruc¸ãointestinal.Oúnico tratamento efetivo é a ressecc¸ão completa do tumor. Relatamos dois casos de GIST
夽
StudylinkedtotheDepartmentofGeneralSurgery,HospitalSãoLucas,FaculdadeAssisGurgacz(FAG),Cascavel,PR,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.F.Ratin).
http://dx.doi.org/10.1016/j.jcol.2015.03.003
(25–35%),colonandrectum(5–10%),andesophagus(<5%). With an incidence estimated at 10–20 cases/10 million inhabitants,4 GIST represents about 0.6% of all malignant
rectaltumors,5comprisingonly1–3%ofallcancersofthe
gas-trointestinaltract.Itsrelevancestemsfromthefactthatthey represent80%ofallprimarytumorsofthegastrointestinal tract.6,7 Thelargestnumberofcasesoccursinolderadults,
especiallybetweenthefourthtosixthdecadeoflife.8Thereis
noprevalenceingender.8
Clinical manifestations of GIST are related to its loca-tion,whichcanbemultiple,anditsdimensions.9 Clinically,
theseare asymptomaticlesions,and inanadvanced state, there may be nausea, vomiting, bleeding, abdominal pain, apalpable mass, and even intestinalobstruction.9–11 Tests
suchasabdominalultrasound,uppergastrointestinal(UGI) endoscopy,colonoscopy,echoendoscopy,computed tomogra-phy(CT)andnuclearmagneticresonance(NMR)areimaging methodsimportantfortheinvestigationofinjury.9Theonly
effective treatment is surgical resection.10 Anorectal
ultra-sonography (USG-A) is indicated in benign and malignant anorectal diseases, including anal incontinence, infectious and inflammatory diseases (abscesses, anorectal fistulae), chronicanorectalpain(endometriosis),andinthestagingand follow-upofanorectalneoplasms.12–14Thus,USG-Aallowsfor
theevaluation ofanatomical structuresthatformthe anal canal,rectumandperi-anorectaltissueswithlowcostandin asafemanner,becausethisisaverylittleinvasivetest,being welltoleratedandwhichdoesnotexposepatientsto radia-tion.Thus,USG-Ahasbecomeacriticalimagingmodalityfor clinicaldiagnosis ofGISTanditsdifferentiation fromother submucosalneoplasms.
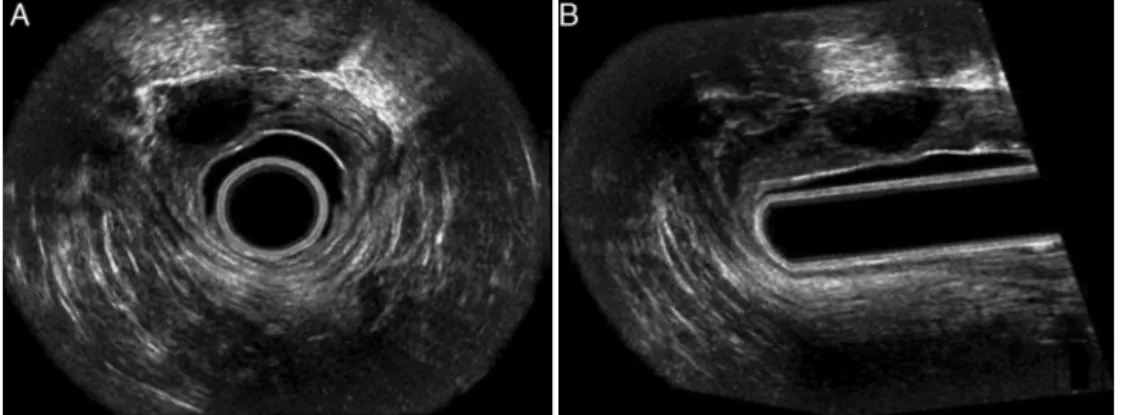
Fig.1–USG-A3Dshowingahypoechoiclesionintheupperregion.(A)Axialcut;(B)diagonalcut.
Case
report
1
Male patient, 57, industrial worker, previously healthy, attendedtheColoproctologyClinicofGastroclínicaCascavel toperformcolonoscopyaspartofamedicalcheck-up. Dur-ingsymptomatologyquestioning,thepatientdidnotreport complaintsorcomorbidities.Thedigitalrectalexamination revealedanelevated,hardened,well-defined,painlesslesion, fixed on the anterior rectal wall, without rectal mucosa changes.The lesionwas locatedabout 5cm from the anal marginandmeasured4cmindiameter.Thepatient under-wentcolonoscopyandUSG-A(Fig.1).Localtransanalexcision wasindicated.Thepatientwashospitalizedontheprocedure day,andarectalcleaningwithfleetenemawascarriedout2h beforetheprocedure.Thesurgicalprocedurewasuneventfully carried out,evolvingonthefirst postoperativedaywithout complaints;thepatientwasdischargedingoodcondition,and hasbeenfollowed-upatourcoloproctologyoutpatientclinic, beingasymptomaticfor3years.
Case
report
2
Fig.2–(A)Viewofaseptalbulging;(B)USG-3D,sagittalcut;(C)USG-3D,crosscut;(D)USG-3Daxialcut.
anorectal junction (rectovaginal septum) measuring about 2.0cm×2.0cm×2.0cm,withoutpenetrationofrectalmuscle
andwithnolymphnodeevidence(Fig.2B–D).Thenodulewas excisedtransvaginally,andthehistopathologyrevealed mes-enchymalneoplasm,withimmunohistochemistrypositivefor CD117(polyclonal)(Fig.3).
Discussion
Histologically,GIST is characterizedby the proliferation of spindle cells, forming small bundles arranged in multiple directions.15 Theimmunohistochemical study is
character-izedbyCD34markerpositivity,rangingfrom46%to100%and withCD117(c-kit)positivityinallcases.16
It is difficult to predict the degree of malignancy for GIST. Hsu et al.3 identified histological features indicating
malignancy,suchastumorsizeandmitoticactivity.Tumors greater than 5.0cm or withmorethan twomitoses byten
high-powerfields(HPF)indicateincreasedriskofmetastasis orrecurrence.17
Theonlyeffectivetreatmentisbysurgicalresectionofthe tumorwithtumor-free margins.Thelaparoscopicapproach isasatisfactoryoptionintheresectionofsmalltumors;in severalseriesofcasesofgastricGISTresection,thisapproach provedtobesafeandwithlowrecurrencerates.18
InpatientswithlargedistalrectalGIST,an abdominoper-inealamputationwillbeneeded.
Neoadjuvantoradjuvantradiotherapyandchemotherapy doesnotprovidegoodresults.19However,imatinibmesylate
(STI571orGleevec),whichactsasatyrosinekinaseinhibitor, hasbeendescribedwithgoodresultsasmonotherapyforthe treatmentofmetastaticGIST.10,17,20Asaneoadjuvantagent,
imatinibcanproducetumordownsizingandallowfor sphinc-terpreservation.
Tothisend,agooddiagnosticevaluationforchoosingthe appropriate surgical treatment should be obtained. USG-A hasbeenwidelyappliedtoclarifythediagnosisofanorectal
parallelimagingsequence(0.25mm),characterizedbythe for-mationofacube.25,26,30,32,52–54
Themobilizationmechanismmaybemanualorautomatic, dependingonthetypeoftransducerused.Theimageformed intoacubecan berecorded and widelydeployed,enabling theoperatortoacquirealltypesofcuts,eveninmultivision, whichconstitutesinsimultaneousviewingfourandsix spe-cializedimages,besidesthepossibilityofsubsequentrevision oftheseimagesasoftenasdesired.Thissignificantlyimproves theaccuracyofthetest,inadditiontoincreasingtheamount ofinformationobtained.52
IncasesofrectalGIST,thescarceliteraturesuggests per-formingnuclearmagneticresonance54sothatonecanattain
accurate assessments. The ultrasound may be an alterna-tive in this area, but the authors used a low-frequency, two-dimensionalendoscopicprobe,55whichresultsina
low-resolutionimagequality.
Inacomparativestudyofresonanceandtwo-dimensional anorectalultrasonographyintheevaluationofpatientswith endometriosis,thesetwotechniqueswereequivalentinterms ofimagequality.Butastudyrelatedtotheevaluationof peri-anorectal layers and tissues with three-dimensional mode versusMRIhasnotyetbeenpublished.56
DespitethegrowingnumberofpublicationsonGIST,there islittleinformationonitsrectalpresentationandonthe eval-uationwithUSG-A.Thistechnologyhastheabilitytoanalyze thesizeofthetumoranditslocation,extentanddepth,aswell asitsrelationshiptoadjacentstructures,besidesanalyzing lymphnodeinvolvement.
Thisstudy aimstotakeinto accountthe importanceof USG-3Dintheevaluationofanorectalregionand perianorec-taltissues,inordertopredictthebesttreatmenttobechosen in the case of suspicion of an anorectal injury, and more specifically,arectalGIST,becausethismethodallowsagood assessmentoftheaffectedrectallayers,besidesdiagnosingif thereisaninvasionofadjacentorgansandblood/lymphatic vessels.
Conclusion
TheuseofanorectalultrasonographyincasesofrectalGIST hasgreatvalueinidentifyingaffectedrectallayers,lesionsize, andinvolvementofadjacentorgansandofblood/lymphatic vessels,helpingintheguidanceforthebesttreatmenttobe proposed.
2006;10:1099–105.
3.HsuK-H,YangT-M,ShanY-S,LinP-W.Tumorsizeisamajor determinantofrecurrenceinpatientswithresectable gastrointestinalstromaltumor.AmJSurg.2007;194:148–52.
4.MiettinenM,LasotaJ.Gastrointestinalstromaltumors: pathologyandprognosisatdifferentsites.SeminDiagn Pathol.2006;23:70–83.
5.TranT,DavilaJA,El-SeragHB.Theepidemiologyofmalignant gastrointestinalstromaltumors:ananalysisof1,458cases from1992to2000.AmJGastroenterol.2005;100:162–8.
6.ShinomuraY,KinoshitaK,TsutsuiS,HirotaS.
Pathophysiology,diagnosis,andtreatmentofgastrointestinal stromaltumors.JGastroenterol.2005;40:775–80.
7.MiettinenM,SobinLH,LasotaJ.Gastrointestinalstromal tumorsofthestomach:aclinicopathologic,
immunohistochemical,andmoleculargeneticstudyof1765 caseswithlong-termfollow-up.AmJSurgPathol.
2005;29:52–68.
8.SanchezVZ.GISTrectal.RevEspEnfermDigMadrid.2008;100.
9.DaniR.Gastroenterologiaessencial.3ed.RiodeJaneiro: GuanabaraKoogan;2006.
10.LiA,NordbergML,HerreraGA.Gastrointestinalstromal tumor:currentconceptsandcontroversies.PatholCaseRev. 2002;7:226–33.
11.HuilgolR,YoungCJ,FracsS.TheGIST:casereportsofa gastrointestinalstromaltumourandaleiomyomaofthe anorectum.ANZJSurg.2003;73:167–9.
12.DragestedJ,GammelgaardJ.Endoluminalultrasonicscanning intheevaluationofrectalcancer:apreliminaryreportof13 cases.GastrointestRadiol.1983;8:367–9.
13.HildrebantU,FiefelG.Preoperativestagingofrectalcancerby intrarectalandmanagementofsquamous-cellcarcinomaof theanalcanal.DisColonRectum.2002;45:16–22.
14.TarantinoD,BernsteinMA.Endoanalultrasoundinthe stagingultrasound.DisColonRectum.1989;28:42–6.
15.LinharesE,ValadãoM.Atualizac¸ãoemGIST.RevColBrasCir RiodeJaneiro.2006;33:51–4.
16.GreensonJK.Gastrointestinalstromaltumourandother mesenchymallesionsofthegut.ModPathol.2003;16:366–75.
17.FranquemontDW.Differentiationandriskassessmentof gastrointestinalstromaltumours.AmJClinPathol. 1995;103:41–7.
18.NishimuraJ,NakajimaK,OmoriT,TakahashiT,NishitaniA, ItoT,etal.Surgicalstrategyforgastricgastrointestinal stromaltumors:laparoscopicvs.openresection.SurgEndosc. 2007;21(6):875–8.
19.HarrisonML,GoldsteinD.Managementofmetastatic gastrointestinalstromaltumourintheGlivecera:apractical case-basedapproach.InternMedJ.2006;36:367–77.
21.BakerH,SchweigerW,CerwenkaH,MischingerHJ.Useof analendosonographyindiagnosisofendometriosisofthe externalanalsphincter.DisColonRectum.1991;42:680–2.
22.BlatchfordGJ.Analultrasonographyintheevaluationoffecal incontinence.SemColonRectalSurg.1995;6:99–104.
23.KleinübingHJr,JanniniJF,MalafaiaO,BrennerS,PinhoTM. Transperinealultrasonography:newmethodtoimagethe anorectalregion.DisColonRectum.2000;43:1572–4.
24.CheongDM,NoguerasJJ,WexnerSD,JagelmanDG.Anal endosonographyforrecurrentanalfistulas:image enhancementwithhydrogenperoxide.DisColonRectum. 1993;36:1158–60.
25.ChristensenAF,NielsenMB,EngelholmSA,RoedH,Svendsen LB,ChristensenH.Three-dimensionalanalendosonography mayimprovestagingofanalcancercomparedwith two-dimensionalendosonography.DisColonRectum. 2004;47:341–5.
26.GoldDM,BartramCI,HalliganS,HumphriesKN,KammMA, KmiotWA.Three-dimensionalendoanalsonographyin assessinganalcanalinjury.BrJSurg.1999;86:365–70.
27.GoldmanS,NormingU,SvenssonC.Transanorectal
ultrasonographyinthestagingofanalepidermoidcarcinoma. IntJColorectalDis.1991;6:152–7.
28.HerzogU,BossM,SpichtinHP.Endoanalultrasonographyin thefollow-upofanalcarcinoma.SurgEndosc.1994;8: 1186–9.
29.HildebrantU,FeifelG.Preoperativestagingofrectalcancerby intrarectalultrasound.DisColonRectum.1985;28:42–6.
30.HunerbeinM,PegiosW,RauB,VoglTJ,FelixR,SchlagPM. Prospectivecomparisonofendorectalultrasound,
three-dimensionalendorectalultrasoundandendorectalMRI inthepreoperativeevaluationofrectaltumors.Preliminary results.SurgEndosc.2000;14:1005–8.
31.KatsuraY,YamadaK,IshizawaT,YoshinakaH,ShimazuH. Endorectalultrasonographyfortheassessmentofwall invasionandlymphnodemetastasisinrectalcancer.Dis ColonRectum.1992;35:362–8.
32.KimJC,ChoYK,KimSY,ParkSK,LeeMG.Comparativestudy ofthree-dimensionalandconventionalendorectal
ultrasonographyusedinrectalcancerstaging.SurgEndosc. 2002;16:1280–5.
33.RegadasSMM,RegadasFSP,RodriguesLV,NogueiraMAA, RegadasRP.Ultrasomanorretal.Indicac¸õeseresultados preliminares.RevBrasColoproctol.1999;19:5–10.
34.SentovichSM,BlatchfordGJ,FalkPM,ThorsonAG,
ChristensenMA.Transrectalultrasoundofrectaltumors.Am JSurg.1993;166:638–42.
35.SchröderJ,LöhnertM,DoniecJM,DohrmannP.Endoluminal ultrasounddiagnosisandoperativemanagementofrectal endometriosis.DisColonRectum.1997;40:614–7.
36.TarantinoD,BernsteinMA.Endoanalultrasoundinthe stagingandmanagementofsquamosous-cellcarcinomaof theanalcanal:potentialimplicationsofanewultrasound stagingsystem.DisColonRectum.2002;45:16–22.
37.WilliamsJG.Analultrasonographyinthediagnosisand managementofabscessandfistuladiseaseoftheanorectum. SemColonRectalSurg.1995;6:105–13.
38.YangYK,WexnerSD,NoguerasJ,JagelmanDG.Theroleof analultrasoundintheassessmentofbenignanorectal disease.Coloproctology.1993;5:260–4.
39.RoschT,LorenzR,ClassenM.Ultrasonographyinthe evaluationofcolonandrectaldisease.GastrointestEndosc. 1990;36:S33–9.
40.TioTL,WeijersO,HulsmanF,JonkersL,CollinsE,SieLH,etal. Endosonographyofcolorectaldiseases.Endoscopy.1992;24 Suppl.1:309–14.
41.SchroderJ,LohnertM,DoniecJM,DohrmannP.Endoluminal ultrasounddiagnosisandoperativemanagementofrectal endometriosis.DisColonRectum.1997;40:614–7.
42.TjandraJJ,MilsonJW,StolfiVW,LaveryI,OakleyJ,ChurchJ, etal.Endoluminalultrasounddefinesanatomyoftheanal canalandpelvicfloor.DisColonRectum.1992;35:465–70.
43.BahrA,ParadesV,GadonneixP,EtienneyI,Salet-LizeED, VilletR,etal.Endorectalultrasonographyinpredictingrectal wallinfiltrationinpatientswithdeeppelvicendometriosis:a moderntoolforanancientdisease.DisColonRectum. 2006;49:869–75.
44.KleinubingHJr,JanniniJF,MalafaiaO,BrennerS,PinhoM. Transperinealultrasonography:newmethodtoimagethe anorectalregion.DisColonRectum.2000;43:1572–4.
45.PiloniV.Dynamicimagingofpelvicfloorwithtransperineal sonography.TechColoproctol.2001;5:103–5.
46.Beer-GabelM,TeshlerM,BarzilaiN,LurieY,MalnickS,BassD, etal.Dynamictransperinealultrasoundindiagnosisofpelvic floordisorders–apilotstudy.DisColonRectum.
2002;45:239–48.
47.Beer-GabelM,TeshlerM,SchechtmanE,ZbarAP.Dynamic transperinealultrasoundvs.defecographyinpatientswith evacuatorydifficulty:apilotstudy.IntJColorectalDis. 2004;19:60–7.
48.AdamsDR,BlatchfordGJ,LinKM,TernentCA,ThorsonAG, ChristensenMA.Useofpreoperativeultrasoundstagingfor treatmentofrectalcancer.DisColonRectum.1999;42:159–66.
49.KarausM,NeuhausP,WiedenmannB.Diagnosisof
enterocelesbydynamicanorectalendosonography.DisColon Rectum.2000;43:1683–8.
50.GavioliM,BagniA,PiccagliI,FundaroS,NataliniG.Usefulof endorectalultrasoundafterpreoperativeradiotherapyin rectalcancer.DisColonRectum.2000;43:1075–83.
51.BuchananGN,BartramCI,WilliamsAB,HalliganS,Cohen CRG.Valueofhydrogenperoxideenhancementof
three-dimensionalendoanalultrasoundinfistula-in-ano.Dis ColonRectum.2005;48:141–7.
52.RegadasSMM,RegadasFSP,RodriguesLV,SilvaFR,LimaDMR, Regadas-FilhoFSP.ImportânciadoUltra-somTridimensional naAvaliac¸ãoAnorretal.ArqGastroenterol.2005;42:226–32.
53.DamC,LindebjergJ,RafaelsenSR.MRIofrectalstromal tumour.UgeskrLaeger.2012;174:1826–7.
54.Murad-RegadasSM,RegadasFSP,RodriguesLV,EscalanteRD, SilvaFRS,LimaDMR,etal.EcodefecografiaTridimensional Dinâmica.NovaTécnicaparaAvaliac¸ãodaSíndromeda Defecac¸ãoObstruída(SDO).RevbrasColoproct. 2006;26:168–77.
55.HussainT,SalamatA,FarooqMA,HassanF,HafeezM. Indicationsforendoscopicultrasoundanddiagnosison fine-needleaspirationandcytology.CollPhysiciansSurgPak. 2009;19:223–7.