w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Oncology
ostomized
patients’
perception
regarding
sexual
relationship
as
an
important
dimension
in
quality
of
life
Cristilene
Akiko
Kimura
a,b,∗,
Dirce
Bellezi
Guilhem
c,
Ivone
Kamada
d,
Breno
Silva
de
Abreu
a,b,d,
Renata
Costa
Fortes
b,daUniversidadedeBrasília(UnB),Brasília,DF,Brazil
bFaculdadedeCiênciaseEducac¸ãoSenaAires(Facesa),ValparaísodeGoiás,GO,Brazil cUniversidadedeBrasília(UnB),FaculdadedeCiênciasdaSaúde,Brasília,DF,Brazil dUniversidadePaulista,Brasília,DF,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received27April2016
Accepted27March2017
Availableonline18May2017
Keywords:
Qualityoflife
Ostomy Sexuality
Colorectalneoplasms
a
b
s
t
r
a
c
t
Introduction:Forostomizedoncologicalpatients,thephysicalbodyalterationsaffectsthe
qualityoflife,asthechangesintheself-conceptarefactorsthatdirectlyaffectthesexual
life.
Objective:Toanalyzetheperceptionsofostomizedmenduetointestinalcancerregarding
sexualrelationsasanimportantdimensionofqualityoflife,treatedattheAmbulatoryCare
ProgramforOstomizedPatientsoftheHealthSecretariatoftheFederalDistrict,Brazil.
Methods:Epidemiological-basedstudy,oftheanalyticaltype,withacross-sectional
descrip-tivedesign,withquantitativeandqualitativeapproachconsideringthecontentanalysis.
The convenience sample included56 participants. Sociodemographic,clinical,and the
WHOQOL-BREFquestionnaireswereused,aswellasanindividualinterview.Datawere
analyzedbyMicrosoftOfficeExcel2010andSPSS20.0software.Statisticalsignificancewas
setat5%.
Results:ThePhysical,SocialRelationsandEnvironmentDomainsarecorrelatedwiththe
mean score,statisticalsignificance(p<0.0001),andthecontentanalysisresultedinfive
categories:Ostomy,Self-Care,Acceptance,Self-concept,andCompanionship.
Conclusion: Sexualityshouldbeconsideredasaprocessofdailylivingofostomized
individ-ualsduetointestinalcancer.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This
isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](C.A.Kimura).
http://dx.doi.org/10.1016/j.jcol.2017.03.009
2237-9363/©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC
Um
olhar
dos
homens
estomizados
intestinais
oncológicos
sobre
a
relac¸ão
sexual
como
dimensão
importante
na
qualidade
de
vida
Palavras-chave:
Qualidadedevida
Ostomia Sexualidade
Neoplasiascolorretais
r
e
s
u
m
o
Introduc¸ão: Paraapessoaestomizadaintestinaloncológicaosignificadodaalterac¸ãono
corpofísicoafetaaqualidadedevida,poisencontra-secomasalterac¸õesnoautoconceito
sãofatoresquedificultamdiretamenteorelacionamentosexual.
Objetivo: Analisaraspercepc¸õesdoshomensestomizadosintestinaisoncológicosquanto
aorelacionamentosexualcomodimensãoimportantenaqualidadedevida,atendidospelo
ProgramadeAssistênciaAmbulatorialaoEstomizadodaSecretariadeSaúdedoDistrito
Federal,Brasil.
Métodos: Estudodebaseepidemiológica,decaráteranalítico,comdelineamento
transver-saledescritivo,comabordagemquantitativaequalitativaàluzdaanálisedeconteúdo.A
amostrafoiconstituídaporconveniência,incluídos56participantes.Utilizou-seos
ques-tionáriossóciodemográfico,clínico,eoWHOQOL-brefeumaentrevistaindividual.Osdados
foramanalisadospelosprogramasMicrosoft® OfficeExcel2010eSPSS20.0.Asignificância
estatísticaaceitafoide5%.
Resultados: OsDomíniosFísico,Relac¸õesSociaiseMeioAmbienteestãocorrelacionadas
comoescoremédio,significânciaestatística(p<0,0001),aanálisedeconteúdoresultouem
cincocategorias:Estomia,Autocuidado,Aceitac¸ão,AutoconceitoeCompanheirismo.
Conclusão: A sexualidade deve ser considerada como processo do viver cotidianodo
estomizadointestinaloncológico.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este
´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
Introduction
TheWorldHealthOrganizationdefinesqualityoflifeas“the
individualsperceptionoftheirpositioninlifeinthecontext
ofthecultureandvaluesysteminwhichtheyliveandin
rela-tiontotheirgoals,expectations,standards andconcerns”.1
Basedonthisaspect,qualityoflifeisabroadand
compre-hensiveconcept,affectedinacomplexwaybythehealthof
thephysicalperson,thatis,itismultidimensional,dynamic,
subjective,individual,complexandseekstointerconnectthe
physical,social,spiritualandenvironmentalaspects.2,3
Fur-thermore,from asubjectiveperspective, theassessmentof
qualityoflifedependsdirectlyontheevaluationofthe
indi-viduals.Inthemultidimensionaldomain,itisimportantto
evaluatetheirphysicalwell-being,theirfunctionalcapacity,
theirpsychologicalandsocialhealth.2,3Therefore,and
consid-eringthequalityoflifeasoneofthedimensionsofhumanlife,
itsevaluationbecomesveryimportant,particularlyregarding
thesexualityoftheoncologicalostomizedmalepatients.
However,sexualitycanbeunderstoodasafundamental
aspectoflifeandispresentsinceuntildeath,havingspecific
characteristics ineach periodofthelifecycle. Sexualityis,
therefore,thesetofemotions,feelings,fantasies,desires,and
interpretationsthatthehumanbeingexperiencesthroughout
life.4
Simultaneously,sexuality constitutes anintegralpart of
thehumanpersonality, associatingpersonaland emotional
experiences,socioculturalknowledge,beliefs,andvaluesbuilt
throughout history and, thus, the sexual life cannot be
separatedfromthesocial,historical,anthropologicaland
psy-chologicalthemes.4
Inthissense,fortheoncologicalostomizedindividual,the
meaningofthealterationsinthephysicalbodyandthe
suf-feringcausedbythenewlifestyleaffectsthequalityoflife,
duetothechangesinbodyimage,thelowself-esteem,with
feelingsofrejectionandchangesindailyactivities,whichare
factorsthatdirectlyaffectthesexuallife.3,5
Basedonthisconception,theobjectiveofthisstudywasto
analyzetheperceptionsofoncologicalostomizedmale
indi-vidualsregardingsexualrelationsasanimportantdimension
ofqualityoflife,treatedattheAmbulatoryCareProgramfor
Ostomized PatientsoftheHealth SecretariatoftheFederal
District,Brazil.
Material
and
methods
Studymethodology
This isepidemiological-based study,ofthe analytical type,
with across-sectionaldescriptive design,withquantitative
and qualitative approachconsidering the content analysis.
Participants included in the study belonged to a group of
ostomized individuals dueto colorectal cancer.The
obser-vation and measurement of the variables ofinterest were
performedsimultaneously,constitutingastatisticalimageof
whatoccursatagivenmoment.
Thedatacollectionoftheinterviewwasanalyzed
consider-ingtheBardinContentAnalysis,whichisbasedonthephase
ofdescriptionormaterialpreparation,inferenceordeduction
andinterpretation.6
ThestudyprotocolwasapprovedbytheResearchEthics
SaúdeoftheStateHealthSecretariatoftheFederalDistrict,
Brazil,underprotocolnumber418/200.Theindividualswho
agreedtoparticipateinthestudysignedtheFreeandInformed
Consentform,afterreceiving detailedexplanationson
pro-posed goals and procedures. The confidentiality about the
originofdataandthevolunteers’anonymitywasguaranteed,
asstatedintheBrazilianregulationsforresearchinvolving
humanbeings.7Inthissense,torespecttheanonymityofthe
volunteerseach interview wasidentifiedwiththe letter “I”
(individual)andanumberindicatingtheorderofits
perfor-mance.
Sample
Thepresentwasaconveniencesample,consideringthe
spon-taneousdemandforthestudyparticipation.Weincluded56
ostomizedindividualsduetocolorectalcancerandenrolled
intheAmbulatoryCareProgramforOstomizedPatientsofthe
HealthSecretariatoftheFederalDistrict,Brasília,Brazil.
Theinclusioncriteriacomprisedmalepatientswitha
diag-nosisofcolorectalcancer,submittedtoasurgicalintervention
forthepreparationofanintestinalstoma,andstable
mar-ital statusof twenty years or more. Children, adolescents,
pregnantandnursingwomen,bedriddenindividuals,female
gender,individualswithotherphysicaldisabilities,and
indi-vidualswho refusedtoparticipatewere excludedfrom the
study.
Datacollection
DatawerecollectedfromMarch2010toAugust2012.Twotools
wereused:asociodemographicandclinicalquestionnaireand
thevalidatedversionoftheWHOQOL-brefquestionnairefor
thePortugueselanguage.Itcomprised26items:twogeneral
questions,relatedtotheperceptionaboutqualityoflifeand
satisfactionwithhealth.Thefourdomains(Physical,
Psycho-logical,SocialRelationsandEnvironment)wereobserved.8
Datacollectionfromtheinterviewwasanalyzedbasedon
Bardin’sContentAnalysis,6startingwiththestudy’sguiding
question:“Tellmeaboutyoursexualrelationships”.The
inter-views were transcribedinfull, right aftereach report. The
speecheswerereadintheirtotality,severaltimes,andat
dif-ferentmoments,so thatit was possibletounderstandthe
discourses,identifythecentralideasandkeywords,observing
therepetitionsandsimilaritiesbetweentheinterviews.The
nextstepwastocondensetheinterviews,tobeginthe
catego-rization.Aflowchartwascreatedtoanalyzethecategorization
data(Fig.1).
Statisticalanalysis
Thedescriptivestatisticalanalysisofthesociodemographic
andclinical questionnairedatawas performed,inaddition
totheinterview.DatafromtheWHOQOL-brefquestionnaire
wereanalyzedthroughmeans,standarddeviationand
pro-portionsandinferentialanalysisusingthefollowingstatistical
procedures:95%confidenceinterval,Student’sttest,and
Pear-son’slinearcorrelationcoefficient.
ThestatisticalanalysiswasperformedusingtheSPSS
soft-ware (Statistical Packageof the Social Sciences, SPSS Inc.,
Chicago, USA) for Windows version 20.0, according to the
WorldHealthOrganizationguidelines.Theacceptedstatistical
significancewassetat5%
Results
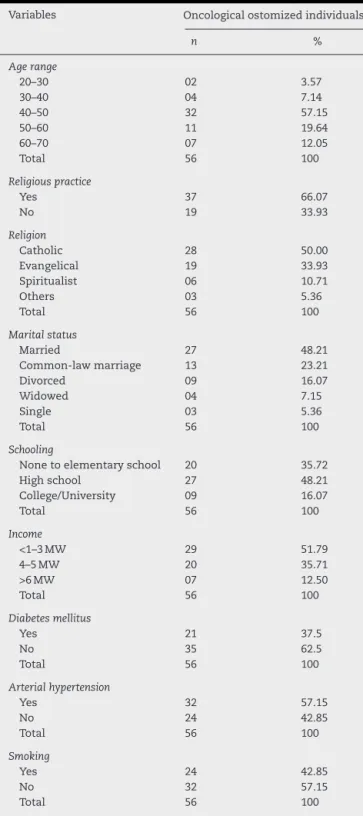
Table1showsthesociodemographicand clinical
character-ization ofthe study participants. The mean age ofthe 56
Table1–Sampleofoncologicalostomizedindividuals accordingtosociodemographicandclinical
characteristics.Brasília,FederalDistrict,Brazil,2016.
Variables Oncologicalostomizedindividuals
n %
Agerange
20–30 02 3.57
30–40 04 7.14
40–50 32 57.15
50–60 11 19.64
60–70 07 12.05
Total 56 100
Religiouspractice
Yes 37 66.07
No 19 33.93
Religion
Catholic 28 50.00
Evangelical 19 33.93
Spiritualist 06 10.71
Others 03 5.36
Total 56 100
Maritalstatus
Married 27 48.21
Common-lawmarriage 13 23.21
Divorced 09 16.07
Widowed 04 7.15
Single 03 5.36
Total 56 100
Schooling
Nonetoelementaryschool 20 35.72
Highschool 27 48.21
College/University 09 16.07
Total 56 100
Income
<1–3MW 29 51.79
4–5MW 20 35.71
>6MW 07 12.50
Total 56 100
Diabetesmellitus
Yes 21 37.5
No 35 62.5
Total 56 100
Arterialhypertension
Yes 32 57.15
No 24 42.85
Total 56 100
Smoking
Yes 24 42.85
No 32 57.15
Sexuality and sexual relations of the oncological ostomized individual
Stoma Self-care Acceptance Self-concept Companionship
Fig.1–Organogramofcontentanalysisofoncologicalostomizedindividuals.Brasília,FederalDistrict,Brazil,2016.
oncologicalostomizedindividualswas56.42±12.16years,and
mostof them,57.15%, was aged between 50 and 59 years
(n=32).
Consideringtheothersociodemographicvariables,a
pre-dominanceoftheCatholicreligionwasfoundin50%(n=28)
and66.07%(n=37)performedreligious practices.Regarding
formal education, 48.21% (n=27) had finished high school.
Regarding the monthly income, the most common range
reportedbythe participants,51.79%(n=29), wasbetween1
and3minimumwages.
Abouttheclinicalaspectrelatedtocomorbidities,57.15%
(n=32)hadarterialhypertensionand37.5%(n=21)Diabetes
Mellitus.Additionally,57.14%(n=32)oftheparticipantswere
smokers.
RegardingtheresultsofTable2,theyshowedstatistically
significant differencesinthe mean scoresforthe physical,
psychological,socialrelations,and environmentaldomains,
aswellasoverallqualityoflife,leadingtostatistical
signifi-cance(p<0.0001).
Table3describesthecategorizationofinterviews,resulting
infivecategories,namely:Ostomy,Self-Care,Acceptance,
Self-conceptandCompanionship.
Discussion
Theanalysisofsociodemographicandclinicaldatarevealed
thatthemeanagewas56.42±12.16years.Studiesindicatea
prevalenceofcolorectalcancerintheagegroupolderthan50
years,anditisverifiedthatmorethan90%ofthesecancers
occurinindividualsolderthan50years.2,3,9,10
Colorectalcancerisamongthemaincausesforthestoma
creation.Amongtheriskfactorsforthistypeofcancer,there
isadirect associationwiththe food pattern,characterized
byaddictions andinadequate eatinghabits favoring
bacte-rialproliferationandtheconsequentdegradationofbileacids
producingcarcinogenicagents.2,3,9,11
It was observed that the predominant religions were
Catholic50%(n=28),followedbyEvangelicalreligions,33.93%
(n=19),and66.07%(n=37)ofparticipantsperformedreligious
Table3–Categorizationoftheinterviewsofthe oncologicalostomizedindividuals.Brasília,Federal District,Brazil,2016.
Ostomy “Itisverysadtolivewiththisstoma.[...].”(I1).
“Thisstomamakesmefeeldepressed,howcanIthinkabout havingintercoursewithmywife[...].”(I2).
“Thispouchimpairsmylife,Idonotfeellikeleavinghome.”(I3). “Iammuchquieterduringsex.Thispouchreallyinterferes[...].” (I4).“
Igetveryworriedaboutthepouchandthus,Icannotdoit[...].” (I5).
Self-Care
“Ialwaysdependonmywifetochangemypouch.Ifeelsafer”(I6). “MyGod,itissodifficulttochangethispouch[...]”(I7). “Mywifeandevenmydaughterhelpmesometimestochange thepouch[...]”(I8).
“Ididnothavemuchdifficulty.Myfamilyhelpedme.[...]”(I9).
Acceptance
“Ithoughttomyself,thereisnootherway.So,Ineedtoadaptto thispouch.”(I10).
“Whatmademeacceptandlivewiththispouchwasthe supportofmyfamily”.(I11).
“Atfirstitwasverydifficulttoacceptthispouch[...]”(I12). “Myfamilygavemethecouragetolivewiththispouch.”(I13).
Self-concept
“Forme,itisnotnormaltohaveaholeinmybelly,themost depressingthingistoevacuateinapouch.Ihavenostimulus foranything.”(I14).
“Itisverydifficulttoseemyselfinthemirrorwiththisbody. [...]”.(I15).
“IfeellikeI’mcarryingacrossonmywaist”(I16).
“Today,whenIlookatmyself,Ifeelmutilated...Ialwaystook careofmybody”.(I17).
“Afterthesurgery,Ineverletmywifeseemenakedagain.Ifeel Iamnogoodasamananymore[...]”.(I18).
Companionship
“Withoutmywife,Icouldneverlivewiththispouch[...]”.(I19). “MywifefromthebeginningalwaysdideverythingsothatI wouldnotfeelbadaboutthepouch.”(I20).
“Ihaveablessedwife,whoismycompanion.[...].”(I21). “Mywifemademefeellikeabetterman.[...].”(I22).
Table2–MeanscoresofthedomainsandqualityoflifeoftheWHOQOL-brefquestionnaireinoncologicalostomized individuals.Brasília,FederalDistrict,Brazil,2016.
Groupofoncologicalostomizedindividuals
Domains n Mean SD 95%CI p
Physical 56 12.02 2.38 11.41–12.31 <0.0001
Psychological 56 12.20 2.74 11.47–12.53 <0.0001
Socialrelations 56 12.44 2.87 12.05–13.02 <0.0001
Environment 56 12.02 2.23 11.58–12.32 <0.0001
practices.Studieshaveshownthatreligiouspracticesinthe
presenceofthe disease can leadtospiritual development,
sinceitremindstheindividualofhisfragilityandcloseness
withhumanfinitude.2,3,5,9,12
Regardingthefamilyincomeand educationallevel, both
were relatively low,with anaverage family incomeof2.68
minimumwages.Thesedataemphasizetherelevanceof
gov-ernmentassistancetotheseindividuals.Lowschoolingmay
beafactorforthenon-preventionofcolorectalcancer,dueto
theprecariousexplanationaboutthefactorsthatcausethis
neoplasm,includingdietaryones.5,12
Regarding comorbidities, most participants had arterial
hypertension(57.15%)(n=32),andasignificantnumberhad
type2diabetes(35.50%)(n=21).Thecombinationofthesetwo
conditionscontributestothehighriskofdeveloping
colorec-talcancer.2,3,10Additionally,57.14%(n=32)oftheparticipants
weresmokers.Althoughthecolonisnotdirectlyaffectedby
thetobaccocomposition,thecarcinogenicsubstancescarried
bytheblood stream haveanegativeimpacton the riskof
developingcolorectalcancer.2,3,13
Themeanscoresforthedomainsandqualityoflifeofthe
WHOQOL–brefquestionnaire,inTable3,showstatistically
significantdifferences inthe mean scoresforthephysical,
psychological,social,andenvironmentaldomains,andinthe
meanscoreofthequalityoflife.Studiesonthequalityoflife
ofoncologicalostomizedpatientsindicatethatthecreationof
theintestinalstomainvolvesnotonlytheuseofthecollection
equipment,butalsoanewbodyimagethatneedstobe
recon-structed.Thisisaprocessthatisatthesametimesubjective,
collective,andsocial,anddeeplyreflectiveaboutthe
coexis-tencewithanintestinalstoma,whichcanaffectthephysical
andpsychologicaldomains,aswellassocialrelationsandthe
environment,impairingtheirqualityoflife.2,3Inthe“stoma”
category,theparticipants’statementsaboutthe creationof
theintestinalstomadiscloseseveraldisordersforthe
individ-uals,andamongthemaresexualfunction,maritaladjustment
andchangeinbehaviorrelatedtothesexuality.Itisbelieved
thatthesechangesmaybecloselyrelatedtochangesinbody
imageandconsequentdecreaseinself-esteem.5,12,14
In addition to the emotional difficulties, the intestinal
stomageneratesaseriesofphysicalalterationsthatimpairs
sociallife.Asaconsequence,thepersonfeelsdifferentfrom
others and even excluded. Thisoccurs because all human
beingsbuild,throughouttheir lives,animageoftheirown
body,whichadaptstotheircustoms,theenvironmentwhere
theylive,etc.,whichmeettheirneedstofeelsituatedintheir
ownworld.4,15,16
Inthe“Self-care”category,itcanbeobservedthatinthe
reportsoftheostomizedpatients, thecollectingequipment
startstorepresentthelostbodypart,establishingnewhabits
throughlearning,mainlyregardingself-care. Theintestinal
stomaalterstheroleoftheostomizedindividualinthefamily
andinsociety.Afterthesurgery,manyostomizedindividuals
starttodependonfamilycare,eventemporarily,inaddition
toexperiencingthesociallyimposeddisabilitiesandleaving
behindtheattributesofindependence,efficiency,and
produc-tivity,whichinterferewithsexualrelations.5,16–18
Regarding the “Acceptance” category, the reports show
thattheostomizedindividualundergoesaprocessstructured
into fourphases, withthe final onebeing theevolution of
acceptance,aprocessthatmustbeaconstructiveone;
accord-ingtotheirperceptionofthepresenceoftheintestinalstoma,
so theiracceptanceis reflected,which ends up
contradict-ing theobtainedresults.Inthis sense,this realitydepends
onthesupportandencouragementthatthepatientsreceive
fromthosearoundthem,includingthehealthprofessionals
whoarepartofthesupportsystempresentedtothem.The
oncologicalostomizedindividualrequirescarethatmustbe
maintained, promotingtheir independence,theirqualityof
lifeforthemselves,theirfamilies,andtheircaregivers.4,17
In the“Self-concept”category, participants,when asked
about theinterferenceoftheintestinalstomaintheir
inti-macy,reportedthatsexualactivityisaffected.Thus,thesexual
relationsarecloselyrelatedtotheideaofself-conceptandthe
consequentalterationinthebodyimageanddecreaseinthe
self-esteemandtheperceptionofsexualattraction,especially
regardingthelossofcontrolintheeliminationofstooland
gasesasaconditionpredisposingtopsychologicalandsocial
isolation,basedonnegativefeelingsthatpermeate
interper-sonalrelations.5,18–21Theuseofthecollectionpouchmakes
socialinteractiondifficultastheyraiseseveralconcernsinthe
patient, inducingtheostomizedindividual toasituationof
detachmentandsocialisolation,impairingtheself-concept.2,3
Regarding the “Companionship” category, the reportsof
theparticipantsaboutcompanionshiprelatedtosexual
activ-ity was considered essential for the sexual relations and,
therefore,sexualityisabroadfunctionthatcoversbiological,
psychological,andsocialaspects.5 Respect,companionship,
admiration, and reciprocallove are necessary between the
individuals. Therefore, the modifications that occur in the
sexuality of ostomized individuals are so profound and
mutilating that the sexual act becomes secondary and is
usuallyreplaced byfeelingsof love,affection, respect, and
companionship.4,22,23
Ontheotherhand,thesexualityofthehumanbeingisnot
restrictedtothepurelyprocreativeapproach.Asexualrelation
betweentwoindividualsinvolvesnotonlybiologicalduties,
but,ontheotherhand,allcorporeality,anemotionalbond,an
infinityoffeelings,aswellassocialandculturalvaluesofthe
couple.4,17
In viewofthe above, thesexual relationissignificantly
impaired,astheostomizedindividualhasnegativefeelingsfor
havinganexternalizedpartandforexperiencingthestigma
ofbeinganostomizedindividual,especiallyinthemale
gen-der, as they suffer greater pressure regarding their sexual
performance.4,5
However,sometimessuchchangesmayberelatedtothe
complications resulting from the surgical procedure,
espe-ciallynervedamage.Mostpatientswithintestinalstomasdo
notreturntotheirsexualactivityordosoonlypartially,due
tophysicalproblems,problemswiththecollectionpouch,a
decreasedsenseofhygieneduringsexualactivity,i.e.,a
feel-ingofbeingdirtyandshameorfearofnon-acceptancebythe
partner.5,15
Inseveralstudies,theliteratureindicatesthat the
sexu-alitydomainislittleconsideredamonghealthprofessionals,
regardingthepatientwithintestinalstoma.Itcanbeobserved
thathealthprofessionalsneedmoretraining toanswer the
doubtsofostomizedindividuals,alsohighlightingissues
imageandstrategiestodealwiththeseissueswithpatients
inasensitivemannerthatfullymeetstheirneeds.5,23
Conclusions
Thus,oncologicalostomizedindividualsreportedchangesin
bodyimage,lowself-esteem,andchangesindailyactivities,
whicharefactorsthatimpairtheprocessofadaptationinthe
sexualrelationswithinarealitythatwas,todate,unknown.In
thissense,sexualityshouldbeconsideredasaprocessofdaily
livingforthepatient,stressingtheimportanceoftheir
corre-lationwithprofessionalpracticeso theseprofessionalscan
assistthepatientsandtheirpartnersintheprocessof
adap-tationtothenewconditionsandinthesearchfornewcoping
strategiesforanactiveandpleasurablesexuallife,resulting
inimprovedqualityoflife.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. WorldHealthOrganization.TheWHOQOLGroup.Qualityof
lifeassessment(WHOQOL):positionpaperfromtheWorld
HealthOrganization.SocSciMed.1995;41:1403–9.
2. KimuraCA,KamadaI,GuilhemD.Qualityoflifeofindividual ostomydueoncologicalreasons:naapproachofintegrality fromBrazilianUnifiedHealthSystem.JColoproctol. 2016;36:34–9.
3. KimuraCA,KamadaI,JesusCAC,GuilhemDB.Qualityoflife ofcolorectalcancerpatientswithintestinalstomas.J CarcinogenMutagen.2014;5:1–7.
4. KimuraCA.Qualidadedevidadepacientesoncológicos
estomizados.149f.Dissertac¸ão(MestradoemEnfermagem)–
UniversidadedeBrasilia.2013.
5. KimuraCA,KamadaI,GuilhemD,FortesRC.Perceptionof sexualactivitiesandthecareprocessinostomizedwomen.J Coloproctol.2013;33:145–50.
6. BardinL.Análisedeconteúdo.Lisboa:Edic¸ões70;2008.
7. Brazil.MinistryofHealth.NationalHealthCouncil.Resolution
N.466/2012.Guidelinesandregulatingnormsforresearch
involvinghumansubjects.Brasilia:CNS;2012.Availableat:
http://conselho.saude.gov.br/resolucoes/1996/Res196en.pdf. 8. FleckMPA,LouzadaS,XavierM,ChachamovichE,VieiraG,
SantosL,etal.Aplicac¸ãodaversãoemportuguêsdo
instrumentoabreviadodeavaliac¸ãodaqualidadedevida WHOQOL-bref.RevSaúdePúbl.2000;34:178–83.
9.KimuraCA,KamadaI,GuilhemD,MonteiroPS.Qualityoflife analysisinostomizedcolorectalcancerpatients.J
Coloproctol.2013;33:216–21.
10.MinistériodaSaúde(BR).SecretariadeAtenc¸ãoàSaúde.
InstitutoNacionaldeCâncer.Estimativas2015:incidênciade
câncernoBrasil.RiodeJaneiro:INCA;2015.
11.SchneiderEC,MalinJL,KahnKL,KoCY,AdamsJ,EpsteinAM. Survivingcolorectalcancer:patient-reportedsymptom4 yearsafterdiagnosis.Cancer.2007;11:2075–82.
12.HawkinsD,BoothA.Unhappilyeverafter:affectsof
long-term,lowqualitymarriagesonwell-being.SocialForces. 2005;84:451–75.
13.StürmerT,GlynnRJ,LeeIM,ChristenWC,HennekensCH. ‘Lifetimecigarettesmokingandcolorectalcancerincidence inthePhysicians’HealthStudyI’.JNatlCancerInst. 2000;92:1178–81.
14.FortesRC,MonteiroTMTC,KimuraCA.Qualityoflifefrom oncologicalpatientswithdefinitiveandtemporary colostomy.JColoproctol.2012;32:253–9.
15.MahjoubiB,MirzaeiR,AziziR,JafariniaM,ShoolamiLZ.A cross-sectionalsurveyofqualityoflifeincolostomates:a reportfromIran.HealthQualLifeOutcomes.2012;10:1–6.
16.NascimentoCMS,GraciaraLBT,MariaHBAL,RobertaFS. Vivênciadopacienteestomizado:umacontribuic¸ãopara assistênciadeenfermagem.TextoContextodeEnfermagem. 2011;20:357–64.
17.LobãoC,ManoelG,AntónioM,PedroS.Aceitandoa Contra-Natura?Oprocessodeaceitac¸ãodoestadodesaúde dapessoacomostomia,RevistaReferencia.RevCientUnid InvestCiêncSaúde.2009;11:23–37.
18.RamirezM,McMullenC,GrantM,AltschulerA,Hornbrook MC,KrouseRS.Figuringoutsexinareconfiguredbody: experiencesoffemalecolorectalcancersurvivorswith ostomies.WomenHealth.2009;49:608–24.
19.DabirianA,YaghmaeiF,RassouliM,TafreshiMZ.Qualityof lifeinostomypatients:aqualitativestudy.PatientPrefer Adherence.2011;5:1–5.
20.FavaratoMECS,AldrighiJM,FráguasJR,PiresALR,LimaSMR. Sexualidadeeclimatério:influenciadefatoresbiológicos, psicológicosesócio-culturais.ReprodClim.2000;15:199–202.
21.BurchJ.Providinginformationandadviceondiettostoma patients.BrJCommunityNurs.2012;16:479–84.
22.BaldwinCM,GrantMRN,WendelC,HornbrookMC,Herrinton LJ,McMullenC,etal.Genderdifferencesinsleepdisruption andfatigueonqualityoflifeamongpersonswithostomies.J ClinSleepMed.2009;5:335–43.