www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Reproducibility
(test---retest)
of
vestibular
evoked
myogenic
potential
夽
,
夽夽
Aline
Cabral
de
Oliveira
a,b,c,∗,
Pedro
de
Lemos
Menezes
a,d,
Liliane
Desgualdo
Pereira
a,eaUniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil bUniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
cUniversidadeFederaldeSergipe(UFS),Aracaju,SE,Brazil
dUniversidadeEstadualdeCiênciasdaSaúdedeAlagoas(UNCISAL),Maceió,AL,Brazil
eDepartmentofPhonoaudiology,UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
Received3December2013;accepted6April2014 Availableonline28August2014
KEYWORDS
Evokedpotentials;
Vestibulelabyrinth;
Vestibularnerve;
Electromyography
Abstract
Introduction:Thereisstillnoconsensusintheliteratureastothebestacousticstimulusfor capturingvestibularevokedmyogenicpotential(VEMP).Low-frequencytoneburstsare gener-allymoreeffectivethanhigh-frequency,butrecentstudiesstilluseclicks.Reproducibilityisan importantanalyticalparametertoobservethereliabilityofresponses.
Objective:Todeterminethereproducibilityofp13andn23latencyandamplitudeoftheVEMP forstimuliwithdifferenttone-burstfrequencies,andtodefinethebesttestfrequency. Methods:Cross-sectionalcohortstudy.VEMPwascapturedin156ears,onthe sternocleidomas-toidmuscle,using100tone-burststimuliatfrequenciesof250,500,1000,and2000Hz,and soundintensityof95dBnHL.Responseswerereplicated,thatis,recordedthreetimesoneach side.
Results:Nosignificantdifferencewas observedforp13 andn23 latenciesoftheVEMP, cap-turedatthreemomentswithtone-burststimuliat250,500,and1000Hz.Onlythefrequency of2000Hzshowed adifferencebetweencaptures ofthispotential(p<0.001).p13 andn23 amplitudeanalysiswasalsosimilarinthetest---retestforallfrequenciesanalyzed.
Conclusion:p13andn23latenciesandamplitudesofVEMPfortone-burststimuliatfrequencies of250,500,and1000Hzarereproducible.
© 2014Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:deOliveiraAC,MenezesPL,PereiraLD.Reproducibility(test---retest)ofvestibularevokedmyogenicpotential. BrazJOtorhinolaryngol.2015;81:264---9.
夽夽
Institution:UniversidadeFederaldeSergipe,Aracaju,Sergipe,SE,Brazil/UniversidadeFederaldeSãoPaulo,SãoPaulo,SP,Brazil. ∗Correspondingauthor.
E-mail:[email protected](A.C.deOliveira). http://dx.doi.org/10.1016/j.bjorl.2014.04.001
PALAVRAS-CHAVE
Potenciaisevocados;
Vestíbulodo
labirinto;
Nervovestibular;
Eletromiografia
Reprodutibilidade(teste-reteste)dopotencialevocadomiogênicovestibular
Resumo
Introduc¸ão: Aindanão existeconsenso quantoao melhor estímuloacústicoutilizadopara a captac¸ãodopotencialevocadomiogênicovestibular(PEMV).Respostasamplassãoobservadas paraestímulosdebaixafrequência,porémestudosrecentesaindautilizamcliques.A repro-dutibilidadedostrac¸adoséumimportanteparâmetrodeanáliseparaobservaraconfiabilidade dasrespostas.
Objetivo: Verificarareprodutibilidadedosparâmetros‘‘latênciaeamplitudedasondasp13e n23’’doPEMVparaestímuloscomdiferentesfrequênciasdeestímulosdotipotoneburst,e definiramelhorfrequênciadeteste.
Método: Estudode coorte-transversal.Captou-se PEMVem 156 orelhas,nomúsculo estern-ocleidomastóideo,com100estímulosdotipotoneburstnasfrequênciasde250,500,1000e 2000Hzenívelsonoro95dBNAn,registradostrêsvezesdecadalado.
Resultados: Foramconstatadassimilaridadesparalatênciasdep13en23dopotencialestudado nos três momentos comestímulos tone burstem 250,500, 1000Hz, e diferenc¸as entre as captac¸õesdessepotencial(P<0.001)paraafrequênciade2000Hz.Aanálisedaamplitudede p13en23semostrousemelhante,noteste-reteste,paratodasasfrequênciasanalisadas. Conclusão:Existe reprodutibilidade daslatências eamplitudes dep13 e n23 doPEMV para estímulostoneburstnasfrequênciasde250,500e1000Hz.
©2014Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
To capture the vestibular evoked myogenic potential
(VEMP), sound stimuli of tone-burst type at frequencies
between100and3200Hz1---4orclicks5,6maybeused.In
gen-eral,toneburstsaremoreeffectivethanclicksforobtaining VEMP.Amongtone-burststimuli,lowfrequencies(≤1000Hz) aremoreeffective thanhigh frequencies,7,8 and500Hzis
themostcommonlyused.2,8,9
Thereis stillnoconsensusintheliteraturewithregard tothe best acoustic stimulusused for VEMP recording. A recentstudy10usedclickstimuli,whichstimulatetheregion
of sensitivity with a range 1000---4000Hz. Research shows thathigh-frequencystimuliresultinpoordefinitionofwaves p13andn23,andtheappearanceofvaguenessoftracing.7,8
VEMP waves present reproducibility for circumstances andparametersofcontrolledstimuli.Thereproducibilityof thetracingisanimportantanalyticalparametertoobserve thereliabilityofresponses.11
Todate,therearenostudiesinliterature(databases: Sci-ELO,LILACS,Scirus,ScienceDirect,andScopus)presenting thesamemethodologicaldesignadoptedinthisstudy,which aim to determine the reproducibility (test---retest) of the parameter‘‘latencyandamplitudeofwavesp13andn23’’ fortheVEMP,forstimuliwithdifferenttone-burst frequen-cies,andtodefinethebesttestfrequency.
Methods
Thiswasahistoricalcross-sectionalcohortstudyin accor-dance withResolution No. 196/96 of the National Health Council(ConselhoNacionaldeSaúde).Itwassubmittedto theResearchEthicsCommitteeoftheuniversitywherethe datawerecollected,andapprovedundernumber1010.The
datacollectionwas conductedfrom March2010 toMarch 2012.
Recordingsof VEMP werecollected from78 volunteers (156ears);40femaleand38malesubjectsagedbetween 18and31yearsold(21.28±2.90years).Thesubjectswere selectedby the following inclusion criteria: normal hear-ingthresholds,i.e.,≤20dB nHL,for frequencies between 250and8000Hzobtainedbypuretoneaudiometrytest;and astotympanometry,thesubjectswererequiredto demon-strateatypeAtympanogram.
Thefollowing exclusioncriteriawereadopted:changes inexternaland/ormiddleear;occupationalorleisurenoise exposure and/or ototoxic medication; presence of tinni-tus,vertigo,dizziness,orothercochleovestibularchanges; andpresenceofsystemicchangesthatcouldcontributeto cochleovestibularpathologies,suchasdiabetes, hyperten-sion,anddyslipidemiaand/orhormonalchanges.
VEMPtestswereperformedwithaspecificapparatusfor captureofthispotential,developedattheCenterfor Instru-mentation,Dosimetry,andRadiationProtection,Faculdade deFilosofia,CiênciaseLetrasdeRibeirãoPreto, Universi-dade de SãoPaulo (USP-FFCLRP),12 which is composed of
biological amplifiers, filters, an electrical protection sys-tem,andalogicsystemthatenablesadetailedinvestigation ofVEMP.This equipmentwasvalidatedwithgold-standard commercial equipment and has been used in previous studies.13---15
Amplitude (uV)
60
A
B
C
D
40
20
0
–20
–40
–60
–80
–100
Amplitude (uV)
60 80
40
20
0
–20
–40
–60
–80
–120 –100
0 10 20 30 40 50 Latency (ms)
Amplitude (uV)
60
40
20
0
–20
–40
–60
–80
–100
–120
0 10 20 30 40 50 Latency (ms)
Amplitude (uV)
60
40
20
0
–20
–40
–60
–80
–100
–120
0 10 20 30 40 50 Latency (ms)
0 10 20 30 40 50 Latency (ms)
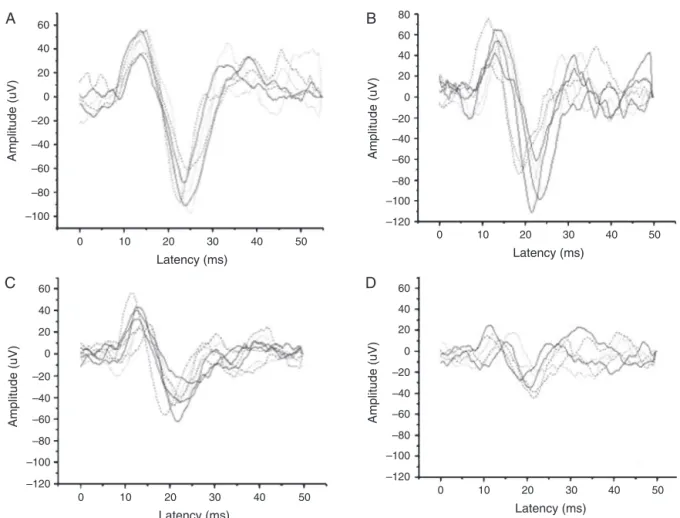
Figure1 Recordsofvestibularevokedmyogenicpotentialwavetracingsbytone-burststimulifrequency.
ToobtainarecordingofVEMPinthesternocleidomastoid muscle,thepatientremainedseated,withmaximumlateral rotationoftheheadtothesidecontralateraltothe stimu-lus,andmaintainedatoniccontractionofthemusclearound 60---80V,which wasmonitored bymeansof surface
elec-tromyography.Thestimuli presentedthroughER-3A insert earphoneswasintroducedintherightafferentand, subse-quently,wasrepeatedin the leftafferent.The responses werereplicated,thatis,recordedthreetimesontheright sideandthreetimesontheleftside.Thosetestspresenting vaguenessoftherecordingofthewavesintheVEMPtracing, duetothepresenceofnoiseandartifacts,wereexcluded.
On examination of VEMP, 100 tone-burst stimuli were averaged at frequencies of 250, 500, 1000, and 2000Hz, withadurationof10ms(uphill:4ms,plateau:2ms, down-hill:4ms), arate of5Hz, asoundintensity levelof 95dB nHL,and withtheuse of aband-pass filterof 5---2200Hz. Therecordingswereperformedin50mswindows.
p13 latency was defined by the positive polarity of a biphasic waveform that appears approximately at 13ms, andn23latency wasdefinedbyanegativepolarityofthe biphasicwaveformthatappearsatapproximately23ms.
Theamplitudeofthewavep13wasmeasuredfromthe zero referenceto themost positivepeak of the wave on theCartesianY-axis.Conversely,theamplitudeofwaven23 wasmeasuredfromthezeroreferencetothemostnegative peakofthewaveontheCartesianYaxis.Bothwaveswere measuredinmicrovolts.
PASWStatisticsdata editorsoftware(version17.0)was usedfor dataanalysis.The Shapiro---Wilktest wasapplied to test the normalityof the sample. Student’s t-test was usedforindependentanalysisof waverecordingsof VEMP between ears. The analysis of variance (ANOVA) test was used to compare the different recordings of VEMP, for parameters‘‘latencyandamplitudeofwavesp13andn23’’, andTukey’sposthoctestwasusedfortheanalysisofVEMP parameters capturedby tone bursts of different frequen-cies.Valueswereconsideredsignificantforp≤0.05andan alphavalueof0.1wasadopted.
Results
VEMPwasrecordedwithappropriatemorphologyand ampli-tudeinallsubjectsatfrequenciesof250Hzand500Hz,in 97.5% at 1000Hz,and in 87% at 2000Hz. Thus, no defini-tionofVEMPwavetracingswasobservedintwosubjectsfor the frequency of1000Hz, andin 10 subjectsfor 2000Hz, bilaterally.
TherecordingsofVEMPwavetracingsbystimulation fre-quencyareshowninFig.1.
WiththeindependentuseofStudent’st-test,no signif-icantdifferencewasfoundbetweenright andleftearsfor latencies and amplitudes of p13and n23 with tone-burst stimuliof250,500,1000,and2000Hz,consideringp-values
Table1 Meanvaluesandstandarddeviationoftheregisteroflatencyforwavep13(test---retest)ofvestibularevokedmyogenic potentialrecordedbydifferenttone-burststimuli,a(n=156forfrequenciesof250and500Hz,n=152for1000Hz,andn=136
for2000Hz).
Stimulustone-burst(Hz) Latencyofp13(ms) p-value Register1 Register2 Register3
250 13.61±2.20 13.66±2.10 13.52±2.05 0.52b
500 14.14±1.38 14.23±1.36 14.33±1.27 0.40b
1000 13.74±2.28 13.98±2.1 13.81±2.16 0.61b
2000 14.53±3.23 20.37±7.25 17.72±5.4 <0.001b
ms,milliseconds;Hz,Hertz.
a Dataexpressedasmean±standarddeviation. b Analysisofvariancetest.
Table2 Meanvaluesandstandarddeviationofregisteroflatencyforwaven23(test---retest)ofvestibularevokedmyogenic potentialrecordedbydifferenttone-burststimuli,a(n=156forfrequenciesof250and500Hz,n=152for1000Hz,andn=136
for2000Hz).
Stimulustone-burst(Hz) Latencyofn23(ms) p-valueb
Register1 Register2 Register3
250 23.25±2.04 23.20±1.93 23.41±2.89 0.64b
500 24.34±2.22 24.45±2.26 24.49±2.5 0.52b
1000 24.48±3.05 24.55±3.15 24.61±3.3 0.24b
2000 19.40±5.37 25.28±3.44 22.78±4.8 <0.001b
ms,milliseconds;Hz,Hertz.
a Dataexpressedasmean±standarddeviation. b Analysisofvariancetest.
Thelatenciesofp13forVEMPrecordingweresimilar (dif-ferenceofupto0.24ms),inthetest---retest,fortone-burst (TB) stimuli of 250, 500,and 1000Hz,with nodifference for p-values ≤0.05. There was significant differenceonly forTB-2000Hz(differenceequalto5.84ms),withp<0.001 (Table1).
As for n23 latencies, the smallest differencebetween VEMPrecordingsinthetest---retestwasfortheTB-stimulus of 1000Hz (0.13ms), followed by TB-500Hz(0.15ms)and TB-250Hz (0.21ms), respectively. Statistically significant differences were found only for the parameter ‘‘latency ofwaven23’’,betweenrecordings, forTB-2000Hz,witha differenceequalto5.88msandp<0.001(Table2).
InTable3,thefindingsrelativetoparameter‘‘amplitude ofwavep13’’arelisted.Whencomparingthethreetracings ofthree differentmoments of VEMPcaptures, the differ-encesfound(3.54;1.46;0.22,and0.34V,respectively,for
thefrequencies of 250, 500, 1000 and 2000Hz) were not statisticallysignificant.
Just as for the amplitude of p13, a similarity for the parameter‘‘amplitudeofwaven23’’wasalsoobservedin thetest---retestin allfrequenciesanalyzed, withvalues upto2.43V(Table4).
Comparing the stimuli frequencies used for recording VEMPwiththeuseofTukey’sposthoctest,significant dif-ferenceswereonlyfoundforp13andp23latenciesbetween
Table3 Mean valuesand standarddeviation ofthe amplitudeof wave p13 (test---retest) for vestibular evoked myogenic potentialrecordedby differenttone-burst stimuli,a (n=156for thefrequencies of250and500Hz,n=152 for1000Hz, and
n=136for2000Hz).
Stimulustone-burst(Hz) Amplitudeofp13(V) p-value
Register1 Register2 Register3
250 27.17±14.75 30.71±19.57 29.71±12.8 0.37b
500 24.62±12.47 26.08±13.18 25.76±13.5 0.22b
1000 14.18±9.72 13.99±9.96 14.21±9.10 0.20b
2000 10.63±7.35 10.97±6.48 10.72±7.45 0.65b
V,microvolts;Hz,Hertz.
Table4 Meanvaluesandstandarddeviationofamplitudeofwaven23(test---retest)ofvestibularevokedmyogenicpotential recordedbydifferenttone-burststimuli,a(n=156forfrequenciesof250and500Hz,n=152for1000Hz,andn=136for2000Hz).
Stimulustone-burst(Hz) Amplitudeofn23(V) p-Value
Register1 Register2 Register3
250 41.71±21.67 39.57±20.24 42.00±20.23 0.32b
500 33.01±18.05 34.04±17.83 33.58±18.60 0.96b
1000 16.15±11.34 16.33±11.63 16.48±11.34 0.85b
2000 10.88±6.75 10.92±6.61 10.64±6.23 0.67b
V,microvolts;Hz,Hertz.
aDataexpressedasmean±standarddeviation. b Analysisofvariancetest.
frequenciesof250and2000Hz,withp<0.04andp<0.001, respectively.
Inthe analysisofamplitudes, it wasobserved thatthe wave p13 had a different presentation, when comparing thefrequenciesof250and500Hzwithstimuliat1000and 2000Hz (p<0.001), as well asbetween 1000 and 2000Hz (p=0.04).Inthewaven23,thisparameterwasdifferentat allfrequenciesofstimulationforvaluesofp<0.005.Thus, itisnotedthat,onaverage,stimuliwithlowerfrequencies provide arecording of VEMP responses withlarger ampli-tudes.
Discussion
AnalyzingtheseVEMPresults,itwasfoundthatthelackof responseswasrestrictedtotone-bursts of1000(2.5%)and 2000Hz (13%). Thus, considering that all subjects had no hearingand/orvestibularchanges,itcanbeseenthatthere isgreatersaccularsensitivitytolowerfrequencies,14---17and
thatVEMPscapturedwithstimuliofhigherfrequenciesmay notshowclearresults,resultinginvaguenessforwavesp13 andn23.3
Itisknownthatthelatencydoesnotdependonstimulus intensity,levelofelectromyographicvoltage,andage,and alsohashighreproducibility.1,18Thus,thelatenciesofwaves
p13andn23areimportantclinicalparametersandshouldbe consideredintheanalysisofVEMPresponses,whichshould bethoughtofasbasedonnormalvalues.2,18 Thus,asthere
isnointerference fromother factors(besides thetypeof stimulus),itcanbepresumed,inthelatencyanalysis,that thedifferencesfoundbetweenVEMPcaptures(test---retest) arederivedsolelyfromthestimulusused.
Althoughresearchshowssaccularsensitivityintheregion offrequenciesbetween100and3200Hz,3lowfrequencies
shouldbeusedduringVEMPrecording,3,13---17 since,besides
havingmoredefinedwaves,thepresentstudyshowed pres-enceofreproducibilityforfrequencies≤1000Hz.
The parameter‘‘amplitude’’,importantintheanalysis of VEMPwaves, is dependent onmany factors, including: stimulustypeandlevelofelectromyographic voltage.The presentdatademonstratethatstimuliwithlower frequen-cies (250 and 500Hz) show, on average, potentials with higheramplitudes,whencomparedtoresponsesatstimuli withfrequenciesof1000and2000Hz.Thisfindingwasalso confirmedbypreviousstudies.9
As the amplitude suffers interference of the variable ‘‘muscletension’’,the stateof contractionof these mus-cles wasmonitored.7,8 This mayexplain the absenceof a
statisticallysignificant differencebetweenthetest---retest fortheamplitudesofp13andn23(forallfrequenciesused). This finding reinforces the principle that the parameter ‘‘amplitude’’remains constantforrecordingsin thesame subjectatdifferenttimes,whenallparametersof stimula-tionandcapturearecontrolled.
A recent study19 determined the frequency of 500Hz
as the stimulus parameter that should be used clinically for VEMP responserecording. In thepresent study, itwas observedthatthefrequenciesof250and500Hzarestimuli that provide responses with larger amplitudes and lower latenciesthanthefrequenciesof1000and2000Hz.Itwas alsofoundthattheparameter‘‘amplitudeofwaven23’’was differentamongfrequencies,withhighestmeanvaluesfor 250Hz.This canbe explainedbythegraviceptive charac-teristicsofthesensorialorganresponsibleforthisresponse (saccule).3,14,15,17,20
Conclusion
Reproducibilitywasobserved forp13andn23 latencies of VEMPtotone-burststimuliatfrequenciesof250,500,and 1000Hz.However,noreproducibilityoftracingsforstimuli at 2000Hz was observed. The parameter ‘‘amplitude’’ showedreproducibilityfor allfrequencies analyzed.Thus, stimuli of 250, 500, and 1000Hz can be used for clinical recordingofVEMP;however,thefrequencyof250Hzproved tobethemostsuitable,asitprovidesthelargestamplitude valuesforwaven23.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
2.BurkardRF,EggermontJJ,DonM.Auditoryevokedpotentials: basicprinciplesand clinicalapplication.Philadelphia: Lippin-cottWilliams&Wilkins;2007.
3.Sheykholeslami K, Kermany MH, Kaga K. Frequency sen-sitivity range of the saccule to bone-conducted stimuli measuredbyvestibularevokedmyogenicpotencials.HearRes. 2001;160:58---62.
4.TimmerFCA, Zhou G, Guinan JJ, Kujawa SG, Herrmann BS, Rauch SD. Vestibular evoked myogenic potencial (VEMP) in patientswith Ménière’s Diseasewith drop attacks. Laryngo-scope.2006;116:776---9.
5.HuangT,SuH,ChengP.Effectofclickdurationon vestibular-evoked myogenic potencials. Acta Otolaryngol (Stockh). 2005;125:141---4.
6.KelschTA,SchaeferLA, EsquivelCR. Vestibular evoked myo-genic potencials in young children: test parameters and normativedata.Laryngoscope.2006;116:895---900.
7.AkinF,MurnaneO, PanusP,CaruthersS,WilkinsonA,Proffitt T.TheinfluenceofvoluntarytonicEMGlevelonthe vestibular-evokedmyogenicpotencial.JRehabilResDev.2004;41:473---80. 8.MurofushiT,MatsuzakiM,WuC.Shorttoneburst-evoked myo-genicpotencialsonthesternocleidomastoidmuscle:arethese potentialsalsoofvestibularorigin?ArchOtolaryngolHeadNeck Surg.1999;125:660---4.
9.HallJW.Newhandbookforauditoryevokedresponses.2rded. Boston:PearsonEducation;2006.
10.Vir D, Silky L, Panda N. Test retest reliability of vesti-bularevokedmyogenicpotentials.ClinNeurophysiol.2011;122, 1,S10.
11.IsaradisaikulS,StrongDA,MousheyJM,GabbardSA,AckleySR, JenkinsHA.Reliabilityofvestibularevokedmyogenicpotentials inhealthysubjects.OtolNeurotol.2008;29:542---4.
12.Oliveira AC, Colafêmina JF, Menezes PL. Vestibular evoked myogenicpotential: we proposea new instrument. IntArch otorhinolaryngol.2010;14:410---6.
13.CarnaúbaATL,FariasVV,SantosN,OliveiraAC,RodriguesRGS, MenezesPL.Influenceofgenderonthevestibularevoked myo-genicpotential.BrazJOtorhinolaryngol.2011;77:245---8. 14.Oliveira AC, Colefêmina JF, Menezes PL. Vestibular evoked
myogenicpotentialsusinglowfrequencystimuli.BrazJ Otorhi-nolaryngol.2011;77:706---10.
15.Oliveira-BarretoAC,ColefêminaJF,MenezesPL.Saccular sen-sitivity function measured by vestibular evoked myogenic potential.ActaOtolaryngol(Stockh).2011.EarlyOnline:1---6. 16.ToddNPM, RosengrenSM,ColebatchJG.Tuning and
sensitiv-ityofthehumanvestibularsystemtolow-frequencyvibration. NeurosciLett.2008;444:36---41.
17.TownsendG, Cody D.Theaverage inion responseevoked by acousticstimulation:itsrelationtothesacculus.AnnOtol Rhi-nolLaryngol.1971;80:121---31.
18.Damen MJ. Vestibular evoked myogenic potencial (VEMP), Clinical application of the threshold. Eindhoven: Technische UniversiteitEindhoven;2007.
19.IsaradisaikulS,NavacharoenN,HanprasertpongC,Kangsanarak J.Cervicalvestibular-evokedmyogenicpotentials:normsand protocols.IntJOtolaryngol.2012:1---7.