www.rpped.com.br
REVISTA
PAULISTA
DE
PEDIATRIA
ORIGINAL
ARTICLE
High
prevalence
of
physical
inactivity
among
adolescents
living
with
HIV/AIDS
Luana
Fiengo
Tanaka
a,∗,
Maria
do
Rosário
Dias
de
Oliveira
Latorre
a,
Aline
Medeiros
da
Silva
a,
Thais
Claudia
Roma
de
Oliveira
Konstantyner
a,
Stela
Verzinhasse
Peres
a,
Heloisa
Helena
de
Sousa
Marques
baUniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil bInstitutodaCrianc¸a,SãoPaulo,SP,Brazil
Received1September2014;accepted25December2014 Availableonline23June2015
KEYWORDS
Adolescent; HIV/AIDS; Physicalactivity; Sedentarylifestyle
Abstract
Objective: ToassesstheprevalenceofphysicalinactivityamongadolescentswithHIV/AIDS,as wellasassociatedfactors.
Methods: Ninety-oneadolescents(from10to19yearsold)withHIV/AIDSwhoarepatientsata universityfollow-upservicewereinterviewed.Anthropometricdata(weight,height,andwaist circumference)weremeasuredtwice;clinicalinformationwasobtainedfrommedicalrecords, andhabitualphysicalactivitywasassessedbyaquestionnaireproposedbyFlorindoetal.The cutoffpointforsedentarinesswas300minutes/week.
Results: Theprevalenceofinadequateheightforage,malnutrition, andoverweight/obesity was 15.4%,9.9%and12.1%, respectively.The mostcommonphysicalactivities were soccer (44.4%),volleyball(14.4%)andcycling(7.8%).Themediantimesspentwithphysicalactivity andwalking/bicyclingtoschoolwere141minand39min,respectively.Mostadolescents(71.4%) weresedentaryandthisproportionwashigheramonggirls(p=0.046).
Conclusions: A highprevalence ofphysicalinactivity among adolescentswithHIV/AIDS was observed,similartothegeneralpopulation.Promotingphysicalactivityamong adolescents, especiallyamonggirlswithHIV/AIDS,aswellasmonitoringitshouldbepartofthefollow-up routineofthesepatients.
© 2015Sociedadede Pediatria de SãoPaulo. Published by Elsevier Editora Ltda.All rights reserved.
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rpped.2014.12.003
∗Correspondingauthor.
E-mail:[email protected](L.F.Tanaka).
PALAVRAS-CHAVE
Adolescente; HIV/Aids; Atividadefísica; Estilodevida sedentário
AltaprevalênciadesedentarismoemadolescentesquevivemcomHIV/Aids
Resumo
Objetivo: Verificar aprevalência de sedentarismo entre adolescentescom HIV/Aids e seus fatoresassociados.
Métodos: Foramentrevistados91adolescentesde10a19anos,comHIV/Aids,em acompan-hamentoemumaunidadedeinfectologiauniversitária.Foramcoletadosdadosantropométricos (peso,alturaecircunferênciadacintura)emduplicata,informac¸õesclínicasforamobtidasnos prontuáriosmédicoseapráticadeatividadefísicahabitualfoimedidapormeiodoquestionário propostoporFlorindoetal.Opontodecorteparasedentarismofoide300minutos/semana. Resultados: As prevalências de altura inadequada para idade, desnutric¸ão e sobrepeso/obesidade foram de 15,4%, 9,9% e 12,1%, respectivamente. As atividades físi-casmaiscitadasforam:futebol(44,4%),voleibol(14,4%)eandardebicicleta(7,8%).Ostempos medianosdispendidoscomapráticadeatividadefísicaecaminhando/andando debicicleta atéaescolaforamde141minutose39minutos,respectivamente.Amaioriadosadolescentes (71,4%)erasedentária,proporc¸ãomaiorentreasmeninas(p=0,046).
Conclusões: FoiobservadaaltaprevalênciadesedentarismoentreadolescentescomHIV/Aids, prevalênciaessasemelhanteàquelaobservadanapopulac¸ãogeral.Promoverapráticade ativi-dadefísicaentreadolescentes---especialmenteentremeninas---comHIV/Aids,assimcomo monitorá-la,devefazerpartedarotinadeacompanhamentodessespacientes.
© 2015Sociedadede Pediatriade SãoPaulo. Publicado porElsevier Editora Ltda.Todosos direitosreservados.
Introduction
Approximately 9% of prematuredeaths (about 5.3 million ofthe57milliondeathsin2008)and6---10%ofmajor non-communicablechronicdiseases suchasdiabetes,coronary heartdiseaseandbreastandcoloncancercanbeattributed tophysicalinactivity.Ifsedentaryindividualsbecame phys-icallyactive,itisestimatedthatworldwidelifeexpectancy would increaseby 0.68 years.1 Astudy carriedout in the
United Stateswithindividuals aged 50years or older and physicallyinactiveshowedthatbecomingphysicallyactive would representa gainof approximately1.3---4.7 yearsin lifeexpectancy.Thus,physical inactivity iscomparableto otherimportantmodifiableriskfactors,suchassmokingand obesity.2
InpatientswithHIV/AIDS,physicalactivitypracticecan integratenon-pharmacologicalapproachestodisease con-trol.Since the introduction of highlyactive antiretroviral therapy (HAART), metabolic and morphological changes startedtobeofconcernforpatientsundergoingtreatment andhealthprofessionals.Thesechangesincludelossoffat inthefacialregion,theupperandlowerlimbs(lipoatrophy) andfataccumulationintheabdominalandcervicalregions aswellasbreasts(lipohypertrophy),inadditiontoincrease in levels of total cholesterol and serumtriglycerides and increasedperipheralinsulinresistance.3
Physical activity, however, can help mitigate the side effectsofthistypetherapy.Suchistheimportanceofthis issue that the Ministry of Health (MH) launched in 2012, thebooklet‘‘Physicalactivityrecommendationsfor individ-ualswithHIVandAIDS.’’AccordingtotheMH,someofthe practicalbenefitsofphysicalactivitybythispopulationare theimmunesystemstimulationanddepressionrelief, pre-ventingorreducingsideeffectsoftheuseofantiretroviral
therapy.4 OtherinstitutionssuchastheFederal Councilof
PhysicalEducation (Conselho Federal de Educac¸ãoFísica) alsorecommendphysicalactivityforthispopulation.5
InspiteofitsimportanceforindividualswithHIV/AIDS, fewstudieshaveassessedthepracticeof physicalactivity by the adolescent population. The aim of this study was todetermine the prevalence of physical inactivity among adolescentswithHIV/AIDSandassociatedfactors.
Method
Thisisacross-sectionalstudynestedinacohortofchildren andadolescentsliving withHIV/AIDStreated atthe Infec-tiousDiseases Unit ofInstituto daCrianc¸a ofHospital das ClínicasdaFaculdade deMedicina ofUniversidadedeSão Paulo.
Between April and September 2010, 124 adolescents aged10---19 yearsenrolledin thatservicewereidentified. Of these, eight had not attended the scheduled visits in theprevious six months; ten werenot found; tenmissed the scheduled evaluation; three refused to participate; and two were excluded due to health problems that impairedthepracticeofphysicalactivity.
A total of 91 adolescents were interviewed for this study,which correspondsto73% ofeligiblepatients.They answeredthephysicalactivityassessmentquestionnairefor adolescentsdevelopedandvalidatedbyFlorindoetal.6
Section II questions (16 and 17) consider the physical activitiesrelatedtomobilitytoschool(walkingorcycling). The score of mobility toschool is the time spent onthis activitymultipliedbyfive.Thesumofthescoresofsections 1 and 2 generates the final score ‘‘minutes of weekly physical activity.’’ Based on this value, the adolescents wereclassified assedentary(<300minof physical activity per week) or active (≥300min/week), according to the
cutoffproposedbyPateetal.7
Biochemical tests analyzed in this study refer to the threemonthsbefore or after theinterview. The informa-tionwascollectedfrommedicalrecordsandsocioeconomic datawereobtainedfromaquestionnaireansweredby par-ents/tutorsatthetimeofinterview.
Theanthropometricassessmentofadolescentswas car-riedoutbyapreviouslytrainednutritionist. Thefollowing were measured in duplicate: weight (kg), using a digital scale; height(meters) usinga stadiometer, andwaist cir-cumference(cm),usinganinelasticmeasuringtape.WHO Anthroplussoftware,version 1.0.3,wasused tocalculate theheightz-scoreandBMIforage.8
Measures of central tendency as well as absolute and relative frequencies were used to characterize the sample. The chi-square test was used to test the asso-ciation between physical inactivity and the dichotomous independentvariables.Forquantitativeindependent varia-bles, we first verified the normal distribution using the Kolmogorov---Smirnovtestandthenthemeandifferencetest wasapplied according tothe distribution (Mann---Whitney test for nonparametric and Student’s ttest for paramet-ricvariables).All variableswithp<0.20 wereselected for themultivariate model,using thestepwise forward strat-egy.TheSPSS(CopyrightIBMCorporation1994,2012.SPSS forWindows,Version15.0.,USA)wasusedforallstatistical analyses.
This study was approved by the Research Ethics Com-mittee of Faculdade de Saúde Pública and Faculdade de Medicina da Universidade de São Paulo (protocol #1667/2007,0144/10and2239/2011).Thevolunteers(aged >18 years)or parents/tutors (of patients aged <18 years) signedthefreeandinformedconsentform.
Results
Medianagewas1.7yearsatthediagnosisofHIVinfection and14.9 yearsat thetime ofthe interview. Most adoles-cents(54.9%)werefemales,wereverticallyinfected(95.6%) andusedantiretroviraltherapy(97.8%).Themediantimeof antiretroviraltherapyusewas11years.
Ten respondents (11.0%) lived in halfway houses. Of theadolescents living withtheir families, 62.5% had par-ents(biological/adoptive)astheircaregiversandtheothers hadotherrelatives(uncles/aunts,siblingsorgrandparents). Mostoftheadolescents’families(76.9%)livedwithuptoone minimumwagepercapita(Table1).
Theprevalence ofinadequateheightforage, malnutri-tionandoverweight/obesitywere15.4%(95%CI=8.0,22.8), 9.9%(95%CI=3.8;16.0)and12.1%(95%CI=5.4,18.8), respec-tively.
Regarding laboratory tests, 74.4% of the adolescents had low HDL-cholesterol and 36.4% had alerted levels of
Table1 Numberandpercentageofadolescents,according to sociodemographic characteristics. Instituto daCrianc¸a, 2010.
Variables n %
Gender
Male 41 45.1
Ethnicity
Caucasian 41 45.1
Ageatdiagnosis(HIV)
0---2years 51 56.0
Ageatthestudy
10to12years 25 27.6
13to15years 33 36.3
16to20years 33 36.3
Modeoftransmission
Vertical 87 95.6
BloodTransfusion 1 1.1
Indeterminate 3 3.3
Useofantiretroviraltherapy
Yes 89 97.8
Typeofantiretroviraltherapya
Doubletherapy 11 12.4
Tripletherapy 68 76.4
Quadrupletherapy 10 11.2
Placeofresidence
Home 81 89.0
Caregiverb
Biological/adoptiveparents 51 63.0
Percapitaincomec
<1minimumwage 50 76.9
Overweight/obesity
Yes 11 12.1
Alteredtotalcholesterold
Yes 32 36.0
AlteredLDL-cholesterole
Yes 14 16.7
AlteredHDL-cholesterolf
Yes 61 74.4
AlteredTriglyceridesf
Yes 32 36.4
Sedentarylifestyle
Yes 65 71.4
a Onlyforadolescentsreceivingantiretroviraltherapy. b Onlyforadolescentsthatlivedwiththeirfamilies.
c Calculationsbased oncurrent minimumwagein 2010(R$
510.00).
Table2 Prevalenceofadolescentsaccordingto indepen-dent variables and physicalactivity. Instituto da Crianc¸a, 2010.
Variables Sedentary(%) Active(%) p-value
Gender 0.046
Male 61.0 39.0
Female 80.0 20.0
Ethnicity 0.286
Caucasian 65.9 34.1
Non-Caucasian 76.0 24.0
Placeofresidence 0.222
Family 69.5 30.5
Halfwayhouses 89.9 11.1
Caregivera 0.093
Biological/ adoptive parents
62.0 38.0
Otherfamily members
80.0 20.0
Percapita incomeb
0.503
<1MW 26.7 73.3
≥1MW 36.0 64.0
Overweight/obesity 0.186
Yes 54.5 45.5
No 73.7 26.3
UndetectableHIV viralloadc
0.791
Yes 68.8 31.2
No 72.9 27.1
Current
immunosuppressiond
0.657
Yes 70.7 29.3
No 77.8 22.2
a Onlyfortheadolescentsthatlivedwiththeirfamilies. b Calculationsbasedonthecurrentminimumwage(MW) in 2010(R$510.00).
c n=88adolescentswithavailablelaboratorytests. d Consideringpatients’currentCDCclassification.
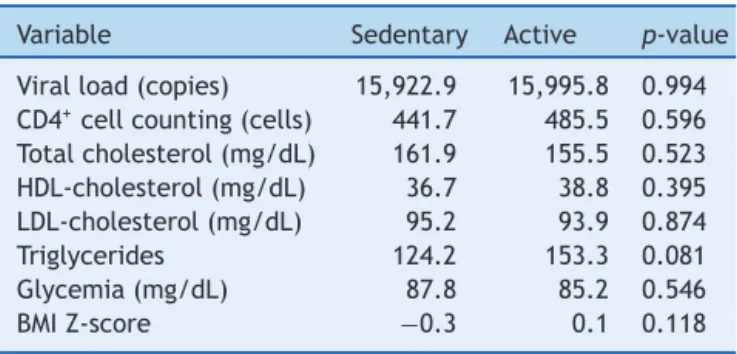
Table3 Comparisonofbiochemicalparametersbetween sedentaryandactiveadolescents.InstitutodaCrianc¸a,2010.
Variable Sedentary Active p-value
Viralload(copies) 15,922.9 15,995.8 0.994 CD4+cellcounting(cells) 441.7 485.5 0.596 Totalcholesterol(mg/dL) 161.9 155.5 0.523 HDL-cholesterol(mg/dL) 36.7 38.8 0.395 LDL-cholesterol(mg/dL) 95.2 93.9 0.874
Triglycerides 124.2 153.3 0.081
Glycemia(mg/dL) 87.8 85.2 0.546
BMIZ-score −0.3 0.1 0.118
triglycerides.Of the total,32 (36.4%) adolescentshad an undetectableviralload.
Thephysicalactivitiesmostfrequentlymentionedbythe adolescents were: soccer (44.4%), volleyball (14.4%) and cycling(7.8%).The mediantimes spentonthepracticeof physicalactivityandwalking/cyclingtoschoolwere, respec-tively,141minand39min.Oftheinterviewedadolescents, 29(31.9%)saidtheydid notpracticeanytypeof physical activity.
High prevalence of physical inactivity was observed among the adolescents: 71.4% (95% CI=62.1; 80.7), with a higher proportion of girls (girls 80.0% versus 61.0% boys; p=0.046). The univariate analysis between physical inactivityandtheotherindependentvariablesfoundno sta-tisticallysignificantassociations(Table2).
Therewasnostatistical differencebetween themeans ofbiochemicaltestsandBMIz-scorewhencomparing seden-taryadolescentsandactiveones(Table3).
Thefinalmodelchosenwastheunivariatemodel (seden-tary lifestyle versus gender) --- as the other dependent variableswerenotstatisticallysignificantinthetested mul-tivariate models --- using the stepwise forward technique (Table4).
Discussion
The present study found a high prevalence of physical inactivity among adolescents living with HIV/AIDS, which washigher in girls. Other assessed factors, suchas place
Table4 Logisticregressionmodels.InstitutodaCrianc¸a,2010.
Genderb Caregiverc Overweightd p-value
Model1a OR 2.56 0.045
CI [1.01;6.52]
Model2 OR 2.88 2.45 0.024
CI [1.06;7.81] [0.82;7.29]
Model3 OR 2.61 0.41 0.058
CI [1.01;6.71] [0.11;1.54]
a Selectedmodel. b Maleasreference.
of residence, caregiver and income, as well as anthro-pometric data, were not associated with the sedentary lifestyle.Regarding the typeof exercise practicedby the adolescents,themostcommonweresoccer,volleyballand cycling.
The findings of the present study are similar to those found inother publications that investigatedthe practice ofphysicalactivityamongadolescentsinthegeneral popu-lationinBrazilandworldwide.9---15
TheNationalSurveyonSchoolchildren’sHealth(Pesquisa NacionaldeSaúdedoEscolar---PeNSE)carriedoutinthe cap-italsandtheFederalDistrictofBrazilevaluatedthephysical activitypracticeonthesevendayspriortotheinterview. Thecutoffusedwasalso300minofphysicalactivity/week. Ofthetotal,56.9%oftheadolescentsweresedentary,with thisbehaviorbeingmoreprevalentamonggirls(68.7%girls versus43.8%boys).Anotherassociationidentifiedbythe sur-veywas a higherprevalence of physical inactivity among publicschoolstudentswhencomparedtostudentsfrom pri-vateschools.13
It is noteworthy that in the study by Guthold et al,9
which analyzed data on physical activity of adolescents aged13---15yearsfrom34countriesanddidincludeBrazil, observed only one exception regarding the proportion of sedentary girls versus boys: in Zambia, where there was a higher proportion of sedentary boys. A study of 177 adolescents (100 girls and 77 boys) investigated the per-ceptionof physical activity behavior amonggirls, through focal groups. Both boys and girls described active girls as ‘‘too aggressive’’. Boys often considered physically activegirlsas‘‘tooathletic’’.Thistypeofperceptionmay negatively influence the practice of physical activity by girls.16
However,duetotheuseofdifferenttools,bothindata collectionand theirsubsequent classification, comparison betweenstudiesbecomeslimited.Inspiteofthislimitation andbasedontheabovedata,itcanbeconcludedthat phys-icalinactivityisaglobalproblem,whichisprevalentinboth developinganddevelopedcountries.9---14
WefoundtwostudiescarriedoutinBrazilonthepractice ofphysicalactivityamongadolescentswithHIV/AIDS.One of these studies investigated children and adolescents (7---14years)orphanedby AIDS,of which only5.5% ofthe sample had positive serology for HIV. The study usedthe same questionnaire andcutoff usedin the present study, allowing direct comparison of results. The prevalence of sedentarylifestylewas42%.Twofindingsaresimilartothose found in this study: association between physical inactiv-ityandgenderandsports thatweremoreoftenpracticed (soccerandvolleyball).11
Theother studywascarriedoutinFlorianopolisandits primaryobjectivewastoevaluatebonedensityof48 ado-lescents with HIV/AIDS, withphysical activity being used as the control variable. Physical activity was measured usingpedometers,appliedforfivedays,includingtwodays at theweekend. The stepcount of 10,000 steps/day was used to classify the level of physical activity in adoles-cents. Approximately 70% of respondents had inadequate levels of physical activity. The authors found no statisti-callysignificantdifferenceinthemeanstepcountbetween genders.17
Physicalactivitypracticemaybean importantstrategy forthepreventionorcontrolofmetabolicand morpholog-icalalterations associatedwithinfectionandalsothe use of HAART. The review article by Fillipas et al18 analyzed
ninerandomizedcontrolledtrialscomparingthe interven-tion group (aerobic exercise) to the control group. The resultsshoweddecreasedbodymassindex,tricepsskinfold, totalbodyfat,waistcircumferenceandwaist-to-hipratio. Thepresentstudyfoundnoassociationbetween anthropo-metricvariablesandthepracticeofphysical activity.It is noteworthy that skinfoldthickness andhip circumference werenotmeasured, limitingthenutritionalassessment of thestudypopulation.
Astudy evaluating theeffect of a structurednutrition programandphysicalactivityinchildrenwithHIVfoundthat after24physical exercisesessions,therewasasignificant increasein muscularstrengthandenduranceandmaximal oxygenconsumption(VO2).19
Studies performed in Brazil analyzing physical activ-ityand lipodystrophy inadult patients withHIV/AIDSalso found similar associations. Florindo et al.20 observed an
inverse association between duration of physical activity andaccumulationofabdominalfat,whereasSegattoetal.21
observedalowerprevalenceoflipodystrophyinactive indi-viduals, when compared to sedentary ones. We did not observe similar associations in the present study. One of the possible reasons for this fact is the study design. As it is a cross-sectional study,both the exposure (socioeco-nomic variables and laboratory tests) and the outcome (physicalactivityorinactivity)weremeasuredatthesame moment.
Encouraging the practice of physical activity is part of the World Health Organization (WHO)’s agenda. After the publication of the World Health Report 2002, which disclosed that 60% of all deaths could be attributed to chronic diseases, the WHO Global Strategy onDiet, Phys-ical Activity and Health was launched. Thus, the WHO emphasized the need to reduce exposure to risk fac-tors forthe developmentof chronicdiseases, byadopting a healthy diet and regular physical activity. According to the WHO, ‘‘at least 30min of moderate physical activity on most days reduces the risk of cardiovascu-lar disease and diabetes, colon and breast cancer.’’22
Equally concerned with questions about physical
activ-ity among adolescents, the US government launched
the ‘‘2008 Physical Activity Guidelines for Americans’’.23
Together with the guidelines, ‘‘The NHANES --- National Youth Fitness Survey’’ was also created, which collected in 2012 information on the physical activity of children and adolescents aged 3---15 years living in the United States.24 The monitoring of physical activity in
adoles-cents by the multidisciplinary team can be used as an approach to assess physical activity over time and iden-tifychanges.Thehabitualphysicalactivityquestionnaireis easilyappliedandusessimplecalculationsandcanbe incor-porated into routine patient care without causing major problems.
therapy, aswell asboost the immune system and relieve depressionsymptoms.
Funding
Fundac¸ão de Amparo à Pesquisa do Estado de São Paulo --- FAPESP (processes:#10/01187-9 and#08/53322-7), Con-selhoNacionaldeDesenvolvimentoCientíficoeTecnológico --- CNPq (process: #135885/2011-4) and Coordenac¸ão de Aperfeic¸oamentodePessoaldeNívelSuperior---CAPES (Mas-ter’sDegreeGrantintheSocialDemandProgram).
Conflicts
of
interest
AlineMedeirosdaSilvaiscurrentlyanemployeeatJanssen PharmaceuticalCompanies,butwashiredafterthepresent studywascarriedout.
Acknowledgments
We thank the medical team from Instituto da Crianc¸a: Samantha Brasil Andrade, Cláudia Menezes, Vera Lúcia MoysesBorelli, MariadeFátimaCarvalhoand Nádia Litvi-nov.Wealsothankthecollectionteam:SofiadeFátimada SilvaBarbosadeOliveira,FláviaMoniqueSantosandElissa CarolinaMendesfortheirhelp.
References
1.LeeIM,ShiromaEJ,LobeloF,PuskaP,BlairSN,KatzmarzykPT. Effectofphysicalinactivityonmajornon-communicable dis-eases worldwide: an analysis of burden of disease and life expectancy.Lancet.2012;380:219---29.
2.Franco OH, de Laet C,Peeters A, Jonker J, Mackenbach J, NusselderW. Effects of physical activity on life expectancy with cardiovascular disease. Arch Intern Med. 2005;165: 2355---60.
3.Leonard EG, McComsey GA. Antiretroviral therapy in HIV-infected children: the metabolic cost of improved survival. InfectDisClinNAm.2005;19:713---29.
4.Brasil---MinistériodaSaúde.SecretariadeVigilânciaemSaúde. DepartamentodeDST,AidseHepatitesVirais.Recomendac¸ões paraapráticadeatividadesfísicasparapessoasvivendocom HIVeAIDS.Brasília:MinistériodaSaúde;2012.
5.Conselho Federal Educac¸ão Física. AIDS e atividade física. RevistaEF.2008;28:20---2.
6.Florindo AA, Romero A, Peres SV, Silva MV, Slater B. Development and validation of a physical activity assess-ment questionnaire for adolescents. Rev Saude Publica. 2006;40:802---9.
7.PateRR,FreedsonPS,SallisJF,etal.Compliancewithphysical activityguidelines:prevalenceinapopulationofchildrenand youth.AnnEpidemiol.2002;12:303---8.
8.WorldHealth Organization. WHO AnthroPlus paraPC --- soft-ware.Availablefrom:http://www.who.int/entity/growthref/ tools/WHOAnthroPlussetup.exe[accessed02.04.14].
9.GutholdR,CowanMJ,AutenriethCS,KannL,RileyLM.Physical activity and sedentarybehavior amongschoolchildren:a 34-countrycomparison.JPediatr.2010;157:43---9.
10.Farias-Junior JC.Associationbetween prevalenceofphysical inactivity and indicators of socio-economic status in adoles-cents.RevBrasMedEsporte.2008;14:109---14.
11.BarrosCR,ZucchiEM,Franc¸aJunior I.Physicalactivitylevel among childrenand adolescentsorphaned byAIDS.Rev Bras Epidemiol.2010;13:446---56.
12.Silva KS, Nahas MV, Hoefelmann LP, Lopes AS, Oliveira ES. Associations between physical activity, body mass index, and sedentarybehaviors inadolescents. RevBrasEpidemiol. 2008;11:159---68.
13.Brasil---MinistériodaSaúde;InstitutoBrasileirodeGeografiae
Estatística;MinistériodoPlanejamento,Orc¸amentoeGestão.
PesquisaNacionaldeSaúdedoEscolar.Brasília:Ministérioda
Saúde;2010.
14.De Moraes AC, Guerra PH, Menezes PR. The worldwide prevalence of insufficientphysical activity in adolescents: a systematicreview.NutrHosp.2013;28:575---84.
15.Colley RC, Garriguet D, Janssen I, Craig CL, Clarke J, TremblayMS.PhysicalactivityofCanadianchildrenandyouth: accelerometerresultsfromthe2007to2009CanadianHealth MeasuresSurvey.StatisticsCanadaHealthReports,Ottawa,vol. 22;2011.p.1---9.
16.Vu MB, Murrie D, Jobe JB. Listening to girls and boys talk about girls’ physical activity behaviors. Health Educ Behav. 2006;33:81---96.
17.LimaLR,SilvaRC,GiulianoIdeC,SakunoT,BrincasSM,Carvalho AP.Bonemassinchildrenandadolescentsinfectedwithhuman immunodeficiencyvirus.JPediatr(RioJ).2013;89:91---9.
18.Fillipas S, Cherry CL, Cicuttini F, Smirneos L, Holland AE. The effects of exercise training on metabolic and morpho-logical outcomes for people living with HIV: a systematic reviewofrandomisedcontrolledtrials.HIVClinTrials.2010;11: 270---82.
19.Miller TL, Somarriba G, Kinnamon DD, Weinberg GA, Friedman LB, Scott GB. The effectof a structured exercise programonnutritionandfitnessoutcomesinhuman immuno-deficiencyvirus-infectedchildren.AIDSResHumRetroviruses. 2010;26:313---9.
20.FlorindoAA,deOliveiraLatorreMdoR,JaimePC,SeguradoAA. Leisuretimephysicalactivitypreventsaccumulationofcentral fatinHIV/AIDSsubjectsonhighlyactiveantiretroviraltherapy. IntJSTDAIDS.2007;18:692---6.
21.Segatto AF,FreitasJunior IF,SantosVR, etal.Lipodystrophy in HIV/AIDS patients with different levelsof physical activ-ity while on antiretroviral therapy. Rev Soc BrasMed Trop. 2011;44:420---4.
22.WorldHealth Organization. Global strategyon diet,physical activity,andhealth.Geneva:WHO;2004.
23.Health.gov [homepage on the Internet]. US Department
of Health and Human Services. Physical activity
guide-linesfor Americans.Available from:http://www.health.gov/
paguidelines/guidelines/[accessed01.10.14].