www.rpped.com.br
REVISTA
PAULISTA
DE
PEDIATRIA
ORIGINAL
ARTICLE
Factors
associated
with
abdominal
obesity
in
children
Matheus
Ribeiro
Theodósio
Fernandes
Melzer
∗,
Isabella
Mastrangi
Magrini,
Semíramis
Martins
Álvares
Domene,
Paula
Andrea
Martins
UniversidadeFederaldeSãoPaulo(Unifesp),CampusBaixadaSantista,Santos,SP,Brazil
Received5January2015;accepted21April2015 Availableonline24August2015
KEYWORDS
Nutritional epidemiology; Children;
Abdominalobesity; Waistcircumference
Abstract
Objective: Toidentifytheassociationofdietary,socioeconomicfactors,sedentarybehaviors andmaternalnutritionalstatuswithabdominalobesityinchildren.
Methods: Across-sectionalstudywithhousehold-basedsurvey,in36randomlyselectedcensus tractsinthecityofSantos,SP.357familieswereinterviewedandquestionnairesand anthropo-metricmeasurementswereappliedinmothersandtheir3---10years-oldchildren.Assessment ofabdominalobesity wasmade bymaternal andchild’swaistcircumferencemeasurement; for classificationusedcut-off pointsproposedbyWorldHealthOrganization(1998)and Tay-loretal.(2000)wereapplied.Theassociationbetweenvariableswasperformedbymultiple logisticregressionanalysis.
Results: 30.5%ofchildren hadabdominal obesity.Associationswith children’sandmaternal nutritionalstatusandhighsocioeconomicstatuswereshownintheunivariateanalysis.Inthe regressionmodel,children’sbodymassindexforage(OR=93.7;95%CI39.3---223.3),female gen-der(OR=4.1;95%CI 1.8---9.3)andmaternalabdominal obesity(OR=2.7;95%CI1.2---6.0)were significantly associated with children’s abdominal obesity, regardless ofthe socioeconomic status.
Conclusions: Abdominalobesityinchildrenseemstobeassociatedwithmaternalnutritional status,otherindicatorsoftheirownnutritionalstatusandfemalegender.Interventionprograms for controlofchildhood obesityandprevention ofmetabolicsyndromeshouldconsiderthe interactionofthenutritionalstatusofmothersandtheirchildren.
©2015SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-license(https://creativecommons.org/licenses/by/4.0/).
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rpped.2015.04.002
∗Correspondingauthor.
E-mail:[email protected](M.R.T.F.Melzer).
PALAVRAS-CHAVE
Epidemiologia nutricional; Crianc¸as;
Gorduraabdominal; Circunferênciada cintura
Fatoresassociadosaoacúmulodegorduraabdominalemcrianc¸as
Resumo
Objetivo: Identificarfatoresindividuais(dietéticos,comportamentosedentário)efamiliares (estado nutricionalmaterno enível socioeconômico) associados com oacúmulo degordura abdominaldecrianc¸as.
Métodos: Estudo dedelineamento transversal debasedomiciliar, em 36setores censitários sorteados aleatoriamente na cidade de Santos/SP. Foram entrevistadas 357 famílias para aplicac¸ãodequestionárioseaferic¸ãodemedidasantropométricasemmãesecrianc¸asde3-10 anos.A avaliac¸ãodoacúmulodegorduraabdominalfoifeitapelamedidadacircunferência dacinturademãesecrianc¸ascomousodarecomendac¸ãodaOrganizac¸ãoMundialdaSaúde (1998)eapropostadeTayloretal.(2000),respectivamente.Aassociac¸ãoentreasvariáveis foiverificadapormeioderegressãologísticamúltipla.
Resultados: Verificou-seque30,5%dascrianc¸asapresentaramacúmulodegorduraabdominal. Naanáliseunivariada,oacúmulodegorduraabdominalesteveassociadoaoestadonutricional maternoedacrianc¸aeaonívelsocioeconômicoelevado.Naanálisemultivariada,foram obser-vadasassociac¸õescomexcessodepesopeloíndicedemassa corporalparaidade(OR=93,7; IC95%39,3-233,3);serdosexofeminino(OR=4,1;IC95%1,8-9,3)eacúmulodegordura abdom-inalmaterno(OR=2,7;IC95%1,2-6);independentementedonívelsocioeconômico.
Conclusões: Oacúmulodegorduraabdominalemcrianc¸asmostrou-seassociadoaoestado nutri-cionalmaterno,aosindicadoresdeseupróprioestadonutricionaleaosexofeminino.Programas deintervenc¸ãoparacontroledaobesidadeinfantileprevenc¸ãodasíndromemetabólica rela-cionadaaoacúmulodegorduraabdominaldevemlevaremconsiderac¸ãoainterac¸ãodoestado nutricionaldemãeseseusfilhos.
©2015SociedadedePediatriadeS˜aoPaulo.PublicadoporElsevierEditoraLtda.Esteéumartigo OpenAccesssobalicençaCCBY(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
Theworldwideobesity epidemicisincreasingat an alarm-ing rate in childhood and can be observed in developing countries,whichhaveshownanincreaseintheprevalence ofchildhoodobesity inrecentdecades.1 InBrazil,astudy withasampleofchildrenaged7---10yearsshoweda preva-lenceofoverweightandobesityof26.7%forboysand34.6% forgirls.2
As a consequence of excessweight, abdominalobesity isassociatedwithcardiovascularriskfactorsandmetabolic disorders, which may already be present in childhood.3,4 Abdominal obesity is understood as the accumulation of fatintheabdominalregionassessedbyananthropometric and/orbodycompositionmeasurethatshowsavalueabove aspecificand sensitivecutoffpoint.4 Among themethods usedfor the diagnosis, waist circumference (WC), widely usedintheassessment of nutritionalstatusin adults,has beenalsousedinchildren.4,5Studieswithdifferent popula-tionshaveproposeddistributionsinpercentilesandcutoffs forWCinchildren,butthereisstillnoconsensusaboutthe criteriausedfortheassessmentofthisgroup.4
TheaccuracyoftheWCmeasurementwhencomparedto othermethodsofnutritionalstatusassessmentinchildren, suchasthebodymassindex(BMI)andthewaist/heightratio (WHtR),wasevaluatedinstudies ofwhich resultsshowed theuseofthismeasurein highblood pressurerisk identi-ficationin combination withBMIor asafactor associated withdyslipidemiaandhyperglycemia.6,7
Somefactorsassociatedwithexcessweightand abdomi-nalobesityinchildren,describedinthescientificliterature, are: the family’s socioeconomic status,8 parents’ nutri-tional status,9 and children’s sedentary behaviors.10 It is alsoknownthatunhealthyeatinghabitsandhighintakeof macronutrientsare possiblecauses of abdominalobesity.3 However,fewstudieshaveemployedtheWCtodetermine abdominalfatinBrazilianchildrenastheoutcomeof inter-est,andtoinvestigatethepossibleassociatedfactors.The aimofthisstudyistoassesstheassociationofdietaryand socioeconomic factors, sedentary behaviorsand maternal nutritionalstatus withabdominalobesity in childrenaged 3---10yearsinSantoscity,stateofSãoPaulo,Brazil.
Method
This study is part of the research project ‘‘Nutritional EnvironmentAssessmentinthecity ofSantos’’(AMBNUT), approvedbytheInstitutionalReviewBoardofUniversidade Federal deSão Paulo (Processes:275/2009 and276/2009) andfundedbyFundac¸ãodeAmparoaPesquisadoEstadode SãoPaulo(FAPESP)(processn.:2009/01361-0). Thiswasa cross-sectional,household-basedproject,carriedoutfrom JanuarytoDecember2010,whentwovisitsweremadeto thehouseholdstocollectsocioeconomicand anthropomet-ricdata,aswellasinformationonthefamilies’healthand foodhabits.
Estatística---IBGE),alsopublishedin 2010,the municipal-ityhad419,400residentsliving inanareaof281,000km2.
Theinsularportionofthemunicipalityisdividedintofour administrativeregions:Coast,Central,NorthwestandHills; theCoastalregionis characterizedbyhigherincome com-paredtotheothers.Itisestimatedthat55%offamilieslive intheCoastalregion,11%intheCentralregion,25%inthe Northwestand9%intheHills.
The AMBNUT project sample consisted of 538 families from 36 of the 566 census sectors in the insular part of the municipality, randomly selected proportionally to the population residing in three of the four regions: Central, Northwest and Coastal regions. The Hills region was not includedduetodifficultiesinaccessingtheplace.Thus,29 sectorswereassessedintheCoastalregion,threesectorsin theCentralregionandfoursectorsintheNorthwestregion, redistributingtheproportionofresidentsintheHills’regions totheotherregions.
Sample calculation considered a prevalence of excess weightinchildrenyoungerthanfiveyearsof7%inthe South-east region, measured by the National Demographic and HealthSurvey(PNDS),usingasignificancelevel of5% and 80%testpowerforatwo-tailedtest,withalossof10%.
Fordatacollection,sixinterviewers,bothgraduatedand undergraduatestudentsfromthehealtharea,weretrained toapplythequestionnaireandperformthefieldwork,and workedinpairs.Thetrainingwascarriedoutbytheresearch team responsible for the project, with a 40-h duration, whichincludedtraininginlaboratoryandsupervised moni-toringduringtheinitialfieldactivities.
The enrollmentofeach sectorwascarriedoutto iden-tifyeligiblehouseholds,havingasinclusioncriteriahomes that had at least one child younger than ten yearsliving withthebirthmother.Ifthemotherhadanydisorderthat could affect her nutritional status (cancer, AIDS or infec-tiousdiseases)orhadundergonebariatricsurgerythepair wasexcluded.Ifthehouseholdhadmorethanonechildin theagegroupbeingassessed,theparticipantwaschosenby drawinglots.Thedatacollectionprocedureswerecarried outonly afterthe children’smotherssigned theInformed ConsentForm.Theresponserateofassessedhouseholdsat enrollment was70%, andthemean durationofinterviews was100min.
A totalof357 pairsofmothers andchildrenwere con-sidered eligible for this specific study, corresponding to householdswithchildren agedthreeyearsoldor older,in whichtheWCmeasurewascollected.Thiscriterion main-tained the assessed sample representativeness, and the poweroftheassociationtestwas90%.
Children’s food intake was estimated using two 24-h recalls,ininterviewswiththemother,oneappliedateach visit. The nutritional composition of the food was calcu-latedusingtheAvanutri®programv.4.0(Avanutri&Nutric¸ão
Servic¸oseInformáticaLtda.,Três Rios,Brasil);thesystem databasewasexpandedusingdatafromtheBrazilianTable ofFoodComposition(TACO)andtheUnitedStates Depart-mentofAgriculture(USDA).
The median consumption of each macronutrient was
usedasacutoffpointfortheanalysis,takingintoaccount the children’s age (3 years, 4---8 years and 9---10 years) togeneratethe variable.This categorizationincludes the agegroupsfor whichtheInstituteofMedicine hasspecific
recommendationsforeachnutrientaccordingtotheDietary ReferenceIntake(DRI),inanattempttonotunderestimate oroverestimateconsumption.
Theweightandheightofmothersandchildrenwere col-lectedusingaTanita®portabledigitalscaleandAlturexata®
portablestadiometer,followingthestandardizedtechniques established by Lohman et al.11 Additionally, the moth-ers’tricipital,bicipital,suprailiacandsubscapularskinfolds werecollectedintriplicate,tocalculatethemeanvalueand estimatebodyfatpercentage.
WCwasmeasuredinduplicateusinga 150-cminelastic metrictape,withmeasurementbeingstandardized atthe midpointbetweenthelastribandtheiliaccrest,withthe childorthemotherinthestandingposition,withoutclothes coveringtheabdominalregion;thereadingwasperformed atexpiration.
TheproposalbyTayloretal.wasusedtoevaluate chil-dren’sabdominalfat,whichconsidersvaluesabovethe80th percentile (p80) as abdominal obesity.12 As for BMI, the WorldHealthOrganization(WHO)curveswereusedto iden-tifyexcessweight.13
Toclassifymaternalnutritionalstatus,BMIandWCwere usedaccordingtotheWHOrecommendations,whichdepict BMI≥25kg/m2asexcessweightandWC≥80cmasabdominal obesity.14Bodyfatclassificationwasconsideredwhenvalues were≥32%,indicatingelevatedbodyfat.11
Thechildren’ssedentarybehaviorswereassessedbased on the time spent watching TV, using the computer and walking,aswellasbicycleridingasamaintransportmode for daily activities or as leisure activities, according to the YOUTH validated questionnaire of the Study Center of the Physical Fitness Laboratory of São Caetano do Sul (CELAFICS).15 The analysis used a cutoff of 2h of watch-ing TV daily, as recommended by the American Academy ofPediatrics16;thesamecriterionwasappliedtocomputer screentimeuse.
The socioeconomic assessment of families wascarried outusingthe IBGEandPNDSquestionnaires,which assess characteristics of households, schooling and income. For thestratification offamilies,theBrazilian Economic Clas-sificationCriteriawere used,asproposedby theBrazilian AssociationofResearchCompanies(ABEP).17 Forthe anal-yses, classes were grouped into A+B (high socioeconomic status)andC+D+E(lowsocioeconomicstatus).
Descriptive statistical analysis of the sample was per-formed,stratifiedbythechildren’sagegroup.Associations between the variables of interest and abdominal obesity were verified using multiple logistic regression models, withWC>p80beingtheoutcome,andsocioeconomic varia-bles,maternalnutritionalstatusandthe child’sindividual variables being used to adjust the model. Initially, the chi-square test was used for the univariate analysis and variables with p<0.20 were included in the multivariate analysis.Inthefinalmodel,onlythevariableswithp-value <0.05remained. The Hosmer---Lemeshowtest wasused to verify the goodness-of-fit. These results are shown with thevaluesof oddsratio(OR) and95% confidenceinterval (95%CI).
StatisticalPackagefortheSocialSciences® (SPSS)software v.16(SPSSInc.,Chicago,IL,USA).
Results
Tables1and2disclosethedescriptivesampledata accord-ingto theprevalence of assessed factors. Overall, it was observed that 30.5% of children and 64% of mothers had abdominalobesity.TheunivariateanalysisshowninTable3 indicatedanassociationbetweenhavingabdominalobesity andexcessweightaccordingtoBMI/age.Therewereno sig-nificantassociationswiththeconsumptionofnutrientsfor carbohydrates,lipidsandprotein;however,proteinintake wassubsequentlytestedintheregressionmodel(p=0.085). Noneofthevariablesrelatedtosedentarybehaviorshowed anassociationwiththeoutcome(p>0.20).Significant
asso-ciations were observed between the variables of social stratification according to ABEP,car ownership, maternal workoutsidethehome,maternalexcessweight,and mater-naltotalandcentralobesity(Table3).
Table 4 shows the results of the final logistic regres-sion model. In the final model, the association between thechild’sabdominalobesityandchildhoodexcessweight according to BMI/age, female gender and the mothers’ abdominalobesityweresignificant.TheABEPsocioeconomic classificationvariableremainedasacontrolvariable.
Discussion
This study identified associations between the abdominal obesityinchildrenandthechild’snutritionalstatus(excess weightaccordingtoBMI/age),thechild’sgender (female) andthemother’snutritionalstatus(abdominalobesity).
Table1 Prevalenceofthesample’sindividualvariables,accordingtothechildren’sagegroup.Santos,2012(n=357).
3---4years 5---7years 8---10years Total
n % n % n % n %
Children’scharacteristics
Gender
Male 50 58.8 68 52.7 75 52.4 193 54.1
Female 35 41.2 61 47.3 68 47.6 164 45.9
Abdominalobesity
Yes 32 37.6 28 21.7 49 34.3 109 30.5
No 53 62.4 101 78.3 94 65.7 248 69.5
ExcessweightaccordingtoBMI/age
Yes 12 14.1 39 30.2 62 43.4 113 31.7
No 73 85.9 90 69.8 81 56.6 244 68.3
TimespentwatchingTV
High 73 85.9 108 83.7 116 81.1 297 83.2
Adequate 12 14.1 21 16.3 27 18.9 60 16.8
Timespentusingcomputer
High 6 7.1 28 21.7 41 28.7 75 21.0
Adequate 79 92.9 101 78.3 102 71.3 282 79.0
Walkingasthemaintransportmode
Yes 48 56.5 84 65.1 91 63.6 223 62.5
No 37 43.5 45 34.9 52 36.4 134 37.5
Bicycleasthemaintransportmode
Yes 4 4.7 11 8.5 12 8.4 27 7.6
No 81 95.3 118 91.5 131 91.6 330 92.4
Carbohydrateconsumptiona
Higherthan/sameasmedian 38 46.3 42 33.4 41 28.8 121 34.5
Belowmedian 44 53.7 84 66.6 101 71.2 229 65.5
Proteinconsumptiona
Higherthan/sameasmedian 44 53.6 57 45.2 72 50.7 173 49.4
Belowmedian 38 46.4 69 54.8 70 49.3 177 50.6
Lipidconsumptiona
Higherthan/sameasmedian 49 59.7 54 42.8 67 47.1 170 48.5
Belowmedian 33 40.3 72 57.2 75 52.9 180 51.5
BMI,bodymassindex.
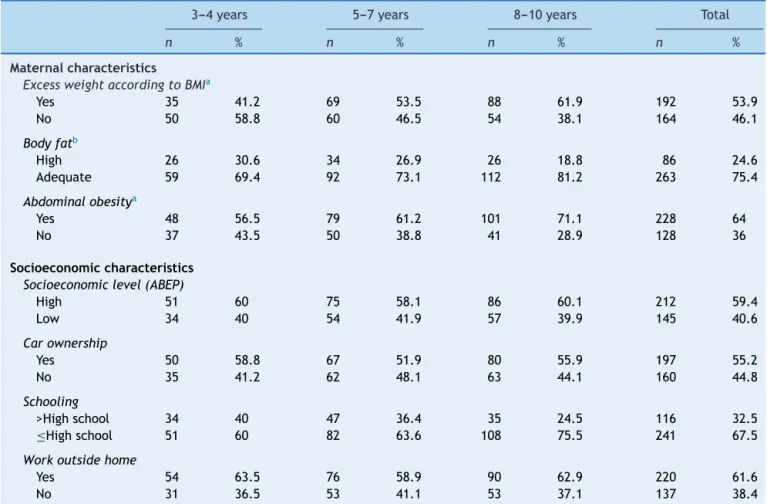
Table2 Prevalenceofmaternalandsocioeconomicvariablesofthesample,accordingtothechildren’s agegroup.Santos, 2012(n=357).
3---4years 5---7years 8---10years Total
n % n % n % n %
Maternalcharacteristics
ExcessweightaccordingtoBMIa
Yes 35 41.2 69 53.5 88 61.9 192 53.9
No 50 58.8 60 46.5 54 38.1 164 46.1
Bodyfatb
High 26 30.6 34 26.9 26 18.8 86 24.6
Adequate 59 69.4 92 73.1 112 81.2 263 75.4
Abdominalobesitya
Yes 48 56.5 79 61.2 101 71.1 228 64
No 37 43.5 50 38.8 41 28.9 128 36
Socioeconomiccharacteristics
Socioeconomiclevel(ABEP)
High 51 60 75 58.1 86 60.1 212 59.4
Low 34 40 54 41.9 57 39.9 145 40.6
Carownership
Yes 50 58.8 67 51.9 80 55.9 197 55.2
No 35 41.2 62 48.1 63 44.1 160 44.8
Schooling
>Highschool 34 40 47 36.4 35 24.5 116 32.5
≤Highschool 51 60 82 63.6 108 75.5 241 67.5
Workoutsidehome
Yes 54 63.5 76 58.9 90 62.9 220 61.6
No 31 36.5 53 41.1 53 37.1 137 38.4
BMI,bodymassindex;ABEP,BrazilianAssociationofResearchCompanies(Associac¸ãoBrasileiradeEmpresasdePesquisa).
a n =356. b n
=349.
The results showed a prevalence of 30.5% of children withabdominalobesity.AstudywithBrazilianchildrenaged 7---10yearsfoundaprevalenceof22%forgirlsand26.5%for boys,slightlylowervalues,butestimatedbasedonanother reference.18Anotherstudyidentifiedaprevalenceof33.7% ofexcessweightinchildrenfromSantoscity,19valuesthat areconsistentwiththedatainthisresearch.Thisscenario shows thatexcessweightandchild abdominalobesity are bothprevalent.
Attheunivariateanalysis,child’sriskfor overweightor overweightwasassociatedwiththepresenceofabdominal obesity.Thisfindingisconsistentwiththefactthatthetrunk regionisonewithincreasedsusceptibilitytofat accumula-tion.Althoughthisvariableremainedinthefinalregression model,itisrelevanttoconsideritseffect’soverestimation, giventhemarkedassociationbetweenexcessweightandthe assessedoutcome;itisalsoimportanttoconsiderthebroad CI(OR=93.7,95%CI:39.3---223.3).12,20AstudywithBrazilian adolescentsproducedsimilarresults,whenconsideringthat individualswithahigheramountofsubcutaneousfatwere 133.6 times more likelyto have abdominalobesity21; the authorsusedtheclassificationbyTayloretal.,12 alsoused inthepresentstudy.
Theresultsalsoshowthatgirlsare4.1timesmorelikely to have abdominal obesity; one expects to find greater
adiposity in females, taking into consideration the BMI22; however,anassociationhasbeenshownbetweenadiposity, BMIandWCinmalechildrenandadolescents.21,23Itisalso knownthattheadultmalehasmorevisceralfat accumula-tionthan adultwomen24;thus, itisworth consideringthe hypothesisthatmostabdominalfatfoundingirlscanbea characteristicofthissample;i.e.,itispossiblethatthe typ-icalconditionsofbodyfataccumulationaremoreevident onlyafterpuberty,whenconsideringthatthesample’sage rangemaybetooyoung.
Activitiesconsidered assedentary practicesshowed no associationwithabdominalobesity,whichcontradicts pre-viousfindingsontheeffectoftimespentwatchingTVand activetransporttoschool.10,22,23AstudywithBrazilian ado-lescentsalsofound adifferentresult:an insufficientlevel ofphysicalactivitywasassociatedwithanelevatedWC.25It ispossiblethatthestudyvariableswerenotgoodmarkers ofsedentarybehaviors,whichmaybringhealthriskstothis population.However,itshouldbeconsideredthatthetime spentwatchingTVandusingthecomputerwasreportedby thechild’smotherandmayhavebeenunderestimated.
Table3 Univariateanalysis ofexploratoryvariables and association with the children’s abdominal obesity as the dependentvariable.Santos,2012(n=357).
crudeOR 95%CI p-value
Children’scharacteristics
Gender
Male 1.0 --- 0.172
Female 1.4 0.8---2.2
ExcessweightaccordingtoBMI/age
Yes 62.4 30.1---129.2 <0.001
No 1.0
---Proteinconsumption
Higherthan/sameas median
1.0 --- 0.085
Belowmedian 0.6 0.4---1.0
Maternalcharacteristicsandsocioeconomiclevel
Socioeconomiclevel(ABEP)
High 1.0 --- 0.017
Low 0.6 0.3---0.9
Carownership
Yes 1.8 1.1---2.8 0.012
No 1.0
---Schooling
>Highschool 1.0 --- 0.171
≤Highschool 0.7 0.4---1.1
Workoutsidehome
Yes 1.9 1.1---3.0 0.010
No 1.0
---Excessweight(BMI)a
Yes 1.7 1.0---2.7 0.024
No 1.0
---Bodyfatb
High 1.9 1.0---3.3 0.033
Adequate 1.0
---Abdominalobesitya
Yes 2.2 1.3---3.6 0.002
No 1.0
---BMI,bodymassindex;ABEP,BrazilianAssociationofResearch Companies(Associac¸ãoBrasileiradeEmpresasdePesquisa);OR, oddsratio;CI,confidenceinterval.
an =356. b n
=349.
changesinthediet,moreproteingeneratedareductionof 2.7cmin WCof children and adolescentsin relation toa groupwithlowproteinintake,inalongitudinalstudy.26
Maternal nutritional status was significantly associ-ated with abdominal obesity in children in all assessed parameters, especially with the WC measurement in the multivariateanalysis.Inoursample,amotherwith abdom-inalobesityincreasesby2.7-foldthechanceofherchildren alsodeveloping thiscondition.Studies carriedoutin Mex-icoreportthatchildrenofparentswithabdominalobesity are2.85times morelikelytohavethesamecondition,9a valuesimilartothatfoundinourstudy.Otherstudiesalso
Table4 Multiplelogisticregressionmodelwith the chil-dren’sabdominalobesityasthedependentvariable.Santos, 2012(n=356).
AdjustedOR 95%CI p-value
Excessweightaccordingtothechild’sBMI/age
Yes 93.7 39.3---223.3 <0.001
No 1.0
---Child’sgender
Male 1.0 --- 0.012
Female 4.1 1.8---9.3
Maternalabdominalobesity
Yes 2.7 1.2---6.0 0.01
No 1.0
---SocioeconomiclevelaccordingtoABEP
High 1.0 --- 0.08
Low 0.5 0.2---1.0
BMI,bodymassindex; ABEP,BrazilianAssociationofResearch Companies(Associac¸ãoBrasileiradeEmpresasdePesquisa);OR, oddsratio;CI,confidenceinterval.
foundanassociationbetweenexcessweightinchildrenand maternalobesity.22,23Thisindicatesthatthenutritional sta-tus of both thechild’s motherandfather may berelated to this outcome, and it should be considered that such influencecouldbeassociatedwithbothgeneticand socio-culturalfactorsof familyhabits. The nutritionalattention care in maternal and child health thus should begin dur-ing the prenatal period and encompass the whole family structure. Ithasbeen shownthatparentalinvolvement in nutritionaleducationinterventionsandin promoting phys-icalactivityforchildrenbeneficiallyassistinreducingBMI andothernutritionalstatusparameters,27 anditshouldbe previouslyconsideredthattheparents’perceptionoftheir child’snutritionalstatuscanbeanobstacle,giventhe diffi-cultyinidentifyingoverweightand,therefore,recognizing theimportanceofincludingtheirchildinsuchactivities.28
Eventhoughithadnosignificanceinthefinalmodel,the univariateanalysisshowedasignificantassociationbetween abdominalobesityinchildrenandsocioeconomicstatusby social stratification, car ownership and the fact that the motherworked outof the household.Highsocioeconomic level, represented by the type of school and town/city, hasalsobeen associatedwithabdominalobesity inIndian children.8 However,another study withBrazilian children younger than five years did not observe an association between socioeconomic status, also represented by the ABEP,andexcessweight29;it canbesuggested thatother factorshavea greaterinfluenceonnutritionalstatusthan socioeconomiclevel.
optionstofeedthem,habitsthatcanbelaterincorporated bythechildren.
The study of food intake has limitations, such as the small number of 24-h recalls and obtaining data through interviewswiththemother,whichcanresultin underreport-ing.Additionally,consideringthisstudyappliedanextensive investigation questionnaire, somequestions andmeasures couldnotbeappliedormeasured bytheinterviewersdue toallegeddiscomfortorrefusalonthepartofthe respon-dentand,thus,therearesomevariableswithmissingvalues. Theresponserateof70%mayalsohaveaffectedtheresults ofsomeassociations.Moreover,consideringthisisa cross-sectionalstudy,onecannotestablishacausalityassociation betweentheanalyzedfactors.Inspiteoftheselimitations, thecontributionsofthisstudyincludetheobservationthat maternalnutritionalstatus,theoccurrenceofexcessweight andfemalegenderareassociatedwithabdominalobesityin children,regardlessoftheirsocioeconomicstatus.
Metabolicsyndromeinchildrenisstillanemergingtopic, for which differentclinical aspectsare considered in the diagnosis, depending onthe theoretical reference.30 Ele-vatedWCis oneoftheseaspects and,whencomparedto others, such asserum levels of glucose andlipids, it has advantagesforbeinganoninvasive,easytomeasure proce-dure.Thus,itsinclusioninroutineprimarycarewouldhelp toplaninterventionsandinterdisciplinaryactivities associ-atedwiththefightagainstchronicdiseasesinchildhood.
Theassociationsinvolvingthechild’sWCarestill uncer-tain. More studies in this line of research are needed to validate some of the assumptions made herein. It is expectedthatthisstudywillcontributetothedevelopment of public policies for the prevention of chronic diseases, consideringtheimportanceofnutritionaleducationactions directedat the family environment,aiming toresult in a greaterimpactonthenutritionalstatusofchildren.
Funding
Fundac¸ãodeAmparoaPesquisadeSãoPaulo---FAPESP (pro-cessesnumbers2009/01361-1and2011/21270-0).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
ToFAPESPforfundingthisstudytothefamiliesthat partic-ipatedinthestudyandtheAMBNUTprojectteam.
References
1.GuptaN,GoelK,ShahP,MisraA.Childhoodobesityin devel-opingcountries:epidemiology, determinants andprevention. EndocrRev.2012;33:48---70.
2.Flores LS, Gaya AR, Petersen RD, Gaya A. Tendência do baixopeso,sobrepesoeobesidadedecrianc¸aseadolescentes brasileiros.JPediatr(RioJ).2013;89:456---61.
3.SuligaE.Visceraladiposetissueinchildrenandadolescents:a review.NutrResRev.2009;22:137---47.
4.MagalhãesEI,Sant’AnaLF,PrioreSE,FranceschiniSC.Perímetro dacintura, relac¸ãocintura/estaturaeperímetro dopescoc¸o como parâmetros na avaliac¸ão da obesidade central em crianc¸as.RevPaulPediatr.2014;32:273---82.
5.DaigreJL,AtallahA,BoissinJL,etal.Theprevalenceof over-weight andobesity, and distribution ofwaistcircumference, inadultsandchildrenintheFrenchOverseasTerritories:the PODIUMsurvey.DiabetesMetab.2012;38:404---11.
6.ZhangYX,WangSR.Comparisonofbloodpressurelevelsamong childrenandadolescentswithdifferentbodymassindexand waist circumference: study in a large sample in Shandong, China.EurJNutr.2014;53:627---34.
7.RosiniN,MachadoMJ,WebsterIZ,MouraSA, CavalcanteLS, daSilvaEL.Simultaneouspredictionofhyperglycemiaand dys-lipidemia in school children in Santa Catarina State, Brazil based on waist circumference measurement. Clin Biochem. 2013;46:1837---41.
8.MisraA,ShahP,GoelK,etal.Thehighburdenofobesityand abdominalobesityinurbanIndianschoolchildren:a multicen-tricstudyof38,296children.AnnNutrMetab.2011;58:203---11.
9.Jiménez-CruzA,WojcickiJM,Bacardí-GascónM,etal.Maternal BMIandmigrationstatusaspredictorsofchildhoodobesityin Mexico.NutrHosp.2011;26:187---93.
10.LubansDR,BorehamCA,KellyP,FosterCE. Therelationship betweenactivetraveltoschoolandhealth-related fitnessin childrenandadolescents:asystematicreview.IntJBehavNutr PhysAct.2011;8:5.
11.LohmanTG,RocheAF,MartorellR.Anthropometric standard-izationreferencemanual.Champaign:HumanKineticsBooks; 1991.
12.Taylor RW, JonesIE, Williams SM,Goulding A. Evaluationof waistcircumference,waist-to-hipratio,andtheconicityindex asscreeningtoolsforhightrunkfatmass,asmeasuredby dual-energyX-rayabsorptiometry,inchildrenaged3---19y.AmJClin Nutr.2000;72:490---5.
13.deOnisM,OnyangoAW,BorghiE,SiyamA,NishidaC,Siekmann J.DevelopmentofaWHOgrowthreferenceforschool-aged chil-drenandadolescents.BullWorldHealthOrgan.2007;85:660---7.
14.World Health Organization [homepage on the Internet], Report of a WHO consultation on obesity Obesity: pre-venting and managing the global epidemic; 1998. Available from http://whqlibdoc.who.int/hq/1998/WHONUTNCD98.1
(p1-158).pdf[accessed17.07.14].
15.YouthRB.Questionáriodeatividadefísica:crianc¸ase adoles-centes.SãoCaetanodoSul:CELAFISCS;2005.
16.AmericanAcademyofPediatrics,CommitteeonPublic Educa-tion,AmericanAcademyofPediatrics.Children,adolescents, andtelevision.Pediatrics.2001;07:423---6.
17.Associac¸ão Brasileira de Empresas de Pesquisa [home-page on the Internet]. Critério de classificac¸ão econômica Brasil; 2008. Available from http://www.abep.org/novo/ Content.aspx?ContentID=302[accessed17.07.14].
18.deAssisMA,Rolland-CacheraMF,deVasconcelosFA,etal. Cen-traladiposityinBrazilianschoolchildrenaged7---10years.BrJ Nutr.2007;97:799---805.
19.da Costa RF, Cintra IP, Fisberg M. Prevalênciade sobrepeso eobesidade emescolaresda cidade deSantos, SP. Arq Bras EndocrinolMetab.2006;50:60---7.
20.EbbertJO,JensenMD.Fatdepots,freefattyacids,and dysli-pidemia.Nutrients.2013;5:498---508.
21.Silva DA, Pelegrini A, da Silva AF, Grigollo LR, Petroski EL. Obesidade abdominale fatoresassociados em adolescentes: comparac¸ãodeduasregiõesbrasileirasdiferentes economica-mente.ArqBrasEndocrinolMetab.2012;56:291---9.
Jordan:prevalenceandassociatedfactors.MaternChildHealth J.2009;13:424---31.
23.NovaesJF,LamounierJA,FranceschiniSC,PrioreSE.Fatores ambientais associados ao sobrepeso infantil. Rev Nutr. 2009;22:661---73.
24.KukJL,LeeS,HeymsfieldSB,RossR.Waistcircumferenceand abdominaladiposetissuedistribution:influenceofageandsex. AmJClinNutr.2005;81:1330---4.
25.GuilhermeFR,Molena-FernandesCA,GuilhermeVR,FáveroMT, ReisEJ,RinaldiW.Inatividadefísicaemedidas antropométri-casemescolaresdeParanavaí,Paraná,Brasil.RevPaulPediatr. 2015;33(1):50---5.
26.Damsgaard CT, PapadakiA, JensenSM,etal. Higherprotein dietsconsumed adlibitumimprove cardiovascularrisk mark-ers in children of overweight parents from eight European countries.JNutr.2013;143:810---7.
27.Niemeier BS, Hektner JM, Enger KB. Parent participation inweight-related healthinterventions for children and ado-lescents: a systematic review and meta-analysis. Prev Med. 2012;55:3---13.
28.FrancescattoC,SantosNS,CoutinhoVF,CostaRF. Percepc¸ão demãessobreoestadonutricionaldeseusfilhoscomexcesso de peso: revisão sistemática. J Pediatr (Rio J). 2014;90: 332---43.
29.dasChagas DC,da SilvaAA, Batista RF, etal. Prevalênciae fatores associados à desnutric¸ão e ao excesso de peso em menoresdecincoanosnosseismaioresmunicípiosdoMaranhão. RevBrasEpidemiol.2013;6:146---56.