www.jped.com.br
ORIGINAL
ARTICLE
Prevalence
of
enuresis
and
urinary
symptoms
at
age
7
years
in
the
2004
birth
cohort
from
Pelotas,
Brazil
夽
Denise
M.
Mota
a,∗,
Aluisio
J.D.
Barros
a,
Alicia
Matijasevich
a,b,
Iná
S.
Santos
aaUniversidadeFederaldePelotas(UFPEL),Pelotas,RS,Brazil
bDepartmentofPreventiveMedicine,FaculdadedeMedicina,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
Received28January2014;accepted22April2014 Availableonline3September2014
KEYWORDS
Enuresis;
Urinarysymptoms; Children;
Prevalence
Abstract
Objective: Todeterminetheprevalenceofenuresis,urinary,andbowelsymptomsand
associ-atedfactorsinchildrenaged7yearsinabirthcohort.
Methods: Apre-codedquestionnairewasapplied to3,602children whobelongedto abirth
cohortinitiatedin2004inPelotas,Brazil.Duringhomevisitsat12,24,and48monthsandat
age7years,mothersansweredaquestionnairewithdemographicquestionsandcharacteristics
ofbladderandbowelhabitsofchildrenusingaurinarysymptomscore.Poissonregressionwas
usedforthehierarchicalmultivariableanalysis,withrobustvariance.
Results: Theprevalenceofenuresiswas10.6%;11.7%inmalesand9.3%infemales;enuresis
wasmonosymptomaticin9.8%ofthechildren(10.8%ofmalesand8.3%offemales);37.4%had
symptomsuptoonceaweek;32.9%,twotofourtimesaweek;and26.2%,everyday,withno
differencebetweengenders.Themostcommonurinarysymptomswereurinaryurgency(22.7%)
andurinaryretentionmaneuvers(38.2%).Inthemultivariateanalysis,itwasobservedthatthe
numberofurinarysymptomsandthenumberofchildrenathomeshowedadirectassociation
withthepresenceofenuresis,whereasmaternaleducationwasinverselyassociated.
Conclusions: Enuresisisaprevalentconditionandshouldbeinvestigatedinclinicalpractice,
especiallyinchildrenoflowersocioeconomicstatus.Adetailedhistoryofurinaryhabitsdetects
associated urinarysymptoms,which isimportantfor adequateclassification ofenuresisand
subsequentmanagement.
©2014SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:MotaDM,BarrosAJ,MatijasevichA,SantosIS.Prevalenceofenuresisandurinarysymptomsatage7yearsin the2004birthcohortfromPelotas,Brazil.JPediatr(RioJ).2015;91:52---8.
∗Correspondingauthor.
E-mail:[email protected](D.M.Mota). http://dx.doi.org/10.1016/j.jped.2014.04.011
PALAVRAS-CHAVE
Enurese;
Sintomasmiccionais; Crianc¸as;
Prevalência
Prevalênciadeenureseesintomasmiccionaisaosseteanosnacoortede nascimentosde2004,Pelotas,Brasil
Resumo
Objetivo: Determinaraprevalênciadeenurese,sintomasurinárioseintestinaisefatores
asso-ciadosemcrianc¸asdeseteanos,emumacoortedenascimentos.
Métodos: Foiaplicadoumquestionáriopré-codificadoem3.602crianc¸aspertencentesàcoorte
denascimentosiniciadaem2004,emPelotas,RS.Emvisitasdomiciliaresrealizadasaos12,24
e48meseseaosseteanos,asmãesresponderamumquestionáriocomquestões
sociodemográ-ficas esobreascaracterísticasehábitosmiccionaiseintestinaisdascrianc¸as,utilizandoum
escoredesintomasmiccionais.Paraaanálisemultivariávelhierarquizada,utilizou-seregressão
dePoissoncomvariânciarobusta.
Resultados: Aprevalênciadeenuresedefoi10,6%,sendo11,7%nosmeninose9,3%nas
meni-nas; aenurese foi monossintomáticaem 9,8%das crianc¸as (10,8%dos meninos e 8,3%das
meninas);37,4%apresentavamosintomaatéumavezporsemana;32,9%,duasaquetrovezes
porsemana;e26,2%todososdias,semdiferenc¸aentreossexos.Ossintomasurináriosmais
fre-quentesforamurgênciamiccional(22,7%)emanobrasdecontenc¸ãourinária(38,2%).Naanálise
multivariável,observou-sequeonúmerodesintomasmiccionaiseonúmerodecrianc¸asem
casamostraramrelac¸ãodiretacompresenc¸adeenurese,enquantoqueaescolaridadematerna
apresentourelac¸ãoinversa.
Conclusões: A enurese éuma patologia prevalente edeve ser investigada em consultasde
rotina,especialmenteemcrianc¸ascommenornívelsocioeconômico.Umahistóriadetalhada
sobrehábitosurináriospodedetectarsintomasmiccionaisassociados,importantesparauma
adequadaclassificac¸ãodaenureseeposteriormanejo.
©2014SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos
reservados.
Introduction
Enuresis is the involuntary loss of urine at night, in the absence of organic disease, at an age when it would be expected for the child to control urination (usually after 5 years).1 Itsnatural history suggestssymptom regression up to adolescence and adulthood, with annual remission rates around15%.Still, enuresis affectsmanyfamilies,as itcancausesocialandemotionalstigma,stress,and incon-venienceforchildrenandparents.
Theprevalenceofenuresisvarieswithage.Studies con-ductedwith7-year-oldchildren havereportedprevalence ratesof7%to10%,consideringbothchildrenthatwetthe bed once a month and those who do it every night.2---4 Enuresis is classified as primary (symptoms were always present)orsecondary(atleastsixmonthswithout bedwet-tingandreturnofsymptoms).5Primaryenuresisappearsto resultfromnocturnalpolyuriaordecreasedbladder capac-ity, together with the incapacity of child to wake up in responsetobladderfullness.2,3,5
Regardingthepresenceofotherurinarysymptoms,itis classifiedasmonosymptomaticenuresis(ME),whentheonly symptom is enuresis, and non-monosymptomatic enuresis (NME),withthepresenceofotherurinarysymptoms(urinary urgency,urinaryincontinence,urinaryretentionmaneuvers, and increased number of daily micturitions).6 The preva-lenceofNMEenuresisisnotwellknowninpopulation-based samples, withestimates ranging from 20% to80% of chil-drenwithenuresis.6Acarefulhistoryisrequiredtodetect
thesesymptoms.Theclassificationofenuresismodifiesthe therapeuticapproachand,consequently,itsprognosis.
Thestudiesgenerallyinvestigatesamplesof schoolchil-dren and users of outpatient services, with scarce population-based and cohort researches, especially with Brazilianchildren.
Theaim ofthisstudywastodetermine theprevalence of enuresis, urinary and bowel symptoms,and associated factors in children aged 7 years belonging to the Pelotas birthcohortof2004.
Methods
TheInternationalClassificationofDiseases(ICD)version 10 defines enuresis as bedwetting at least once a month forthreemonths,inchildrenagedfiveyearsorolder.9The AmericanPsychiatric Association defines enuresis as bed-wettingatleasttwiceamonth,forthreemonths.10Forthis analysis,enuresis was defined asbedwetting at night, at leastonceamonth,inthelastthreemonths.
Toevaluateotherurinarysymptoms,thecriteriadefined by theInternational ContinenceSociety11 wereused: uri-naryincontinence(involuntarylossofsmallamountsofurine duringtheday, atleastonceeverytwoweeks,inchildren withsphincter controlor, after3 yearsofage); increased urinaryfrequency(urinatingmorethaneighttimesaday); decreasedurinaryfrequency(urinatinglessthanthreetimes aday);urinaryretentionmaneuvers(child’seffortsto sup-presstheurgencyassociatedwithurination,suchascrossing the legs, sit on the heels, squeeze the penis); urinary urgency(urgentneedtourinate);anddysuria(painduring urination).
Constipation wasdefined as the report of difficulty in evacuating, interval between bowel movements greater than72hours,painondefecation,orhardorlumpystools.12 Encopresiswasdefinedasthereportoffecalescapeinthe last three months. Both urinary and intestinal symptoms wereevaluatedregardingfrequency: never,sometimes (1-14daysinthemonth),almostalways(15to29daysinthe month),andalways(everyday).
The history of urinary tract infection was assessed throughfamilyreportateachvisitmadetothecohort: uri-narytractinfectionbefore1year;between1and2years; between2and4years;between4and6years;andatany ageupto6years.
Ascoreofeliminationdysfunctionwascreated, consist-ingof the number of urinarysymptoms, except enuresis, presented by the child at 7 years of age: urinary incon-tinence,urinarymaneuvers,urinary urgency,increasedor decreasedurination, andencopresis andintervalbetween evacuations>72hours.Thescorecouldrangefrom0to6 (sumofsymptoms).
Theothervariablesincludedintheanalysiswere:gender ofthechild,lowbirthweight(<2,500g),prematurity (gesta-tionalage<37weeks),numberofchildreninthehousehold inadditiontotheindexchild(informationcollectedatthe visitof48months);maternalcharacteristics:schoolingand age(inyears),ethnicity(white,blackormixed-race),parity, maternalpaidwork,andfamilysocioeconomiclevel accord-ingtotheNationalEconomicIndicator(IndicadorEconômico Nacional-IEN), inreferencequintilesforPelotas,13 based oninformationcollectedduringthe48months.
The interviewerswerespeciallytrainedtoperformthe interviews.Qualitycontrol,inordertopreventanddetect fraudintheinterviews,includedtherepetitionof10%ofthe interviewsathome(usingareducedquestionnaire),aswell astelephonecontactwithmotherswhohadafixedormobile telephone(forconfirmationofperformanceandsatisfaction withtheinterview).
The analysis was performed using the Stata 11 (Stata Corp., College Station, TX, United States) software. Chi-squaredtestswereusedtocompareprevalence,according tocategoricalexposures,andlineartrendtestswereused for ordinal exposures. For the hierarchical multivariable analysis,Poissonregressionwithrobustvariancewasused,
Table1 Descriptionofthegeneralsampleandofchildren
withenuresis.
Variable Totaln(%) Enuresis10.6%
Gender p=0.019
Male 1,872(52.0) 11.7
Female 1,729(48.0) 9.3
Prematurity p=0.040
Yes 496(13.8) 13.2
No 3,101(86.2) 10.2
Birthweight p=0.006
<2,500grams 282(7.8) 15.4
≥2500grams 3,318(92.2) 10.2
Maternalage(years) p=0.011
Adolescent(upto
19)
645(18.7) 13.0
20-29 1,702(49.2) 10.8
30-39 995(28.8) 8.0
>40 117(3.4) 11.1
Maternalschooling (years)
p<0.001
0-4 510(14.9) 13.2
5-8 1,418(41.4) 11.9
9-11 1,157(33.8) 8.2
>12 343(10.0) 6.8
Referencequintiles forsocioeconomic level(IEN)
p=0.003
1(poorer)(at4
years)
772(22.6) 13.7
2 713(20.9) 10.5
3 772(22.6) 10.8
4 566(16.6) 8.0
5(wealthier) 596(17.4) 8.1
Maternalethnicity p=0.002
White 2,049(62.3) 8.8
Black 548(16.7) 13.7
Mixed-race 690(21.0) 11.3
Numberofchildren athome(at4 years)
p<0.001
None 1,315(38.3) 8.6
One 378(11.0) 13.5
Two 1,427(41.6) 9.9
Threeormore 314(9.1) 16.6
IEN,IndicadorEconômicoNacional.
separatelyforthedifferencesfoundintheliteratureonthe prevalenceofenuresisbetweengenders.
ThestudyprotocolwasapprovedbytheEthics Commit-teeof theSchoolofMedicine oftheUniversidadeFederal dePelotas.Writtenconsenttoparticipateinthestudywas requestedfromallmothers,aftertheywereinformedabout thestudyobjectives,andconfidentialityofinformationwas guaranteed.
Results
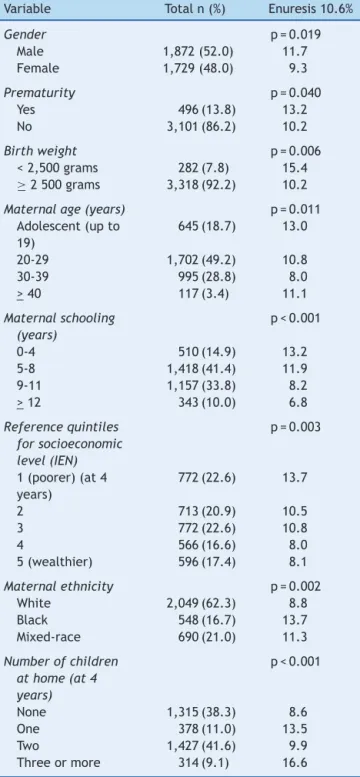
Dataon3,602 children agedbetween 6and 7years were used for this analysis. Table 1 describes the overall sam-pleandtheprevalenceofenuresisaccording tomaternal,
socioeconomic,anddemographicvariables.52%ofthe chil-drenweremales.Themeanagewas6.8yearsand43.5%of familieswereclassifiedinthetwolowerincomequintiles. The prevalence of enuresis was 10.6%, with a predomi-nanceofmales(p=0.019).Theprevalenceofenuresiswas inverselyassociatedwithsocioeconomicstatus(p=0.003). Enuresiswasmorecommonamongchildrenwithlowbirth weight,prematurechildren,children of adolescent moth-ers,lowerdegreeofmaternalschooling,blackethnicity,and livinginhouseholdswiththreeormorechildren.
Table2showstheprevalenceofurinaryandbowel symp-tomsamongchildrenintheoverallsampleandstratifiedby gender.Themostprevalentsymptomswereurinaryurgency (22.7% of the children had symptoms almost always or always)andurinaryretentionmaneuvers(occurringin38.2%
Table2 Prevalenceofurinaryandbowelsymptomsinchildrenwithandwithoutenuresisfromthe2004cohortat7yearsof
agestratifiedbygender.
Variable General Male General Female
Enuresis 11.8
Noenuresis
88.2
p-value Enuresis
9.3
Noenuresis
90.7
p-value
Urinaryincontinence <0.001 <0.001
Never 89.7 66.1 92.9 87.8 57.5 90.9
Sometimes 8.5 21.6 6.8 10.0 26.9 6.8
Almostalways 0.8 4.6 0.2 1.3 7.5 0.2
Always 1.0 7.8 0.1 0.9 8.1 0.1
Inadequatenumber
ofmicturitions
(<threeor>
eight/day)
10.2 13.2 9.8 0.137 8.6 17.6 7.7 <0.001
Retentionmaneuvers <0.001 <0.001
Never 67.2 60.5 68.0 52.6 43.4 53.5
Sometimes 24.8 25.1 24.7 33.4 35.2 33.3
Almostalways 5.6 8.4 5.3 9.3 10.1 9.2
Always 2.4 6.1 2.0 4.7 11.3 4.1
Urinaryurgency 0.002 <0.001
Never 26.2 22.2 26.7 24.6 16.5 25.4
Sometimes 51.7 45.4 52.6 51.0 46.8 51.1
Almostalways 13.1 19.0 12.3 14.4 16.5 14.2
Always 9.0 13.4 8.4 10.3 20.3 9.3
Encopresis <0.001 <0.001
Never 95.8 89.9 96.6 98.7 91.3 99.5
Sometimes 2.8 4.1 2.6 0.8 4.4 0.4
Almostalways 0.6 0.9 0.6 0.4 0.6 0.1
Never 0.8 5.1 0.2 0.6 3.8 0.0
Intervals>72hsto
evacuate
8.9 11.5 8.6 0.165 9.1 8.2 9.1 0.720
Urinarysymptom
scorea
<0.001 <0.001
Nosymptoms 17.2 10.8 19.1 16.0 8.3 16.8
Onesymptom 35.3 27.1 39.9 32.0 21.4 33.0
Twosymptoms 33.5 35.5 30.5 36.2 35.2 36.3
Threesymptoms 11.2 20.7 8.1 13.2 22.8 12.2
Fourormore symptoms
2.8 5.9 2.6 2.6 12.4 1.6
Sometimes,upto14daysduringthemonth;Almostalways,15to29dayspermonth;Always,everyday.
a Urinarysymptomscore:thesymptomsevaluatedwereurinaryincontinence,contentionmaneuvers,urinaryurgency,encopresis,
ofthechildren).Femaleshadmoreeliminationdysfunction symptomswhencomparedtomales(p<0.001).
Enuresis wasME in only 9.8% of children (10.8% males and8.3% of females) (Table 2). Among the enuretic chil-dren,37.4%hadsymptomsuptoonceaweek;32.9%,twoto fourtimesaweek;and26.2%,everyday,withnodifference betweengenders(p=0.134).
When comparing children with and without enuresis, urinaryandintestinalsymptomsweremorefrequentin chil-drenwithenuresis,inbothgenders(Table2).Thefrequency ofdaytimeurinaryincontinencewas4.8timeshigheramong enureticmalesand6timeshigheramongenureticfemales whencompared withtheirpeers (Table2).The daily fre-quencyof urinaryurgency or on most days of the month wasalso higher among enuretic children when compared tonon-enuretic ones. Among males, therewasno associ-ationbetweenenuresis andurinaryfrequencyor intervals greater than 72hours to evacuate. All urinary symptoms weremorecommoninenureticfemaleswhencomparedto non-enuretic.
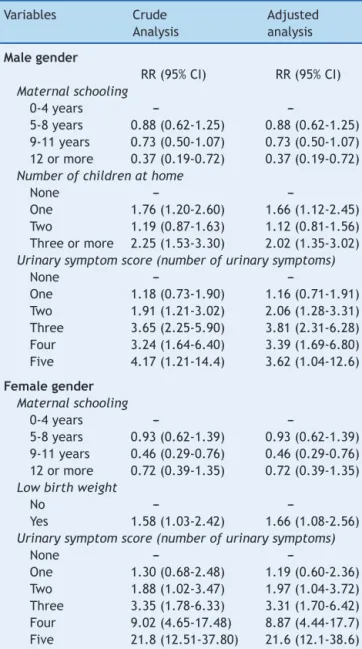
The multivariate analysis demonstrated that, in males (Table3), the numberof urinary symptomsand the num-berof children at home showeda direct association with thepresenceofenuresis,whereasmaternaleducationwas inversely related. In males, higher maternal education decreasedtheriskofenuresisandthehighernumberof uri-narysymptomsincreasedthisrisk;infemales,thepresence ofurinarysymptomsincreasedthechance ofhavingmore enuresis.Low birth weightwasassociated withmore fre-quentbedwettingepisodesonly in females.Analyses with isolatedsymptomspresentat4and6yearsshowedan asso-ciation of enuresis with urinary incontinence and urinary retentionmaneuvers,inbothgenders(datanotshown).
Discussion
Nocturnalenuresisisatypeofmorbiditythatinvolves sev-eral physiopathologic mechanisms.5 This study sought to describeitsoccurrence,classification,andassociated fac-tors,without describing itsphysiopathology.5 The present study did not assess the familial occurrence of enuresis, which is an important factor for its occurrence,14,15 and whetherthesechildrenhadalreadysoughttreatment.The feelingsofthechildren andtheirparentsregarding symp-tomswerealsonotconsidered,whichdidnotinterferewith thepresentresults,astheyareimportantforthetreatment, whichwasnottheapproachofthisstudy.
Oneadvantageofthepresentstudyisthefactthatitwas population-basedand used a questionnairewith symptom definitions according to the International Children Conti-nenceSociety (ICCS),15 providinginformation that canbe comparedtootherstudies.
Theprevalenceofenuresisisvariableintheliterature, especiallyduetothedefinitionsused,inadditiontocultural variationsamongthestudiedsites.Population-based stud-iesconductedinBrazil andother countriesarescarce, as mostsamplesconsistofambulatorypatientsor schoolchil-dren.Allanalyzedstudiesdemonstratedthattheprevalence ofenuresis decreasedwithage. The prevalenceof enure-sisinthisstudywas10.6%,whichwashigheramongmales, ofwhom 25% hadurinary leakage everynight. Mota,in a
Table3 Riskfactorsforenuresisusingmultivariate
analy-sis(Poissonregression)andhierarchicalmodelstratifiedby
gender.
Variables Crude
Analysis
Adjusted analysis
Malegender
RR(95%CI) RR(95%CI)
Maternalschooling
0-4years ---
---5-8years 0.88(0.62-1.25) 0.88(0.62-1.25)
9-11years 0.73(0.50-1.07) 0.73(0.50-1.07)
12ormore 0.37(0.19-0.72) 0.37(0.19-0.72)
Numberofchildrenathome
None ---
---One 1.76(1.20-2.60) 1.66(1.12-2.45)
Two 1.19(0.87-1.63) 1.12(0.81-1.56)
Threeormore 2.25(1.53-3.30) 2.02(1.35-3.02)
Urinarysymptomscore(numberofurinarysymptoms)
None ---
---One 1.18(0.73-1.90) 1.16(0.71-1.91)
Two 1.91(1.21-3.02) 2.06(1.28-3.31)
Three 3.65(2.25-5.90) 3.81(2.31-6.28)
Four 3.24(1.64-6.40) 3.39(1.69-6.80)
Five 4.17(1.21-14.4) 3.62(1.04-12.6)
Femalegender
Maternalschooling
0-4years ---
---5-8years 0.93(0.62-1.39) 0.93(0.62-1.39)
9-11years 0.46(0.29-0.76) 0.46(0.29-0.76)
12ormore 0.72(0.39-1.35) 0.72(0.39-1.35)
Lowbirthweight
No ---
---Yes 1.58(1.03-2.42) 1.66(1.08-2.56)
Urinarysymptomscore(numberofurinarysymptoms)
None ---
---One 1.30(0.68-2.48) 1.19(0.60-2.36)
Two 1.88(1.02-3.47) 1.97(1.04-3.72)
Three 3.35(1.78-6.33) 3.31(1.70-6.42)
Four 9.02(4.65-17.48) 8.87(4.44-17.7)
Five 21.8(12.51-37.80) 21.6(12.1-38.6)
Poissonregression:Inthefirstlevel,thevariableseducation, age,ethnicityandmaternalsocioeconomicstatus;secondlevel, prematurity,lowbirthweight,andnumberofchildrenathome; thirdlevel,thescoresofurinarysymptomsandprevioushistory ofurinarytractinfection.Variableswithp<0.05didnotremain inthemodel.
CI,confidenceinterval.
In2007,Cuneytassessed1,500schoolchildrenandfound aprevalenceofenuresisof22.2%inmalesand18%infemales aged7 years, and25.3% and 19.2% aged8 years, respec-tively; among all children studied, 33.3% had symptoms everynight.18Gumus,in1999,foundaprevalenceof16.9% in malesand 10.6% infemales between 7 and11 years,19 and,in2004,EmelGurobservedaprevalence of19.8%in children aged 6 to10 years.20 In 7,012 Italian schoolchil-dren, the occurrence of enuresis was lower,3.9%, with a predominanceofmales.21
In a study of schoolchildren from the Democratic RepublicoftheCongo,CentralAfrica,theprevalencewas 34.5% at 7 years and 30% at 8 years, higher than that observedin EuropeanandAmericancountries.22 Ina sam-pleofschoolchildrenfromIran,theprevalenceofenuresis between5and7yearswas9%andbetween8and10years, of6.9%.Thefrequency ofoverfivenightsaweekwas3%, withnodifferencesbetweenthegenders.23Inanotherstudy in Iranianschoolchildren aged 7to 11 years,therewas a prevalenceof 18.7%witha predominanceofmales (20.9%
vs.16.5%);symptomsdecreasedasageincreased.24 Theconcomitantoccurrenceofotherlowerurinarytract dysfunctionsymptomsisofutmostimportance,asthe phy-siopathological characteristics and therapeutic strategies differfromthemanagementofMEenuresis.Mostchildren had NME enuresis (85%),which has been also observedin currentstudies.16,18,19Themostfrequentlyreportedurinary symptomswere retentionmaneuvers andurinaryurgency. Thesesymptomsmaybeassociatedwithdysfunctionsofthe lowerurinarytract,especiallyhyperactivebladder,2which needstobemanagedbeforethetreatmentofenuresis.
Enuresis is acommon pathologyin children from fami-lieswithloweducationalandsocioeconomicstatus.Itmay cause secondary psychological disorders and problems of social and familial adaptation. The highest prevalence of enuresiswasobservedinchildrenofmotherswithlower edu-cationlevels,oflowersocioeconomicstatus,andinfamilies with more children, demonstrating a significant variation between different social levels. The studies by Cuneyt, Gumus, Emel Gur, and Chiozza had similar findings, with adirectassociation betweenenuresis andmorenumerous familieswithlowerlevelofschooling.18---21
The initialevaluation of enuretic children can be con-ductedthroughadetailedhistoryandphysicalexamination, withouttheneedforlaboratoryorinvasivetests.25The eval-uationofotherurinaryandintestinalsymptomsformsthis detailed history and is necessary for the classification of enuresis, aswell asfortherapeutic guidance.The urinary symptom score16,26 wasshown to bea good tool for ade-quateevaluationoftheurinarypatternandhasbeenused inotherstudies.16,26---28
Childhealth monitoringisa uniqueopportunity for the pediatriciantoprevent,diagnose,andtreatchildhood mor-bidities.Enuresisanditsassociatedsymptomsareprevalent andshouldbeinvestigatedinclinicalpractice,especiallyin childrenoflowersocioeconomicstatus.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Gurbuz A,Karateke A, KabacaC.Enuresisin childhood, and urinaryand fecalincontinenceinadultlife: dotheysharea commoncause?BJUInt.2005;95:1058---62.
2.Yeung CK. Nocturnal enuresis (bedwetting). Curr OpinUrol. 2003;13:337---43.
3.YeungCK,SreedharB,SihoeJD,SitFK,LauJ.Differencesin characteristicsofnocturnalenuresisbetweenchildrenand ado-lescents:acriticalappraisalfromalargeepidemiologicalstudy. BJUInt.2006;97:1069---73.
4.HjalmasK,ArnoldT,BowerW,CaioneP,ChiozzaLM,VonGotard A,etal.Nocturnalenuresis:aninternationalevidencebased managementstrategy.JUrol.2004;171:2545---61.
5.Harari MD. Nocturnal enuresis. J Paediatr Child Health. 2013;49:264---71.
6.Franco I, von Gontard A, De Gennaro M. Evaluation and treatment of non monosymptomatic nocturnal enuresis: a standardization document from the International Children’s ContinenceSociety.JPediatrUrol.2013;9:234---43.
7.Barros AJ, da Silva dos Santos I, Victora CG, Albernaz EP, DominguesMR,TimmIK,etal.The2004Pelotasbirthcohort: methodsanddescription.RevSaudePublica.2006;40:402---13.
8.SantosIS,BarrosAJ,MatijasevichA,DominguesMR,BarrosFC, VictoraCG.Cohortprofile:the2004Pelotas(Brazil)birthcohort study.IntJEpidemiol.2011;40:1461---8.
9.ReportoftheExpertCommitteeontheInternational Classifi-cationofDiseases-10threvision:firstmeeting.Geneva:World
HealthOrganization;1984.
10.Gmitrowicz A, Kucharska A. Developmental disordersin the fourtheditionoftheAmericanclassification:diagnosticand sta-tisticalmanualofmentaldisorders(DSMIV– optionalbook). PsychiatrPol.1994;28:509---21.
11.NeveusT,vonGotardA,HoebekeP,HjalmasK,BauerS,Bower W, et al. The standardization of terminology of lower uri-nary tract function inchildrenand adolescents: reportfrom theStandardisationCommitteeoftheInternationalChildren’s ContinenceSociety.JUrol.2006;176:314---24.
12.MotaDM,BarrosAJ,SantosI,MatijasevichA.Characteristics ofintestinalhabitsinchildrenyoungerthan4years:detecting constipation.JPediatrGastroenterolNutr.2012;55:451---6.
13.Barros AJ, Victora CG.A nationwide wealth score based on the 2000 Brazilian demographic census. Rev Saude Publica. 2005;39:523---9.
14.Arnell H, Hjalmas K, Jagervall M, Lackgren G, Stenberg A, BengtssonB,etal.Thegeneticsofprimarynocturnalenuresis: inheritanceandsuggestionofasecondmajorgeneon chromo-some12q.JMedGenet.1997;34:360---5.
15.Bauer SB, Néveus T, von Gontard A, Hoebeke P, Bower W, Jorgensen TM, et al. Standardizing terminology in pediatric urology.JPediatrUrol.2007;3:163.
16.MotaDM,VictoraCG,HallalPC.Investigac¸ãodedisfunc¸ão mic-cionalemumaamostrapopulacionaldecrianc¸asde3a9anos. JPediatr(RioJ).2005;81:225---32.
17.ButlerRJ,GoldingJ,NorthstoneK.Nocturnalenuresisat7.5 years old:prevalence and analysisofclinicalsigns.BJU Int. 2005;96:404---10.
18.Ozden C,Ozdal OL, Altinova S, Oguzulgen I,Urgancioglu G, MemisA.Prevalenceandassociatedfactorsofenuresisin Turk-ishchildren.IntBrazJUrol.2007;33:216---22.
19.GumusB,VurgunN,LekiliM,IscanA,MuezzinogluT,Buyuksu C. Prevalence of nocturnal enuresis and accompanying fac-tors in children aged 7-11 years in Turkey. Acta Paediatr. 1999;88:1369---72.
21.ChiozzaML,BernardinelliL,CaioneP,DelGadoR,FerracaP, GiorgiPL,etal.AnItalianepidemiologicalmulticentrestudyof nocturnalenuresis.BrJUrol.1998;81Suppl3:86---9.
22.AloniMN,EkilaMB,EkuluPM,AloniML,MagogaK.Nocturnal enuresisinchildreninKinshasa,DemocraticRepublicofCongo. ActaPaediatr.2012;101:e475---8.
23.Safarinejad MR. Prevalence of nocturnal enuresis, risk fac-tors, associated familial factors and urinary pathology among school children in Iran. J Pediatr Urol. 2007;3: 443---52.
24.Hashem M, Morteza A, Mohammad K, Ahmad-Ali N. Preva-lenceofnocturnalenuresisinschoolagedchildren:theroleof personaland parentsrelatedsocio-economicandeducational factors.IranJPediatr.2013;23:59---64.
25.NeveusT.Nocturnalenuresis-theoreticbackgroundand practi-calguidelines.PediatrNephrol.2011;26:1207---14.
26.FarhatW, BagliDJ,CapolicchioG,O’ReillyS,MerguerianPA, Khoury A. The dysfunctionalvoiding scoringsystem: quanti-tative standardization of dysfunctional voiding symptoms in children.JUrol.2000;164:1011---5.
27.CaladoAA,AraújoEM,BarrosoJrU,NetoJM,FilhoMZ,Macedo JrA,etal.Cross-culturaladaptationofthedysfunctional void-ingscoresymptom(DVSS)questionnaireforBrazilianchildren. IntBrazilJUrol.2010;36:458---63.