Association of handgrip strength with
self-reported diseases in adults in
Rio Branco, Acre State, Brazil:
a population-based study
Associação da força de preensão manual com
morbidades referidas em adultos de Rio Branco,
Acre, Brasil: estudo de base populacional
Asociación entre la fuerza de prensión manual
con las morbilidades referidas en adultos de Rio
Branco, Acre, Brasil: estudio de base poblacional
1 Instituto Federal do Acre, Rio Branco, Brasil. 2 Escola Nacional de Saúde Pública Sergio Arouca, Fundação Oswaldo Cruz, Rio de Janeiro, Brasil.
3 Centro de Ciências da Saúde e do Desporto, Universidade Federal do Acre, Rio Branco, Brasil.
4 Departamento de Educação Física, Universidade Federal de Rondônia, Porto Velho, Brasil.
Correspondence C. A. Amaral
Instituto Federal do Acre. Av. Brasil 920, Rio Branco, AC 69903-068, Brasil.
Cledir de Araújo Amaral 1 Margareth Crisóstomo Portela 2 Pascoal Torres Muniz 3
Edson dos Santos Farias 4 Thiago Santos de Araújo 3 Orivaldo Florêncio de Souza 3
Abstract
This study aimed to analyze the association of handgrip strength with self-reported diseases and multimorbidity among adults in Rio Branco, Acre State, Brazil, through a population based survey involving 1,395 adults of both sexes. Associations by sex were estimated by logistic regression analysis. The mean handgrip strength in men (44.8kg) is higher than in women (29kg) and decrease with age. The mean handgrip strength difference between those classified as strong and weak was 21kg and 15.5kg for men and woman, respectively. Controlling for age group, body mass index and physical activity when it was relevant, men with low handgrip strength were more likely to have hypertension [OR = 2.21 91.35; 3.61)], diabetes [OR = 4.18 (1.35; 12.95)], musculoskeletal disorders [OR = 1.67 (1.07; 2.61)] and multimorbidity [OR = 1.99 (1.27; 3.12)]. Among woman, associations between handgrip strength and cardiovascular disease, dyslipidemia, musculoskeletal disorders and multimorbidity were not sustained in the multivariate models. This study endorses the use of handgrip strength as a health biomarker.
Handgrip Strength; Morbidity; Health Surveys
Resumo
Este estudo objetivou analisar a associação da for-ça de preensão manual com morbidades referidas e multimorbidade em adultos de Rio Branco, Acre, Brasil, mediante inquérito de base populacional com 1.395 adultos de ambos os sexos. As associa-ções, por sexo, foram estimadas com a técnica de regressão logística. A média de força de preensão manual nos homens (44,8kg) é maior que entre as mulheres (29kg) e reduz com a idade. A dife-rença da força de preensão manual média entre aqueles classificados como fortes e fracos foi 21kg e 15,5kg, para homens e mulheres, respectivamente. Controlando para a faixa etária, índice de massa corporal e atividade física quando relevante, ho-mens com baixa força de preensão manual tive-ram maiores chances de ocorrência de hipertensão [OR = 2,21 (1,35; 3,61)], diabetes [OR = 4,18 (1,35; 12,95)], distúrbio musculoesquelético [OR = 1,67 (1,07; 2,61)] e multimorbidade [OR = 1,99 (1,27; 3,12)]. Nas mulheres, associações entre força de preensão manual e evento cardiovascular, dislipi-demia, distúrbio muscolesquelético e multimorbi-dade não se mantiveram nos modelos multivaria-dos. Este estudo endossa o uso da força de preensão manual como biomarcador de saúde.
Introduction
Handgrip strength is recognized as an estima-tor of overall strength and has been presented as a biomarker for important health outcomes 1. Studies with predominantly middle-aged and el-derly individuals show that low handgrip strength is associated with sarcopenia 2, functional limi-tations and disabilities 3, falls 4, decreased bone mineral density, and increased fracture risks 5, and is considered a useful marker for frailty in the elderly 6. Among men 40 to 68 years of age followed for 25 years, low handgrip strength was predictive of functional limitations and disabili-ties, while higher handgrip strength apparently protected against these conditions in old age, in-dicating that handgrip strength can be used for early screening of individuals at increased risk of physical disability in old age 4. Mean decline in handgrip strength during the follow-up period was 8-9kg and was inversely associated with age and blood glucose, but directly associated with cognitive function, body mass index (BMI), and hemoglobin level 7.
In addition to disorders inherent to the muscu-loskeletal system, low handgrip strength has also been associated with changes in nutritional sta-tus 8, post-surgical clinical complications 9, length of hospital stay 10, various chronic diseases 11,12, and mortality 13, although the mechanisms of these associations are not well understood.
Low handgrip strength has been associated with increased odds of anxiety, stroke, chronic kidney disease (CKD), chronic obstructive pul-monary disease (COPD), and hyperthyroidism in men and anemia, falls, and kyphosis in wom-en 10. Among men and women 30 to 72 years of age followed for 22 years, handgrip strength de-cline was associated with incidence of chronic diseases such as cardiovascular events, diabetes mellitus, chronic bronchitis, chronic back pain, hypertension, and asthma as well as impor-tant weight loss, physical inactivity, and persis-tent smoking 12. According to a Brazilian study, women with metabolic syndrome showed lower mean handgrip strength than healthy ones 14. A study in men in the United States found a protec-tive effect of muscle strength against metabolic diseases, regardless of cardiopulmonary fitness and overweight 15. Several studies have found an association between diabetes mellitus and de-creased handgrip strength 16,17,18.
The 37-year follow-up of a cohort of one mil-lion men starting with their enlistment in the Swedish Army (mean age 18.2 years) identified an inverse relationship between handgrip strength and risk of heart disease and stroke 19. Mean-while, the seven-year monitoring of older elderly
elders with higher initial handgrip strength, re-gardless of gender, with handgrip strength being an important predictor of mortality 13.
Potential prediction of morbidity based on measurement of handgrip strength suggests the variable’s use as a biomarker in the assessment of health conditions in the population. This empha-sizes the importance of accumulating knowledge from studies in different contexts to determine cut-off points for different diseases, not currently available in the literature.
Despite evidence from international studies, we are unaware of any epidemiological study on the topic in Brazil and that includes a wide age spectrum. The current study thus aimed to be-gin filling this gap by analyzing the association between handgrip strength and specific diseases and multimorbidity among adults in Rio Branco, Acre State, Brazil.
Methods
A cross-sectional study was conducted with adults in Rio Branco, under the research proj-ect Health and Nutrition of Children and Adults in Rio Branco, Acre, from November 2007 to Oc-tober 2008.
A two-stage probabilistic cluster sample was used, with 35 census tracts as the primary units, 31 in the urban area and four in the rural area. Twenty-five households were randomly selected in each census tract and represented the second-ary units, increased by 15% to compensate for losses or refusals, totaling 977 households, where all residents 18 years or older and able to an-swer the questions were asked to participate in the study.
The selected sample consisted of 1,516 adults from 18 to 96 years of age (the procedures have been presented elsewhere 20). Pregnant women and participants who did not perform the hand-grip strength test were excluded from the survey, leading to a loss of 121 subjects (7.8%), with no statistically significant difference according to socio-demographic profile. The final sample in-cluded 1,395 participants, considering the demo-graphic characteristics (age and gender), leisure-time physical activity, and self-reported diseases, as well as the biometric variables height, weight, and handgrip strength.
by the American Society of Hand Therapists 21. The handgrip strength score was the higher value of two measurements of the dominant hand. In-dividuals were classified into tertiles according to their handgrip strength score – strong (highest tertile), moderate strength (middle tertile), and weak (lowest tertile).
The dependent variables for self-reported diseases were identified by the individual’s ac-count of diagnosis by a health professional for the following conditions: hypertension, diabetes mellitus, cardiovascular events (myocardial in-farction, stroke), dyslipidemia (high cholesterol or triglycerides), depression, chronic kidney dis-ease, and musculoskeletal disorders (tendonitis, repetitive strain injury, spine or back disease, arthritis, non-infectious rheumatism, gout, and osteoporosis). The multimorbidity variable was built adopting the definition of the simultaneous occurrence of two or more chronic diseases in the same individual. A value of 1 for “yes” and 2 for “no” was assigned to each variable indicating occurrence of the disease.
The covariates were age, leisure-time physi-cal activity, and BMI. Age was categorized in two groups, 18-39 years and 40 years and older. Lei-sure-time physical activity was defined accord-ing to weekly frequency and duration. Accord-ing to recommendations by the World Health Organization (WHO) 22, individuals totaling 150 minutes of moderate physical activity or 75 min-utes of vigorous activity were classified as active, and those who did not achieve these levels were considered sedentary. BMI was defined as weight divided by height-squared, using WHO 23 cutoff points: underweight (BMI < 18.5); normal weight (BMI = 18.5 to 24.9); overweight (BMI 25 to 29.9); and obese (BMI ≥ 30).
Data were double-entered and validated us-ing Epi Info 6.04 (Centers for Disease Control and Prevention, Atlanta, USA).
In the descriptive analysis, we verified the ab-solute and relative frequencies of all the variables analyzed by gender and the estimated differenc-es in frequencidifferenc-es between men and women using Pearson’s chi-square test, with significance set at α = 0.05.We also obtained handgrip strength measures of central tendency and dispersion ac-cording to gender and age group.
For men and women, logistic regression models estimated the magnitude of association as odds ratio (OR) between the dependent vari-ables indicating diseases and handgrip strength in tertiles, with the highest handgrip strength ter-tile (strong) as the reference. Three models were estimated for each dependent variable: the first model focused on crude association between disease and handgrip strength; the second model
on age group-adjusted association; and the third model on association adjusted for age group, BMI, and when relevant, leisure-time physical activity. Age group-handgrip strength interaction was tested. Significance was set at α = 0.05.
All the analyses took into account the ef-fect of the sample design and weights of obser-vations, using SAS version 9.3 (SAS Inst., Cary, USA) surveyfreq, surveymeans, and surveylogistic procedures.
The research project that collected the data used in this study was approved by the Ethics Research Committee of the Federal University of Acre under Protocol n. 2307.001150/2007-22 and obtained informed consent from each participant.
Results
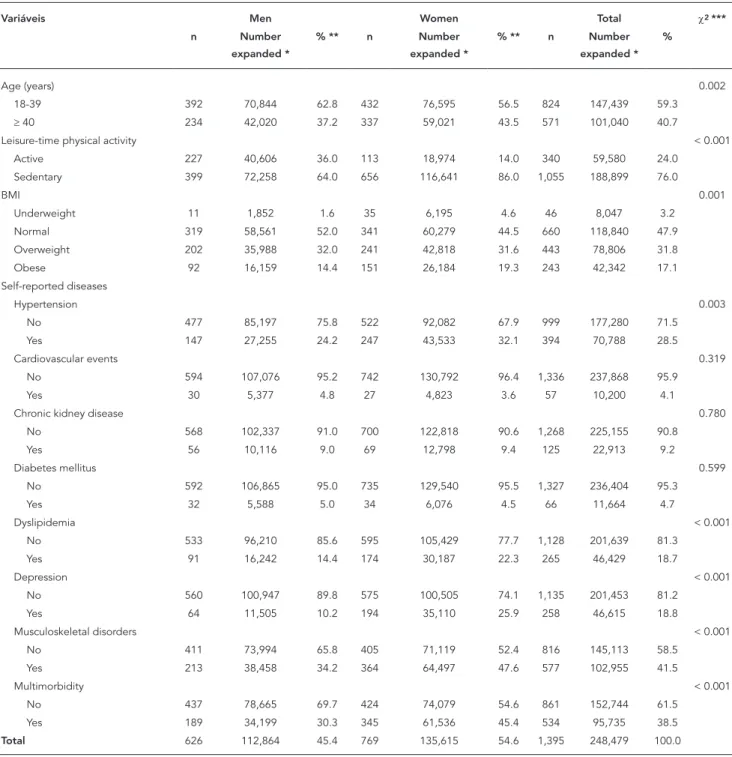
With the sample expansion using the sampling weights, the 1,395 observations corresponded to 248,479 individuals. Estimates point to a pre-dominantly female population (54.6%) aged up to 39 years (59.3%). There were statistically sig-nificant differences (p < 0.05) between genders in the distributions of type of physical activity, BMI, hypertension, dyslipidemia, depression, musculoskeletal disorders, and multimorbidity (Table 1).
Overall mean handgrip strength was 36kg (44.8kg in men and 29kg in women). Regardless of gender, handgrip strength was also higher in the 18-39-year age group than in 40 years and over. In the handgrip strength analysis per tertile, strong and weak men had a mean handgrip strength of 55.3kg and 34.1kg, respectively, while strong and weak women had a mean handgrip strength of 36.1kg and 20.6kg, respectively (Table 2).
Lei-Socio-demographic and health characteristics of adults in Rio Branco, Acre State, Brazil, 2007-2008.
Variáveis Men Women Total χ2 ***
n Number expanded *
% ** n Number expanded *
% ** n Number expanded *
%
Age (years) 0.002
18-39 392 70,844 62.8 432 76,595 56.5 824 147,439 59.3
≥ 40 234 42,020 37.2 337 59,021 43.5 571 101,040 40.7
Leisure-time physical activity < 0.001
Active 227 40,606 36.0 113 18,974 14.0 340 59,580 24.0
Sedentary 399 72,258 64.0 656 116,641 86.0 1,055 188,899 76.0
BMI 0.001
Underweight 11 1,852 1.6 35 6,195 4.6 46 8,047 3.2
Normal 319 58,561 52.0 341 60,279 44.5 660 118,840 47.9
Overweight 202 35,988 32.0 241 42,818 31.6 443 78,806 31.8
Obese 92 16,159 14.4 151 26,184 19.3 243 42,342 17.1
Self-reported diseases
Hypertension 0.003
No 477 85,197 75.8 522 92,082 67.9 999 177,280 71.5
Yes 147 27,255 24.2 247 43,533 32.1 394 70,788 28.5
Cardiovascular events 0.319
No 594 107,076 95.2 742 130,792 96.4 1,336 237,868 95.9
Yes 30 5,377 4.8 27 4,823 3.6 57 10,200 4.1
Chronic kidney disease 0.780
No 568 102,337 91.0 700 122,818 90.6 1,268 225,155 90.8
Yes 56 10,116 9.0 69 12,798 9.4 125 22,913 9.2
Diabetes mellitus 0.599
No 592 106,865 95.0 735 129,540 95.5 1,327 236,404 95.3
Yes 32 5,588 5.0 34 6,076 4.5 66 11,664 4.7
Dyslipidemia < 0.001
No 533 96,210 85.6 595 105,429 77.7 1,128 201,639 81.3
Yes 91 16,242 14.4 174 30,187 22.3 265 46,429 18.7
Depression < 0.001
No 560 100,947 89.8 575 100,505 74.1 1,135 201,453 81.2
Yes 64 11,505 10.2 194 35,110 25.9 258 46,615 18.8
Musculoskeletal disorders < 0.001
No 411 73,994 65.8 405 71,119 52.4 816 145,113 58.5
Yes 213 38,458 34.2 364 64,497 47.6 577 102,955 41.5
Multimorbidity < 0.001
No 437 78,665 69.7 424 74,079 54.6 861 152,744 61.5
Yes 189 34,199 30.3 345 61,536 45.4 534 95,735 38.5
Total 626 112,864 45.4 769 135,615 54.6 1,395 248,479 100.0
BMI: body mass index.
* Number expanded from weights and sample design; ** Percentage from number expanded;
*** p-value of Pearson’s chi-square test.
sure-time physical activity was positively associ-ated with multimorbidity.
Table 4 presents the results corresponding to the previous table but for women, showing
Table 2
Distribution of handgrip strength in kg by age group and handgrip strength tertile by gender in adults in Rio Branco, Acre State, Brazil, 2007-2008.
Age group Mean Median Minimum * Maximum ** Standard error
Coefficient of variation
Men
18-39 years 46.6 45.8 18 83 0.48 0.010
≥ 40 years 41.6 41.4 12 77 0.81 0.020
Handgrip strength
Strong 55.3 54.0 50 83 0.37 0.006
Moderate 44.9 45.0 41 49 0.17 0.004
Weak 34.2 36.0 12 40 0.43 0.011
Total 44.8 44.4 12 83 0.50 0.011
Mulher
18-39 years 30.5 29.8 11 60 0.34 0.011
≥ 40 years 27.0 26.8 10 46 0.46 0.017
Handgrip strength
Strong 36.0 35.0 32 60 0.25 0.007
Moderate 28.4 28.0 26 31 0.09 0.004
Weak 20.6 21.0 10 25 0.23 0.011
Total 29.0 28.6 10 60 0.35 0.012
Total 36.1 33.9 10 83 0.36 0.010
* Minimum: lower limit; ** Maximum: higher limit.
Table 3
Logistic regression analysis of handgrip strength tertiles and self-reported diseases in men in Rio Branco, Acre State, Brazil, 2007-2008.
Reported diseases OR (95%CI) (model 1) *
OR (95%CI) (model 2) **
OR (95%CI) (model 3) ***
Hypertension Handgrip strength
Strong 1.00 1.00 1.00
Moderate 1.89 (1.19; 3.00) 1.77 (1.08; 2.90) 2.05 (1.19; 3.54)
Weak 2.31 (1.47; 3.64) 1.72 (1.09; 2.69) 2.21 (1.35; 3.61) Age ≥ 40 years - 4.08 (2.52; 6.60) 3.53 (2.14; 5.83)
BMI - - 1.10 (1.04; 1.15)
p-value trend # < 0.001 0.021 0.001
% agreement ## 42.3 61.6 73.8
Cardiovascular event Handgrip strength
Strong 1.00 1.00 1.00
Moderate 1.52 (0.45; 5.19) 1.35 (0.40; 4.48) 1.42 (0.43; 4.68) Weak 2.53 (0.76; 8.51) 1.77 (0.57; 5.46) 1.83 (0.60; 5.58)
Age ≥ 40 years - 4.82 (2.08; 11.18) 4.38 (1.78; 10.78)
BMI - - 1.04 (0.96; 1.12)
p-value trend # 0.110 0.296 0.263
% agreement ## 42.1 59.5 67.4
Reported diseases OR (95%CI) (model 1) *
OR (95%CI) (model 2) **
OR (95%CI) (model 3) ***
Chronic kidney disease
Handgrip strength
Strong 1.00 1.00 1.00
Moderate 1.28 (0.64; 2.57) 1.21 (0.60; 2.44) 1.17 (0.57; 2.37) Weak 0.99 (0.50; 1.93) 0.82 (0.40; 1.69) 0.77 (0.36; 1.64) Age ≥ 40 years - 2.10 (1.03; 4.28) 2.21 (1.05; 4.64)
BMI - - 0.97 (0.93; 1.02)
p-value trend # 0.965 0.562 0.468
% agreement ## 36.1 52.6 60.0
Diabetes mellitus Handgrip strength
Strong 1.00 1.00 1.00
Moderate 1.62 (0.58; 4.57) 1.42 (0.49; 4.14) 1.67 (0.54; 5.14) Weak 4.54 (1.50; 13.76) 3.16 (1.06; 9.47) 4.18 (1.35; 12.95) Age ≥ 40 years - 5.29 (2.20; 12.75) 4.31 (1.82; 10.23)
BMI - - 1.11 (1.05; 1.18)
p-value trend # 0.008 0.042 0.014
% agreement ## 50.8 69.8 79.5
Dyslipidemia Handgrip strength
Strong 1.00 1.00 1.00
Moderate 0.98 (0.55; 1.73) 0.83 (0.46; 1.50) 0.98 (0.52; 1.88) Weak 1.36 (0.78; 2.39) 0.88 (0.48; 1.62) 1.31 (0.71; 2.40) Age ≥ 40 years - 6.00 (3.86; 9.33) 5.16 (3.33; 7.99)
BMI - - 1.16 (1.10; 1.22)
p value trend # 0.277 0.716 0.382
% agreement ## 36.5 64.3 80.2
Depression Handgrip strength
Strong 1.00 1.00 1.00
Moderate 1.86 (0.93; 3.74) 1.78 (0.88; 3.57) 1.78 (0.88; 3.58)
Weak 0.87 (0.43; 1.76) 0.73 (0.35; 1.52) 0.73 (0.36; 1.50) Age ≥ 40 years - 2.01 (1.14; 3.55) 2.01 (1.12; 3.63)
BMI - - 1.00 (0.93; 1.07)
p-value trend # 0.673 0.340 0.339
% agreement ## 41.6 55.5 55.6
Musculoskeletal disorders Handgrip strength
Strong 1.00 1.00 1.00
Moderate 1.48 (0.96; 2.28) 1.38 (0.86; 2.19) 1.34 (0.85; 2.09) Weak 2.28 (1.45; 3.59) 1.76 (1.13; 2.74) 1.67 (1.07; 2.61)
Age ≥ 40 years - 3.61 (2.54; 5.14) 3.73 (2.54; 5.47)
BMI - - 0.98 (0.94; 1.02)
p-value trend # < 0.001 0.013 0.027
% agreement ## 42.2 60.9 68.3
Table 3 (continued)
Reported diseases OR (95%CI) (model 1) *
OR (95%CI) (model 2) **
OR (95%CI) (model 3) ***
Multimorbidity
Handgrip strength
Strong 1.00 1.00 1.00
Moderate 1.42 (0.93; 2.18) 1.30 (0.83; 2.02) 1.41 (0.90; 2.22) Weak 2.34 (1.51; 3.63) 1.72 (1.09; 2.73) 1.99 (1.27; 3.12) Age ≥ 40 years - 4.72 (3.35; 6.64) 3.80 (2.67; 5.41)
BMI - - 1.06 (1.01; 1.11)
Leisure-time physical activity - - 1.72 (1.09; 2.71)
p-value trend # < 0.001 0.022 0.003
% agreement ## 42.5 64.1 74.0
95%CI: 95% confidence interval; BMI: body mass index; OR: odds ratio. * Model 1: crude analysis;
** Model 2: adjusted for age;
*** Model 3: adjusted for age, BMI, and physical activity, when relevant; # p-value trend = trend test of OR between handgrip strenght tertiles; ## % agreement = model adherence percentage.
Table 4
Logistic regression analysis of handgrip strength tertiles and reported diseases in women in Rio Branco, Acre State, Brazil, 2007-2008.
Reported diseases OR (95%CI) (model 1) *
OR (95%CI) (model 2) **
OR (95%CI) (model 3) ***
Hypertension Handgrip strength
Strong 1.00 1.00 1.00
Moderate 0.81 (0.58; 1.13) 0.74 (0.51; 1.05) 0.90 (0.60; 1.36) Weak 1.17 (0.79; 1.74) 0.81 (0.53; 1.22) 1.03 (0.64; 1.64)
Age ≥ 40 years - 3.25 (2.47; 4.28) 2.22 (1.61; 3.05)
BMI - - 1.44 (1.05; 1.96)
p-value trend # 0.495 0.287 0.947
% agreement ## 38.1 57.7 73.4
Cardiovascular event
Handgrip strength
Strong 1.00 1.00 1.00
Moderate 0.89 (0.32; 2.44) 0.81 (0.30; 2.14) 0.81 (0.29; 2.25) Weak 2.46 (1.11; 5.47) 1.66 (0.72; 3.81) 1.65 (0.70; 3.89) Age ≥ 40 years - 4.09 (1.47; 11.36) 4.14 (1.59; 10.81)
BMI - - 1.00 (0.94; 1.06)
p-value trend # 0.037 0.233 0.246
% agreement ## 45.0 63.1 64.9
Reported diseases OR (95%CI) (model 1) *
OR (95%CI) (model 2) **
OR (95%CI) (model 3) ***
Chronic kidney disease
Handgrip strength
Strong 1.00 1.00 1.00
Moderate 0.65 (0.34; 1.25) 0.63 (0.33; 1.22) 0.65 (0.34; 1.24) Weak 0.69 (0.34; 1.39) 0.62 (0.31; 1.23) 0.64 (0.32; 1.26) Age ≥ 40 years - 1.41 (0.71;2.79) 1.36 (0.69; 2.66)
BMI - - 1.01 (0.97; 1.06)
p-value trend # 0.291 0.169 0.191
% agreement ## 37.4 47.0 54.5
Diabetes mellitus Handgrip strength
Strong 1.00 1.00 1.00
Moderate 0.90 (0.32; 2.49) 0.80 (0.29; 2.20) 0.78 (0.29; 2.09) Weak 1.34 (0.49; 3.70) 0.81 (0.31; 2.14) 0.87 (0.35; 2.19) Age ≥ 40 years - 6.70 (2.88; 15.58) 5.85 (2.33;1 4.66)
BMI - - 1.03 (0.96; 1.10)
p-value trend # 0.591 0.683 0.790
% agreement ## 37.6 63.7 71.9
Dyslipidemia Handgrip strength
Strong 1.00 1.00 1.00
Moderate 0.79 (0.51;1.22) 0.70 (0.46;1.05) 0.79 (0.52;1.18) Weak 1.63 (1.03;2.57) 1.05 (0.66;1.66) 1.25 (0.79;1.97) Age ≥ 40 years - 4.48 (3.16;6.35) 3.56 (2.37;5.39)
BMI - - 1.08 (1.03;1.12)
p value trend # 0.055 0.862 0.369
% agreement ## 42.0 62.7 74.1
Depression Handgrip strength
Strong 1.00 1.00 1.00
Moderate 1.04 (0.72;1.50) 1.01 (0.70;1.46) 1.06 (0.73;1.54)
Weak 1.38 (0.93;2.04) 1.16 (0.77;1.75) 1.23 (0.82;1.87) Age ≥ 40 years - 1.73 (1.35;2.21) 1.59 (1.19;2.13)
BMI - - 1.03 (0.99;1.06)
p-value trend # 0.122 0.487 0.327
% agreement ## 36.6 44.5 59.1
Musculoskeletal disorders Handgrip strength
Strong 1.00 1.00 1.00
Moderate 0.92 (0.67;1.27) 0.84 (0.61;1.14) 0.83 (0.60;1.14) Weak 1.73 (1.23;2.44) 1.17 (0.78;1.76) 1.16 (0.76;1.78)
Age ≥ 40 years - 3.84 (2.85;5.17) 3.85 (2.80;5.30)
BMI - - 1.00 (0.97;1.03)
p-value trend # 0.002 0.528 0.553
% agreement ## 40.2 60.5 66.8
Table 4 (continued)
Reported diseases OR (95%CI) (model 1) *
OR (95%CI) (model 2) **
OR (95%CI) (model 3) ***
Multimorbidity
Handgrip strength
Strong 1.00 1.00 1.00
Moderate 0.89 (0.64;1.23) 0.78 (0.55;1.11) 0.87 (0.61;1.23) Weak 1.70 (1.18;2.45) 1.06 (0.71;1.59) 1.24 (0.83;1.85) Age ≥ 40 years - 4.93 (3.73;6.50) 4.10 (3.07;5.48)
BMI - - 1.07 (1.03;1.10)
p-value trend # 0.006 0.859 0.337
% agreement ## 40.5 62.9 73.8
95%CI: 95% confidence interval; BMI: body mass index; OR: odds ratio. * Model 1: crude analysis;
** Model 2: adjusted for age;
*** Model 3: adjusted for age, BMI, and physical activity, when relevant; # p-value trend = trend test of OR between handgrip strenght tertiles; ## % agreement = model adherence percentage.
Interaction terms between age and handgrip strength were tested in the multivariate models in Table 3 and 4, but were not statistically signifi-cant (p < 0.05).
Discussion
The results showed associations between hand-grip strength and self-reported hypertension, diabetes, musculoskeletal disorders and multi-morbidity in men only. Reduced muscle strength, a condition known as dynapenia 2, was observed in the 40-and-over age group.
The study found significant differences in the magnitude and gradient of muscle strength be-tween men and women, corroborating previous studies 11,24, which can be explained by hormon-al differences inherent to gender.
There was no statistically significant as-sociation between low handgrip strength and the cardiovascular events. However, metabolic syndrome, an important risk factor for cardio-vascular disease that results precisely from the combination of dyslipidemia, hyperglycemia, and hypertension 25, was shown to be individu-ally associated with handgrip strength in men. The components of metabolic syndrome are thus associated with chronic systemic inflammation and increased interleukin-1 and -6 (IL-1 and IL-6) and tumor necrosis factor-alpha (TNF-α) 26. High levels of inflammatory markers such as IL-6 and C-reactive protein (CRP) increase the risk of mus-cle strength loss in older men and women 27, who thus tend to decline in physical function and
in-crease in functional disability, dependence in ac-tivities of daily living, and mortality 28,29. Evidence have been reported on the progressive reduction of handgrip strength in the presence of cata-bolic biomarkers (CRP, IL-6, IL-1RA, TNF-α) 30, which increase oxidative stress, reducing muscle mass and causing consequent loss of strength in the elderly 2,31,32.
The present results corroborate other stud-ies showing that diabetic men have lower hand-grip strength than their non-diabetic peers, but the same was not evident among women 11,17. Prospective studies indicate that type-2 diabetes reduces muscle strength and mass 18, and that higher strength protects against the develop-ment of diabetes 33. In vitro and in vivo clinical evidence attests that hyperglycemia affects con-tractile function and muscle strength 34.
This study also agrees with others identify-ing the association between low strength and hy-pertension in men, but not in women 35,36. It has been reported that resistance training appears to prevent metabolic disorders such as dyslip-idemia, impaired fasting glucose, pre-hyperten-sion, and increased waist circumference, but not hypertension 37, while recognizing that increased strength may improve vascular health and reduce complications 38 and mortality among hyperten-sive individuals 39. The statistical association be-tween handgrip strength and hypertension may mean that muscle strength expresses overall in-dividual fitness 40 more than a direct relationship with hypertension.
between handgrip strength and overall strength, which itself reflects operation of the musculo-skeletal system 1. Low strength has already been associated with history of falls in both sexes and with kyphosis in women 11. This study’s findings thus highlight the importance of using handgrip strength as a health biomarker, realizing that re-duced levels of muscle strength may lead to dis-ability and functional limitations, particularly among older individuals 2,3,41. The assessment of handgrip strength during middle age could al-low early identification of risks of future disabil-ity 3, dependence in activities of daily living, and cognitive decline in older age 4. It can also play a role in predicting fracture risks 5 and tracking sarcopenia 2.
Part of the modeling process in this study fo-cused on differentiating between individuals 60 years and older and 40-59 years of age, confirm-ing the role of agconfirm-ing in the occurrence of diseases and providing relatively consistent results. How-ever, the small number of strong individuals in the 60-and-older group, especially among men, led to loss of power in the inferences.
Future studies should contribute to under-standing the effect of handgrip strength in older
in the role of handgrip strength as a predictor of morbidity between men and women.
As far as we know, this is the first study to test interaction between handgrip strength and age when assessing the association between hand-grip strength and diseases. The findings do not indicate potentiation or attenuation of the effect of low handgrip strength with older age in the oc-currence of diseases.
The study has some limitations, such as the inability to make causal inferences. The statis-tical associations should only be considered as such, with due caution concerning assumptions about which variables precede which. Another limitation is the lack of clinical parameters for diseases, although self-reported chronic diseases express an approximate measure of the informa-tion obtained by clinical examinainforma-tion 42.
We highlight that this research was unprece-dented in Brazil, as the first Brazilian population-based study with adults that assesses handgrip strength and diseases. The models used here also considered the effect of handgrip strength adjusted by the main variables published in the literature: age, BMI, and leisure-time physical activity.
Resumen
El objetivo fue analizar la asociación de la fuerza de prensión manual con las morbilidades y multimorbi-lidad entre los adultos en Rio Branco, Acre, Brasil, me-diante una encuesta poblacional con 1.395 adultos de ambos sexos. Las asociaciones, por sexo, se estimaron mediante regresión logística. La media de la fuerza de prensión manual en los hombres (44,8kg) es mayor que en las mujeres (29kg) y disminuye con la edad. La di-ferencia de la fuerza de prensión manual media entre los clasificados como fuertes y débil fue 21kg y 15,5kg para hombres y mujeres, respectivamente. Controlan-do por edad, índice de masa corporal y la actividad física, cuando sea pertinente, los hombres con baja
fuerza de prensión manual son más propensos a sufrir de hipertensión [OR = 2,21 (1,35; 3,61)], diabetes [OR = 4,18 (1,35; 12,95), trastorno musculoesquelético [OR = 1,67 (1,07; 2,61)] y multimorbilidad [OR = 1,99 (1,27; 3,12)]. Entre las mujeres, las asociaciones entre fuerza de prensión manual y evento cardiovascular, dislipide-mia, trastorno musculoesquelético y multimorbilidad no se mantuvieron en los modelos multivariados. Este estudio respalda el uso de fuerza de prensión manual como un biomarcador de la salud.
Conclusion
The findings confirm the association between low handgrip strength and chronic diseases, musculo-skeletal disorders, and multimorbidity among men, supporting the measurement of muscle strength with a hand-held dynamometer as a useful, relatively low-cost, and easy-to-apply marker for clinical evaluation and monitoring of individual health conditions, espe-cially in primary care.
The study also indicates the need for further epi-demiological research to improve our understanding of the findings based on clinical parameters for diseases and focused on specific age groups, explaining the dif-ferences between men and women and contributing to proposals of reference values and cutoff points for health risks.
Contributors
C. A. Amaral participated in the data processing, analy-sis, and interpretation, literature review, and writing of the article. M. C. Portela collaborated in the analysis and interpretation of the results presented in the new version, as well as in the final revision. P. T. Muniz and T. S. Araújo contributed to the data collection and criti-cal revision of the article. E. S. Farias participated in the critical revision and approval of the final version. O. F. Souza collaborated in the data organization, analysis, and interpretation, critical revision of the article, and approval of the final version.
Acknowledgments
The authors wish to thank the agencies CNPq (Call for Projects, UFAC-FIOCRUZ, case n. 620024/2008-9) and Capes (PROCAD-NF 1442/2007 and PROCAD-NF 2557/2008 programs) for funding the program of col-laboration between the Master’s Program in Collective Health at the Federal University of Acre and the Gradu-ate Studies Program in Public Health and the Environ-ment at the Oswaldo Cruz Foundation.
References
1. Bohannon RW. Are hand-grip and knee extension strength reflective of a common construct? Per-cept Mot Skills 2012; 114:514-8.
2. Manini TM, Clark BC. Dynapenia and aging: an update. J Gerontol A Biol Sci Med Sci 2012; 67: 28-40.
3. Rantanen T, Guralnik JM, Foley D, Masaki K, Lev-eille S, Curb JD, et al. Midlife hand grip strength as a predictor of old age disability. JAMA 1999; 281:558-60.
4. Taekema DG, Gussekloo J, Maier AB, Westendorp RG, De Craen AJ. Handgrip strength as a predic-tor of functional, psychological and social health. A prospective population-based study among the oldest old. Age Ageing 2010; 39:331-7.
5. Cheung C-L, Tan KCB, Bow CH, Soong CSS, Loong CHN, Kung AW-C. Low handgrip strength is a pre-dictor of osteoporotic fractures: cross-sectional and prospective evidence from the Hong Kong Os-teoporosis Study. Age (Dordr) 2012; 34:1239-48. 6. Syddall H, Cooper C, Martin F, Briggs R, Aihie Sayer
A. Is grip strength a useful single marker of frailty? Age Ageing 2003; 32:650-6.
7. Charles LE, Burchfiel CM, Fekedulegn D, Kashon ML, Ross GW, Sanderson WT, et al. Occupational and other risk factors for hand-grip strength: the Honolulu-Asia Aging Study. Occup Environ Med 2006; 63:820-7.
8. Cucinotta D, Frondini C, Paletti P, Reggiani A, Lan-cellotti F, Galletti L. The importance of assessment of nutritional status for the extension of an inde-pendent longevity. Arch Gerontol Geriatr Suppl 2002; 8:123-8.
9. Bragagnolo R, Caporossi FS, Dock-Nascimento DB, Aguilar-Nascimento JE. Handgrip strength and adductor pollicis muscle thickness as predic-tors of postoperative complications after major operations of the gastrointestinal tract. E Spen Eur E J Clin Nutr Metab 2011; 6:e21-6.
10. Kerr A, Syddall HE, Cooper C, Turner GF, Briggs RS, Sayer AA. Does admission grip strength predict length of stay in hospitalised older patients? Age Ageing 2006; 35:82-4.
11. Cheung C-L, Nguyen US, Au E, Tan KCB, Kung AW. Association of handgrip strength with chronic dis-eases and multimorbidity: a cross-sectional study. Age (Dordr) 2013; 35:929-41.
12. Stenholm S, Tiainen K, Rantanen T, Sainio P, He-liövaara M, Impivaara O, et al. Long-term deter-minants of muscle strength decline: prospective evidence from the 22-year mini-Finland follow-up survey. J Am Geriatr Soc 2012; 60:77-85.
13. Oksuzyan A, Maier H, Mcgue M, Vaupel JW, Chris-tensen K. Sex differences in the level and rate of change of physical function and grip strength in the Danish 1905-cohort study. J Aging Health 2010; 22:589-610.
Fitzgerald SJ, Barlow CE, et al. Associations of mus-cle strength and fitness with metabolic syndrome in men. Med Sci Sports Exerc 2004; 36:1301-7. 16. Cetinus E, Buyukbese MA, Uzel M, Ekerbicer H,
Karaoguz A. Hand grip strength in patients with type 2 diabetes mellitus. Diabetes Res Clin Pract 2005; 70:278-86.
17. Sayer AA, Dennison EM, Syddall HE, Gilbody HJ, Phillips DI, Cooper C. Type 2 diabetes, muscle strength, and impaired physical function: the tip of the iceberg? Diabetes Care 2005; 28:2541-2. 18. Park SW, Goodpaster BH, Strotmeyer ES, Kuller
LH, Broudeau R, Kammerer C, et al. Accelerated loss of skeletal muscle strength in older adults with type 2 diabetes: the health, aging, and body com-position study. Diabetes Care 2007; 30:1507-12. 19. Silventoinen K, Magnusson PK, Tynelius P, Batty
GD, Rasmussen F. Association of body size and muscle strength with incidence of coronary heart disease and cerebrovascular diseases: a popula-tion-based cohort study of one million Swedish men. Int J Epidemiol 2009; 38:110-8.
20. Lino MZR, Muniz PT, Siqueira KS. Prevalência e fatores associados ao excesso de peso em adul-tos: inquérito populacional em Rio Branco, Acre, Brasil, 2007-2008. Cad Saúde Pública 2011; 27: 797-810.
21. Fess EE. Documentation: essential elements of an upper extremity assessment battery. In: Hunter JM, Mackin, EJ, Callahan AD, editors. Rehabilita-tion of the hand and upper extremity. 5th Ed. Saint Louis: Mosby; 2002. p. 263-84.
22. World Health Organization. Global recommenda-tions on physical activity for health. Geneva: WHO Press; 2010.
23. World Health Organization. Obesity: preventing and managing the global epidemic. Geneva: World Health Organization; 2000. (WHO Technical Re-port Series, 894).
24. Schlussel MM, Anjos LA, Vasconcellos MTL, Kac G. Reference values of handgrip dynamometry of healthy adults: a population-based study. Clin Nutr 2008; 27:601-7.
25. Xavier HT, Izar MC, Faria Neto JR, Assad MH, Ro-cha VZ, Sposito AC, et al. V diretriz brasileira de dislipidemias e prevenção da aterosclerose. Arq Bras Cardiol 2013; 101 Suppl 1:1-22.
26. Calabro P, Yeh ET. Intra-abdominal adiposity, in-flammation, and cardiovascular risk: new insight into global cardiometabolic risk. Curr Hypertens Rep 2008; 10:32-8.
27. Schaap LA, Pluijm SM, Deeg DJ, Visser M. Inflam-matory markers and loss of muscle mass (sarcope-nia) and strength. Am J Med 2006; 119:526.e9-17. 28. Visser M, Pahor M, Taaffe DR, Goodpaster BH,
Si-monsick EM, Newman AB, et al. Relationship of interleukin-6 and tumor necrosis factor-alpha with muscle mass and muscle strength in elderly men and women: the Health ABC Study. J Gerontol A Biol Sci Med Sci 2002; 57:M326-32.
TE; MacArthur Studies of Successful Aging. The as-sociations between physical activity and inflam-matory markers in high-functioning older per-sons: MacArthur Studies of Successful Aging. J Am Geriatr Soc 2003; 51:1125-30.
30. Stenholm S, Maggio M, Lauretani F, Bandinelli S, Ceda GP, Di Iorio A, et al. Anabolic and catabolic biomarkers as predictors of muscle strength de-cline: the InCHIANTI study. Rejuvenation Res 2010; 13:3-11.
31. Howard C, Ferrucci L, Sun K, Fried LP, Walston J, Varadhan R, et al. Oxidative protein damage is associated with poor grip strength among older women living in the community. J Appl Physiol (1985) 2007; 103:17-20.
32. Leite LEA, Resende TL, Nogueira GM, Cruz IBM, Schneider RH, Gottlieb MGV. Envelhecimento, estresse oxidativo e sarcopenia: uma abordagem sistêmica. Rev Bras Geriatr Gerontol 2012; 15: 365-80.
33. Wander PL, Boyko EJ, Leonetti DL, McNeely MJ, Kahn SE, Fujimoto WY. Greater hand-grip strength predicts a lower risk of developing type 2 diabetes over 10 years in leaner Japanese Americans. Dia-betes Res Clin Pract 2011; 92:261-4.
34. Helander I, Westerblad H, Katz A. Effects of glu-cose on contractile function, [Ca2+]i, and glycogen in isolated mouse skeletal muscle. Am J Physiol Cell Physiol 2002; 282:C1306-12.
35. Yoon JH, So WY. Associations of hypertension sta-tus with physical fitness variables in korean wom-en. Iran J Public Health 2013; 42:673-80.
36. Cavazzotto TG, Tratis L, Ferreira SA, Fernandes RA, Queiroga MR. Muscular static strength test perfor-mance: comparison between normotensive and hypertensive workers. Rev Assoc Med Bras 2012; 58:574-9.
37. Churilla JR, Magyari PM, Ford ES, Fitzhugh EC, Johnson TM. Muscular strengthening activity pat-terns and metabolic health risk among US adults. J Diabetes 2012; 4:77-84.
38. Cook MD, Heffernan KS, Ranadive S, Woods JA, Fernhall B. Effect of resistance training on bio-markers of vascular function and oxidative stress in young African-American and Caucasian men. J Hum Hypertens 2013; 27:388-92.
39. Artero EG, Lee DC, Ruiz JR, Sui X, Ortega FB, Church TS, et al. A prospective study of muscular strength and all-cause mortality in men with hy-pertension. J Am Coll Cardiol 2011; 57:1831-7. 40. Swain DP, Franklin BA. Comparison of
cardiopro-tective benefits of vigorous versus moderate inten-sity aerobic exercise. Am J Cardiol 2006; 97:141-7. 41. Barbosa AR, Souza JMP, Lebrão ML, Laurenti R,
Marucci MFN. Functional limitations of Brazilian elderly by age and gender differences: data from SABE Survey. Cad Saúde Pública 2005; 21:1177-85. 42. Theme Filha MM, Szwarcwald CL, Souza Junior
PRB. Medidas de morbidade referida e inter-rela-ções com dimensões de saúde. Rev Saúde Pública 2008; 42:73-81.
Submitted on 15/May/2014