w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Molecular
typing
of
human
platelet
antigens
in
immune
thrombocytopenia
patients
in
northern
Brazil
Julia
Cavalcante
do
Carmo
a,
Prissyla
de
Souza
Klippel
a,
Sabrine
da
Costa
Cordeiro
b,
Ângela
Maria
dos
Santos
Fernandes
b,
Raquel
Medeiros
Pinto
a,
Simone
Schneider
Weber
c,d,∗,
Cleiton
Fantin
aaUniversidadedoEstadodoAmazonas(UEA),Manaus,AM,Brazil
bFundac¸ãodeHematologiaeHemoterapiadoAmazonas(Hemoam),Manaus,AM,Brazil
cUniversidadeFederaldoAmazonas(UFAM),Itacoatiara,AM,Brazil
dUniversidadeFederaldoMatoGrossodoSul(UFMS),CampoGrande,MS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received26October2016 Accepted5January2017 Availableonline22February2017
Keywords:
Immunethrombocytopenia Platelets
BeadCheaptechnology Genotyping
HPA
a
b
s
t
r
a
c
t
Background:Immunethrombocytopeniaisanimmunediseasecharacterizedby thrombocy-topeniaandbleedingduetoplateletantibodiesagainstplateletmembraneglycoproteins. Humanplateletantigensarederivedfrompolymorphismsoftheseglycoproteins.Theaim ofthisstudywastoinvestigatehumanplateletantigenfrequenciesinimmune thrombocy-topeniapatientsfromthestateofAmazonas,Brazilandinvestigatethepotentialassociation betweenspecificantigensandriskforimmunethrombocytopenia.
Method:HumanplateletantigentypingwasperformedbyBeadChiptechnologyto deter-mineallelicvariantsof11systems(HPA-1toHPA-9,HPA-11andHPA-15).Thirty-sixpatients (8maleand28female)withamedianageof34years(range:9–69years)wereevaluatedand comparedwithdatafromAmazonasblooddonors.
Results:Plateletcountsvariedfrom3to98×109/L.Theallelefrequencieswere0.944for
HPA-1a,0.056forHPA-1b,0.847forHPA-2a,0.153forHPA-2b,0.555forHPA-3a,0.444forHPA-3b, 0.805forHPA-5a,0.222forHPA-5b,0.9975forHPA-9a,0.025forHPA-9b,0.486forHPA-15aand 0.513forHPA-15b.Amongimmunethrombocytopeniaindividuals,noballeleoftheHPA-4, -6,-7,-8and-11werefound.
Conclusions:The results suggest HPA-1a, HPA-3b and HPA-5b are immune thrombocytopenia-specificautoepitopes.
©2017Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthorat:CentrodeCiênciasBiológicasedaSaúde.UniversidadeFederaldoMatoGrossodoSul,CidadeUniversitária
S/N,CaixaPostal549,79070-900CampoGrande,MS,Brazil. E-mailaddress:[email protected](S.S.Weber).
http://dx.doi.org/10.1016/j.bjhh.2017.01.003
Introduction
Immune thrombocytopenia (ITP) is an immune-mediated acquired disease characterized by transient or persistent decreaseaffectingplateletnumbersand,dependinguponthe degreeofthrombocytopenia,increasedriskofbleeding,1due
tothepresenceofplateletautoantibodies.Plateletmembrane glycoproteins(GPs)appeartobethe principalbindingsites ofITPserumantibodies.2Thepolymorphismsofthehuman
plateletalloantigensoccurduetosinglenucleotide substitut-ionsthatresultinthesubstationofanaminoacid.3
The Immuno Polymorphism Database (IPD) of human plateletalloantigens(HPA)lists35plateletalloantigens,which are located in GPs (platelet receptors).4 The three major
platelet receptorsare GPIIb-IIIa,GPIb-IX-V and GPIa-IIa.3,5,6
GPIIb/IIIais the mostpolymorphic complex and carries19 antigens5:HPA-1(176T>C);HPA-3(2621T>G);HPA-4(506G>A);
HPA-6 (1544G>A); HPA-7w (1297C>G); HPA-8w (1984C>T); HPA-9w(2602G>A); HPA-10w(263G>A); HPA-11w(1976G>A); HPA-14w (19091911delAAG); HPA-16w (497C>T); HPA-17w
(662C>T); HPA-19 (487A>C); HPA-20w (1949C>T); HPA-21w
(1960G>A);HPA-22w(584A>C);HPA-23w(1942C>T);HPA-24w
(1508G>A)andHPA-26w(1818G>T).ThevonWillebrandfactor (vWF)receptorGPIb/IXcarriestwoantigensHPA-2(482C>T) and HPA-12w (119G>A). In addition, the GPIa/IIa complex carriesthe HPA-5(1600G>A), HPA-13w (2483C>T), HPA-18w (2235G>T)and HPA-25w(3347C>T) polymorphic systems.7,8
Moreover,theHPA-15(Gov)polymorphism islocatedinthe CD109moleculeand itsalleles differatasinglenucleotide polymorphism(C2108A)thatcausesaTyr682Seraminoacid substitution.9,10 Thesepolymorphismscanberecognizedas
alloantigens or autoantigens and trigger the clearance of opsonized platelets by phagocytes in the reticuloendothe-lial system or inhibition of platelet production.11 Several
groupsworldwidehavetriedtoestablishapossibleassociation betweenHPApolymorphismsandITP.12–15SomeITP-specific
autoepitopeshavebeensuggested,suchasHPA-2ainGerman patientswithchronicrefractoryITP14andHPA-2bin
Macedo-nianpatientswithITP.15Inaddition,Castroetal.,12suggested
thepresenceofHPA-5binBrazilianpatientswithincreased riskforacuteITP,whilethe HPA-5ahasbeenimplicatedin Koreanpatients.13However,theresultshavebeenunclear,and
studiesexploringthesehypothesesarestilllacking.
Theaimofthis studywastoanalyzethefrequenciesof humanplateletantigens,groupedas11biallelicHPAsystems (HPA-1toHPA-9,HPA-11andHPA-15)inpatientsfrom Ama-zonasStatewithprimaryITP,andtoinvestigatethepotential associationbetweenspecificHPApolymorphismsandriskfor ITP.
Methods
Studysite
TheFundac¸ãoHospitalardeHematologiaeHemoterapiado Amazonas(HEMOAM)isareferral centerforthe diagnosis, treatmentandmonitoring ofhematological diseasesinthe northernregionofBrazil.Theservicereceivesapproximately
100newcasesofITPannually.Thisstudywasapprovedbythe institution’sEthicsCommittee(CEP/HEMOAM#803.634/2014).
Sampledefinitions
In total, 36 unrelated sequential ITP patients treated in HEMOAMparticipatedinthestudybetweenOctober2014and April2015.Informedconsentwasobtainedfromallenrolled patients.AllpatientsinthisstudyhadchronicprimaryITP, whichbydefinitionmeantthediseaselastedformorethan12 monthsaftertheinitialtreatment.Thecriterionforprimary ITPwasthepresenceofisolatedthrombocytopenia (periph-eralbloodplateletcount<100×109/L)intheabsenceofother
causes or disordersthat mightbeassociatedwiththis low plateletcount,inaccordancewiththestandardizationofITP diagnosisestablishedbyaninternationalITPworkinggroup.16
Thus,thediagnosisofprimaryITPwasachievedbyexclusion. The sampledefinitionfor HPAgenotyping ofblood donors excludedsampleswithplateletcountslessthan150×109/L.
GenomicDNAextraction
GenomicDNAsampleswereobtainedfromEDTA-preserved wholebloodusingtheQIAampDNABloodkit(Qiagen,Hilden, Germany)accordingtothemanufacturer’sinstructions.The automatedepMotion5075system(Eppendorf,Hamburg, Ger-many) was adapted. The DNA concentration and quality wereevaluatedspectrophotometricallyusingNanoDrop tech-nology (ThermoFisherScientific,Massachusetts,USA).The sampleswerestoredat−80◦Cuntiluse.
PlateletgenotypingbyBeadChipmicroarraytechnology
Platelet genotyping was performed using a BeadChip assay.17,18 The BeadChip microarray method is capable of
determining 22 allelic variants of 11 HPA systems (HPA-1 toHPA-9,HPA-11andHPA-15).DNAamplificationand post-polymerase chainreaction stepswere performedaccording tothemanufacturer’sinstructions.TheBeadChipslideswere analyzedinafluorescentsystemusingtheBioarraySolutions software(Immucor,Warren,NJ)intheHEMOAMgenomic lab-oratory.
Statisticalanalysis
Thegenotypeandallelefrequencieswereestimatedbydirect counting,andtheresultswerecomparedindividuallywiththe valuespublished forhealthyindividuals from Amazonas.19
The 95% confidence interval (CI), chi square (X2) test or
Fisher’s exacttestwere usedforcomparativeanalysis.The Hardy–WeinbergequilibriumofHPA systemgenotypes was evaluated using the Hardy–Weinberg calculator.20 p-Values
lower than0.05wereconsideredsignificantinallstatistical analyses.
Results
Table1–Clinicaldataandcomparativeanalysisofallelefrequenciesbetweenimmunethrombocytopenia(ITP)patients andblooddonorsinthestateofAmazonas.
Clinicaldata ITPpatients Blooddonorsb
n◦patients 36 200
Gender(male:famale) 8:28 140:60
Age(years) 34(9–69) 36(19–65)
Plateletcount–×109/L 41.5(3–98)a >150c
System a b a b p-valued
HPA-1 0.944 0.056 0.86 0.137 <0.0001
HPA-2 0.847 0.153 0.852 0.147 0.754
HPA-3 0.555 0.444 0.665 0.335 <0.0001
HPA-4 1.00 0.00 0.995 0.005 <0.0001
HPA-5 0.805 0.222 0.892 0.107 <0.0001
HPA-6 1.00 0.00 1.00 0.00 –
HPA-7 1.00 0.00 1.00 0.00 –
HPA-8 1.00 0.00 1.00 0.00 –
HPA-9 0.997 0.025 0.997 0.005 –
HPA-11 1.00 0.00 1.00 0.00 –
HPA-15 0.486 0.513 0.502 0.497 0.502
a Plateletcountatdiagnosis.
b ControlincludesblooddonorsamplespublishedbyPortelaetal.19
c Plateletcountsgreaterthan150 ×109/L.
dChi-squarewithYates’correctioncalculatedFisher’sexactp-valueforcomparisonsofallelefrequenciesbetweenITPpatientsandAmazonas
blooddonors.
Table2–GenotypeandallelefrequenciesforHPA-1toHPA-9,HPA-11andHPA-15inchronicimmunethrombocytopenia patientsfromthestateofAmazonas.
GP SNP Genotypefrequency Allelefrequency p-valueHardy-Weinberg
AA AB BB a b
HPA-1 GPIIIa T176C 0.888 0.111 0.00 0.944 0.056 0.724
HPA-2 GPIIa T482C 0.694 0.305 0.00 0.847 0.153 0.279
HPA-3 GPIIb T2621G 0.305 0.5 0.194 0.555 0.444 0.940
HPA-4 GPIIIa G506A 1.00 0.00 0.00 1.0 0.00 –
HPA-5 GPIa G1600G 0.611 0.388 0.027 0.805 0.222 0.479
HPA-6 GPIIIa G1544A 1.00 0.00 0.00 1.0 0.00 –
HPA-7 GPIIIa C1297G 1.00 0.00 0.00 1.0 0.00 –
HPA-8 GPIIIa C1984T 1.00 0.00 0.00 1.0 0.00 –
HPA-9 GPIIb G2602A 0.995 0.005 0.00 0.9975 0.025 0.97
HPA-11 GPIIIa G1976A 1.00 0.00 0.00 1.0 0.00 –
HPA-15 CD109 C2108A 0.166 0.638 0.194 0.486 0.513 0.094
GP:glycoprotein;SNP:singlenucleotidepolymorphism.
ITP patients and comparative analysis are summarized in Table1.Thestudysamplewascomprisedofeight(22%)male and28(78%)femaleindividuals.Theparticipants’agesranged from9to69years(meanage:34years)andtheplateletcount atdiagnosisvariedfrom3to98×109/L(median:41.5×109/L).
Thediseaseseverityrangedbetweenmildormoderatewhen correlatedwiththedegreeofthrombocytopenia.Thegenotype and allelefrequenciesand p-valuesofthe Hardy–Weinberg testofsamplesemployedinthisstudyareshowninTable2. Theallelefrequencieswere0.944forHPA-1a,0.056forHPA-1b, 0.847forHPA-2a,0.153forHPA-2b,0.555forHPA-3a,0.444for HPA-3b,0.805forHPA-5a,0.222forHPA-5b,0.9975forHPA-9a, 0.025forHPA-9b,0.486forHPA-15aand0.513forHPA-15b.Of theITPindividuals,noballelewasidentifiedforHPA-4, HPA-6,HPA-7,HPA-8andHPA-11.AmongtheseITPindividuals,the
allelefrequenciesoftheHPAsystemwereconsistentwiththe Hard-Weinbergequilibrium.
In the comparative analysis, the allele frequencies for HPA-2(p-value=0.754)and HPA-15 systems(p-value=0.502) were not significantly different between analyzed groups (ITP patients and healthy individuals). On the other hand, the ITP Group had higher incidences of HPA-1a (0.944), HPA-3b and HPA-5balleles when comparedto the Control Group.
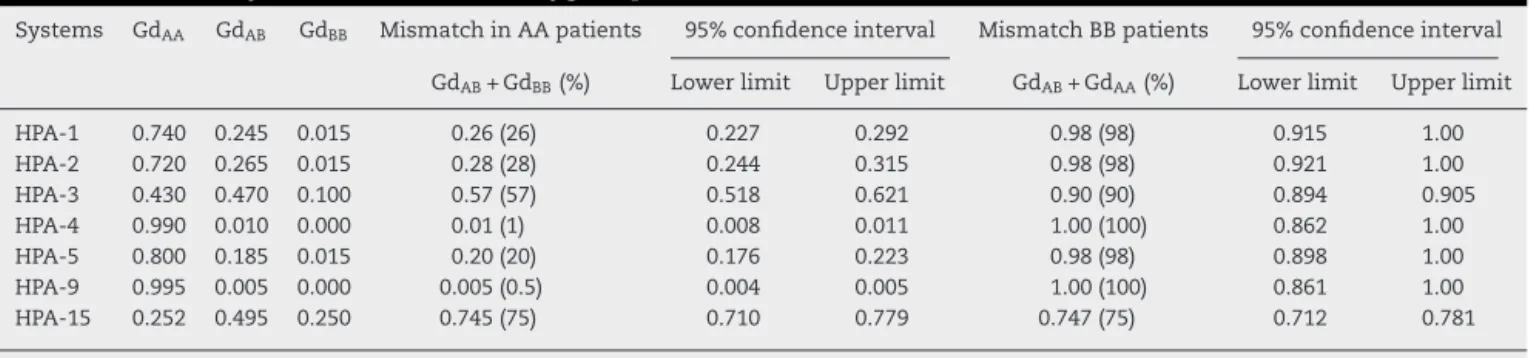
Table3–Probabilityofmismatchinhomozygouspatients.
Systems GdAA GdAB GdBB MismatchinAApatients 95%confidenceinterval MismatchBBpatients 95%confidenceinterval
GdAB+GdBB(%) Lowerlimit Upperlimit GdAB+GdAA(%) Lowerlimit Upperlimit
HPA-1 0.740 0.245 0.015 0.26(26) 0.227 0.292 0.98(98) 0.915 1.00
HPA-2 0.720 0.265 0.015 0.28(28) 0.244 0.315 0.98(98) 0.921 1.00
HPA-3 0.430 0.470 0.100 0.57(57) 0.518 0.621 0.90(90) 0.894 0.905
HPA-4 0.990 0.010 0.000 0.01(1) 0.008 0.011 1.00(100) 0.862 1.00
HPA-5 0.800 0.185 0.015 0.20(20) 0.176 0.223 0.98(98) 0.898 1.00
HPA-9 0.995 0.005 0.000 0.005(0.5) 0.004 0.005 1.00(100) 0.861 1.00
HPA-15 0.252 0.495 0.250 0.745(75) 0.710 0.779 0.747(75) 0.712 0.781
Gd:genotypeofAmazonasblooddonor.
Discussion
Studies have demonstrated relevant associations between GPpolymorphismsandimmune-mediatedplateletdisorders. TheHPAallelefrequencieswerecomparedin36chronicITP patientswithpublisheddataof200healthyindividualsfrom Amazonas.19 TheITPgrouppresentedhigherincidencesof
theHPA-1a,HPA-3bandHPA-5balleles,whichcouldsuggest anassociationofthesealleleswithITPinthispopulation.In addition,Castroetal.12suggestedthatthepresenceofHPA-5b
mightbeassociatedtoincreasedriskforacuteITPinBrazilian patients.Ontheotherhand,Thudeetal.15showedthatallele
frequenciesof the HPA-1, HPA-3and HPA-5 were identical between patients with refractory autoimmune thrombocy-topeniaandblooddonorsintheGermanpopulation.While, the HPA-2b was relatedto a higherrisk forchronic ITP in Macedonianpatients.14Therefore,wesupposethatthe
diver-sityintheprevalenceofautoepitopesamongITPindividuals worldwideoccursinresponsetogeneticinheritanceofHPA polymorphisms.
Thereisevidenceofclinicalcorrelationsbetween autoanti-bodiesagainstextracellularGPepitopesandtheirpathogenic roleinITP.13 ITPTcells recognizeepitopesgeneratedfrom
GPIIb/IIIaand probablyother platelet proteins.21 Thus, the
immunepotentialsofHPA-1,HPA-3andHPA-5allelesarevery important,forexample,GPIIb/IIIa,carryingHPA-1andHPA-3 antigens,isthemostabundantcomplex(50,000–80,000copies per platelet).While,despite the lowabundance ofGPIa/IIa on the platelet membrane (800–2000 copies per platelet), HPA-5hasbeenconsideredanimportantimmunogenic fac-torlinked toimmune syndromes inCaucasians22 and has
beenassociatedwithhighpredictedriskofinducing alloim-munizationintheAmazonaspopulation.19Ghevaertetal.22
demonstratedthat,mostanti-plateletantibodies(95%)have specificityagainstHPA-1aorHPA-5b,whileonly5%are spe-cifictotheothersystems,suchasHPA-2,HPA-3andHPA-15. However,thepathogenesisofITPisclearlyheterogeneousdue totheracialadmixtureamongBrazilianindividuals,a condi-tionthatcanaffectthesefindings.Antibodyspecificitywas notevaluatedinthisstudy,makingitimpossibletospeculate aboutthispotentialassociation.
Plateletmembraneglycoproteinsappeartobean impor-tantbindingsiteforITPserumantibodies.Thisstudyanalyzed 36patientswithITPfromAmazonas,anddescribedspecific HPAantigensrelatedtotheoccurrenceofITP.However,the
relationshipbetweenimmunizationanditspotentialclinical consequencesisnotstraightforward.Hence,thefindingsof thisstudyrepresentjustanattempttoamplifytheknowledge aboutHPAandITPandsuggestapotentialassociationasa riskfactorforthedevelopmentofITP.
Finally, studies have discussed the feasibility of apply-ing molecular typingin theroutine ofhospitaltransfusion services.23,24 Some authors have reported a correlation
betweenthepreventionofnewlydevelopedalloantibodiesin previouslyimmunizedpatientsandreductionsintransfusion rates. Thus, a simulation ofplatelet transfusion mismatch wasperformedconsideringtheHPAgenotypefrequenciesof Amazonasblooddonors.19Theresultssuggestahigherriskof
alloimmunizationinhomozygousBBpatients,duetothehigh frequencyofAAandAB genotypesintheAmazonasblood donorregistry.Therefore,whentransfusionsarenecessaryin previouslyimmunizedpatients,afuturestrategycouldinvolve therecruitmentofhomozygousBBdonorsbyHPAmolecular typing.
Funding
PSK and SCC were recipients of scholarship provided by Fundac¸ão de Amparo à Pesquisa do Estado do Ama-zonas (PAIC/HEMOAM/FAPEAM 2015/2016) and RMP (POS-GRAD/2015/UEA).
Authorship
JCC, PSK,RMP and SCC participated actively in all experi-mentsanddraftedthemanuscript.CFandAMSFhelpedwith dataanalysisandmanuscriptwriting andprovided sugges-tionsduringthecourseoftheexperiments.SSWdesignedthe experiments,providedguidanceduringallpartsofthework, includingthepreparationofthemanuscript.
Conflicts
of
interest
Acknowledgements
The authors wish to thank the Ministério da Saúde and Fundac¸ão de Hematologia e Hemoterapia do Amazonas (HEMOAM)forfinancialandstructuralsupport.Specialthanks toErichdePaula(PVSscholarshipprovidedbyFAPEAM),fora verycarefulreviewofthismanuscriptandgreatsuggestions. All authors read and approved the final version of the manuscript.
r
e
f
e
r
e
n
c
e
s
1. CooperN,BusselJ.Thepathogenesisofimmune
thrombocytopenicpurpua.BrJHematol.2006;133(4):364–74.
2. HeR,ReidDM,JonesCE,ShulmanNR.Extracellularepitopes ofplateletsglycoproteinIbareactivewithserumantibodies frompatientswithchronicidiopathicthrombocytopenia purpura.Blood.1995;86(10):3789–96.
3. RozmanP.Plateletantigens.Theroleofhumanplatelet alloantigens(HPA)inbloodtransfusionandtransplantation. TransplImmunol.2002;10(2–3):165–81.
4. ImmunoPolymorphismDatabase[cited26.10.16].Available from:http://www.ebi.ac.uk/ipd/hpa/table1.html.
5. CurtisBR,McFarlandJG.Humanplateletantigens.VoxSang. 2014;106(2):93–102.
6. LymanS,AsterRH,VisentinGP,NewmanPJ.Polymorphismof humanplateletmembraneglycoproteinIIbassociatedwith theBaka/Bakballoantigensystem.Blood.1990;75(12):2343–8.
7. UlrichtsH,VanhoorelbekeK,CauwenberghsS,VauterinS, KrollH,SantosoS,etal.vonWillebrandfactorbutnot alpha-thrombinbindingtoplateletglycoproteinIbalphais influencedbytheHPA-2polymorphism.ArteriosclerThromb VascBiol.2003;23(7):1302–7.
8. UnkelbacK,KalbR,SantosoS,KrollH,Mueller-EckhardtC, KiefelV.GenomicRFLPtypingofhumanplateletalloantigens Zw(PlA),Ko,BakandBr(HPA-1,2,3,5).BrJHaematol. 1995;89(1):169–76.
9. CardoneJD,ChibaAK,Boturao-NetoE,Vieira-FilhoJP,Bordin JO.GenefrequenciesoftheHPA-15(Gov)plateletalloantigen systeminBrazilians.TransfusMed.2004;14:433–7.
10.HwanSM,KimMJ,ChangHE,HongYJ,KimTS,SongEY,etal. HumanplateletantigengenotypingandexpressionofCD109 (humanplateletantigen15)mRNAinvarioushumancell types.BiomedResInt.2013:946403.
11.CinesDB,BlanchetteVS.Immunethrombocytopenicpurpura. NEnglJMed.2002;346(13):995–1008.
12.CastroV,OliveiraGB,OrigaAF,Annichino-BizzacchiJM, ArrudaVR.Thehumanplateletalloantigen5polymorphism asariskforthedevelopmentofacuteidiopathic
thrombocytopeniapurpura.ThrombHaemost. 2000;84(2):360–1.
13.KimB,SongK.Geneticpolymorphismsofhumanplatelet antigen(HPA)inpatientswithimmunethrombocytopenia.In: XVIthCongrSocThromHaemost.Annais.1997.p.254.
14.PavkovicM,StojanovicA,KaranfilskiO,CevreskaL,Spiroski M.Associationofpolymorphismsinhumanplateletantigens withidiopathicthrombocytopenicpurpurainMacedonians. Prilozi.2012;33(1):135–46.
15.ThudeH,GatzkaE,AndersO,BarzD.Allelefrequenciesof humanplateletantigen1,2,3,and5systemsinpatientswith chronicrefractoryautoimmunethrombocytopeniaandin normalpersons.VoxSang.1999;77(3):149–53.
16.RodeghieroF,StasiR,GernsheimerT,MichelM,ProvanD, ArnoldDM,etal.Standardizationofterminology,definitions andoutcomecriteriainimmunethrombocytopenicpurpura ofadultsandchildren:reportfromaninternationalworking group.Blood.2009;113(11):2386–93.
17.ContiF,BertrandG,DezanM,CostaT,AravechiaM,MotaM, etal.MolecularHPAgenotypingbymicroarrayinBrazilian blooddonors.Transfusion.2014;54(2):405–11.
18.EdelmannL,HashmiG,SongY,HanY,KornreichR,Desnick RJ.Cysticfibrosiscarrierscreening:validationofanovel methodusingBeadChiptechnology.GenetMed. 2004;6(5):431–8.
19.PortelaCN,SchrieferA,AlbuquerqueSR,PerdomoRT,Parente AF,WeberSS.Thehumanplateletalloantigenprofileinblood donorsfromAmazonas,Brazil.TransfusMed.
2016;26(6):448–56.
20.KoonecHardy-WeinbergEquilibriumCalculator[cited 26.10.16].Availablefrom:http://www.koonec.com/k-blog/ 2010/06/20/hardy-weinberg-equilibrium-calculator/.
21.SukatiH,WatsonHG,UrbaniakSJ,BarkerRN.Mappinghelper T-cellepitopesonplateletmembraneglycoproteinIIIain chronicautoimmunethrombocytopenicpurpura.Blood. 2007;109(10):4528–38.
22.GhevaertC,CampbellK,WaltonJ,SmithGA,AllenD, WilliamsonLM,etal.Managementandoutcomeof200cases offetomaternalalloimmunethrombocytopenia.Transfusion. 2007;47(5):901–10.
23.SapatnekarS,FigueroaPI.Howdoweusemolecularredblood cellantigentypingtosupplementpretransfusiontesting? Transfusion.2014;54(6):1452–8.