First, the thesis examined the role of multiple adverse childhood experiences in the risk of self-harm. Experience of maternal and paternal adversity in childhood as determinants of self-harm in adolescence and young adulthood.
Definition
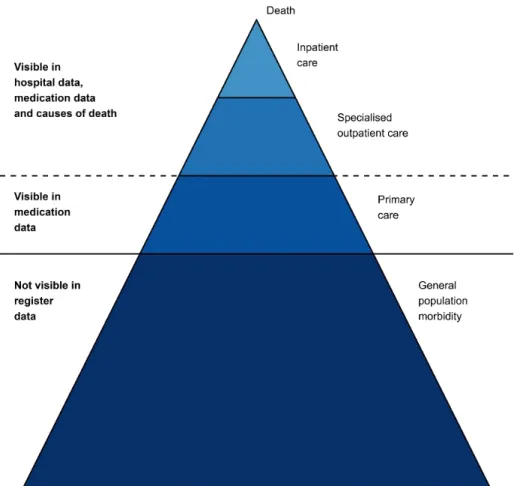
The vast majority of the iceberg, self-harm in the community, is invisible to healthcare. Furthermore, most of the events studied in this task are self-poisoning, as they constitute the majority of self-harm cases treated in hospitals (see e.g. Geulayov et al., 2018).
Epidemiological aspects
The frequency of emergency department presentations due to self-harm in Canada is somewhat similar (Gardner et al., 2019). Research into trends in hospital-presenting self-harm in the Nordic countries is scarce, but a Danish study observed no increases in these trends (Steeg et al., 2020).
Psychiatric disorders
In addition, a history of self-harm has also been associated with an increased risk of developing subsequent psychiatric disorders (Borschmann et al., 2017; Mars et al., 2014). Mental disorders may also act as mechanisms linking other risk factors, such as predisposing psychological vulnerabilities and stressful life events, to self-harm (Hawton, Saunders, et al., 2012; O'Connor & Nock, 2014).
Psychological factors
Regarding these risk factors, psychological research has also assessed the reasons and motives underlying self-harm. While some cases of self-harm are characterized by suicidal intent, there are other motivations and reasons for self-harm.
Adverse childhood experiences
In addition to stress-induced mechanisms, ACEs can also affect a child's mental health through impaired parenting in families facing adversity (Uddin et al., 2020). Furthermore, many of the parental behavioral and psychiatric factors, such as depression (Goodman, 2020; Sawyer et al., 2019) and alcohol abuse (Campbell & Oei, 2010), included in ACE measurements also have a intergenerational component, and thus parts of the association may be related to the transmission of self-harm risk factors across generations.
Risks of risks: Parental socioeconomic resources
Social causation and health selection
These factors are partly heritable and known to be associated with self-injury (Fiori et al., 2014; Turecki & Brent, 2016) and may also play a role in the association between parental SEP and self-injury. An additional source of stress may also stem from social comparison with others (Wetherall et al., 2019).
Effect moderation
There are several mechanisms behind this hypothesis, many of which revolve around elevated levels of stress experienced in lower SEP households (Devenish et al., 2017). The socio-economic differences in healthcare use can be explained by differences in resources, broadly understood (Fjær et al., 2017; Link & Phelan, 1995).
Adverse childhood experiences and self-harm
Previous research
This can be considered a limitation, as experiences of sexual and physical abuse are known to significantly increase the risk of self-harm (Angelakis et al., 2020). These are comparable to estimates from cross-sectional studies (Bruffaerts et al., 2010; Dube et al., 2001).
Identified gaps
Parental socioeconomic resources and self-harm
Previous research
Finally, in a Swedish study, socioeconomic resources were not associated with more severe cases of self-harm presenting to hospital (Lodebo et al., 2017). Receiving social assistance is a similar risk indicator: the risk of self-harm in hospital (E. Björkenstam, Kosidou, et al., 2016) or suicide (Agerbo et al., 2002;.
Identified gaps
The existing evidence for socio-economic differences seems inconclusive (Islam et al., 2020; Michelmore & Hindley, 2012), but there is some support that young adults' own low education can predict non-treatment (Tang et al., 2022) . Given that many of the reported reasons for not seeking help for adolescent mental health problems are resource-related (Radez et al., 2020; Reardon et al., 2017), population-based.
Self-harm among Finnish adolescents and young adults
There is no Finnish statistical database on self-harm in clinical settings, or other self-harm for that matter. Regarding self-harm present at the community level, there is only one study reporting prevalence estimates (Laukkanen et al., 2009).
Mental health care
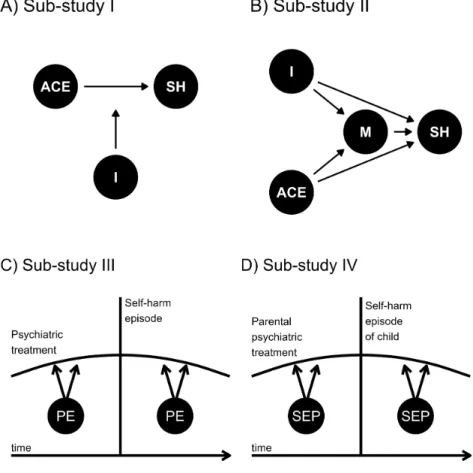
Sub-study I (Figure 1, panel A) examined the associations between adverse childhood experiences related to biological parents and self-harm during adolescence and young adulthood. The moderating effects of parental education (PE) on the temporal trajectory of psychiatric treatment before and after self-harm in adolescents and young adults.

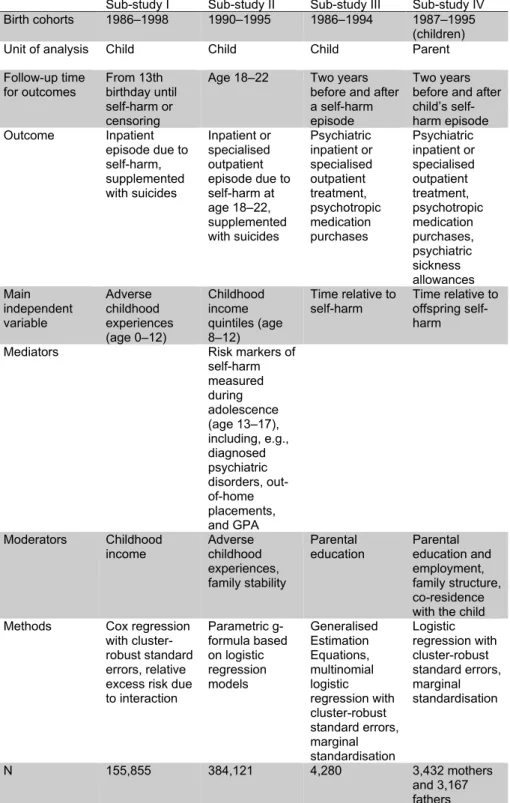
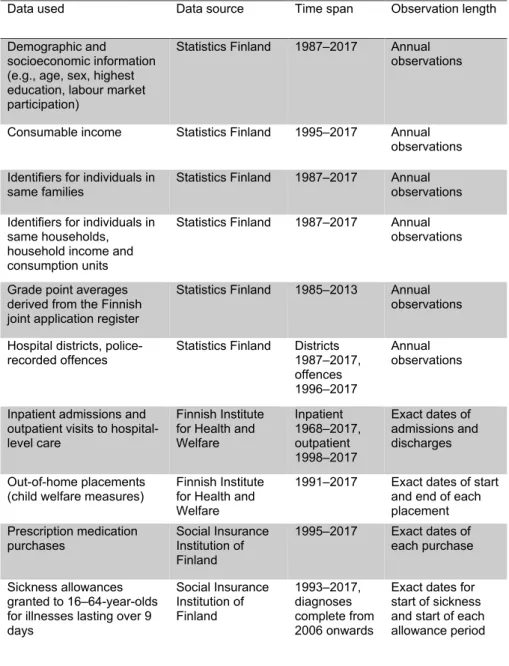
Data
The data sources were the same as in sub-studies II–IV, but hospital data were only available up to 2011 and Statistics Finland data up to 2012, and there were no data on specialized outpatient health care. Income from consumer goods Statistics Finland 1995-2017 Annual observations Identifiers for individuals in the same families Statistics Finland 1987-2017 Annual observations Identifiers for individuals in the same households, household income and consumption units.
Participants and study design
Iceberg of administrative data
Above the surface are all those conditions that have been addressed at various levels of the health care system. Finally, the tip of the iceberg consists of deaths that can be identified with the cause-of-death data of Statistics Finland.
Self-harm
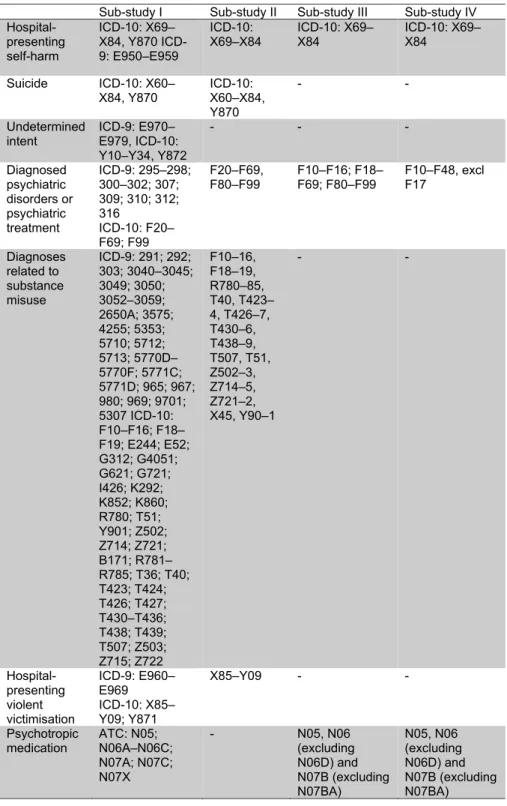
The International Classification of Diseases version 10 (ICD-10) was used to identify episodes of self-harm from registry data. In sub-study I, the outcome also included those hospital episodes where the external cause of injury was defined as the consequences of deliberate self-harm (Y870).
Adverse childhood experiences
Parental substance use admissions in Part I were defined from hospital data in the same way as ICD codes (Table 3). In Part Study II, ACEs were conceptualized as confounders in the association between childhood income and self-injury.
Parental socioeconomic resources
Adolescent risk markers and psychiatric treatment
Additional covariates
In substudy II, a variable measuring family stability was constructed and used as a confounder in the mediation analysis. In sub-study IV, parent and child living arrangements were considered as a covariate and effect modifier.
Statistical methods
Cox regression and interaction analyses
In sub-study III, a binary indicator of being under or over 18 years of age at the time of self-harm was included in the models and age was also used to define the index event. In substudy I, a sensitivity analysis was performed where data were restricted to those who lived with their parents throughout their childhood (ages 0–12 years).
Parametric g-formula
After these three simulations, the mean values of the outcome were stored for each scenario. These effects were calculated after each bootstrap iteration and the average of the 250 bootstrap effect.
Trajectories of treatment and multinomial models
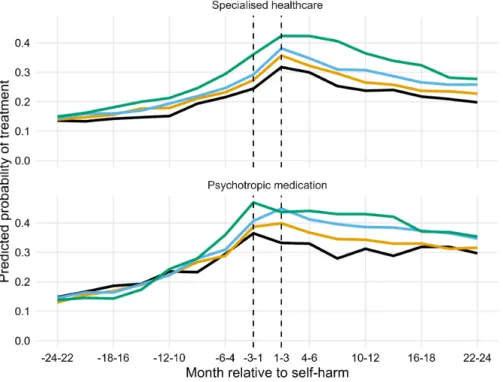
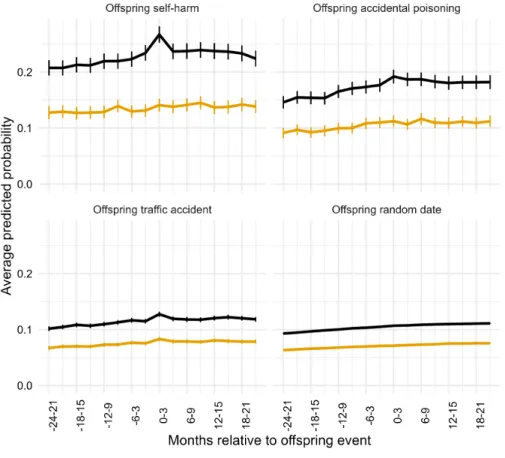
In substudy IV, the entire population mean curve was estimated, and sociodemographic differences according to parents' employment, education, and living conditions with the child were evaluated using interaction analyses. Therefore, in substudy III, cumulative psychiatric treatment at different time points (one month, one year, and two years before and after self-injury) was calculated and hierarchically categorized into inpatient treatment.
Adverse childhood experiences and self-harm
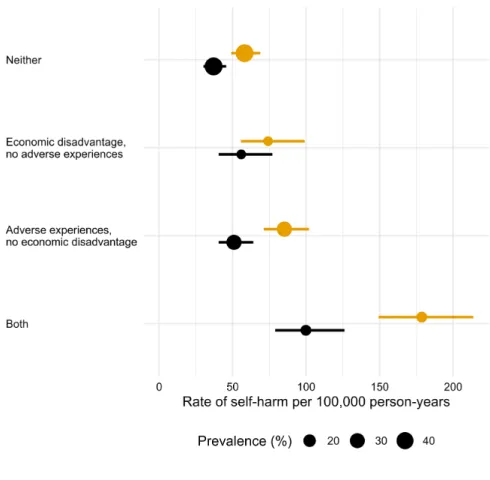
The second aim of the substudy was to examine possible differences in the experience of adverse experiences in low-income households versus. calculated (Figure 6).
Low childhood income and self-harm
Main association
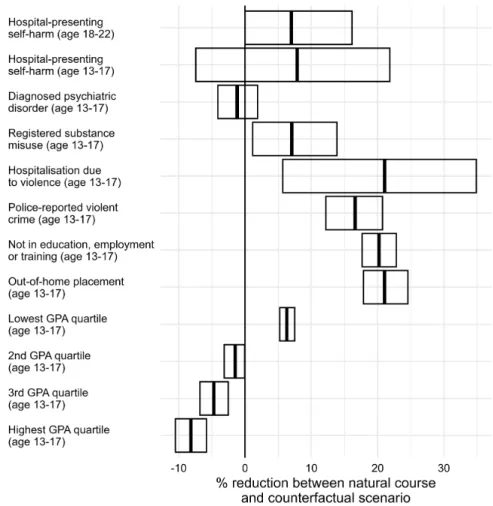
The ATT for the intervention on the main outcome, self-harm aged 18–22, was about 7.0% (95% CI reduction in the prevalence of self-harm between the natural course (NC) and counterfactual (CF) scenarios, i.e. , between the simulated scenario with no intervention in the data and the simulated scenario with an intervention to raise those in the lowest childhood income quintile to the second lowest implemented to the data (Figure 7). These differences appear systematic and the effects of the hypothetical intervention are statistically significant only in the subgroups who are exposed to ACE.
Mediation
Adding the effect of GPA on the TE decreased the percentage mediated from about 75% to about 60-65%. Rows show the percentage mediated after including a specific mediator on the direct effect of income.

Psychiatric treatment before and after self-harm
The probabilities of purchasing psychotropic drugs decreased gradually after self-harm and were 0.30 and 0.35 at the end of follow-up in the lowest and highest parent education groups, respectively. The probability of not using treatment during the two years after self-harm was 0.29 in those in the lowest parental education group, while in the highest parental education group the corresponding.
Parental psychiatric treatment before and after self-harm
Among fathers who were not employed, the odds of treatment varied between 0.25 and 0.29, but no significant changes were observed relative to offspring self-harm. Again, offspring self-injury did not appear to significantly alter these probabilities among fathers.
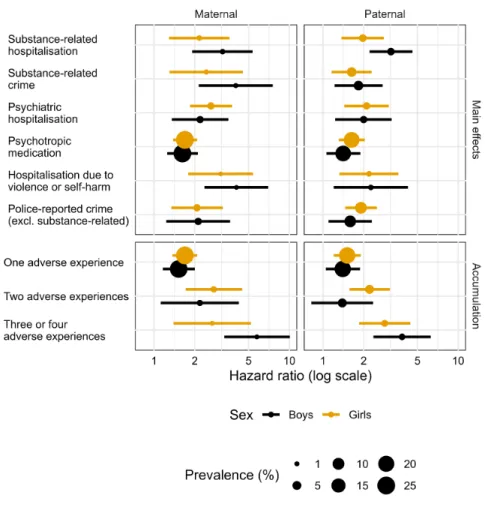
Differences between maternal and paternal adversity
This is also encouraged because of the finding that the effect of experiencing the combination of both maternal and paternal adversity may have more than additive effects on self-harm risk. In addition to differences between maternal and paternal adversity, sub-study I also examined gender differences in the association between ACEs and adolescent self-harm.
Mediators linking childhood income with self-harm
The relative differences in prevalence between children's income groups were also the highest for these risk markers, suggesting that it is low.
Adverse childhood experences and childhood income
However, this differential vulnerability hypothesis derived from previous SLE studies has also been questioned recently as being solely observed due to confounding (Anderson et al., 2021), and it is possible that some of the effect moderation findings in this study also may be subject to this bias, as the study designs did not account for unobserved confounds through the use of e.g. individual or sibling fixed effects. The complex pathways between SEP and ACEs have only recently gained interest (Straatmann et al., 2020; Taylor-Robinson et al., 2018), but there is still much that is not yet understood, including the causal directions in the relationship between ACEs and SEP.
Socioeconomic differences in psychiatric treatment
Moustgaard et al., 2016), but there is no previous evidence on temporal differences in psychiatric treatment use before and after an episode of self-harm presenting in hospital in adolescence and young adulthood. In addition, men may be less likely to seek psychiatric treatment than women (Roberts et al., 2018).
Policy implications
Similar findings have been shown in the previous literature (Moustgaard et al., 2016; Paananen, Ristikari, et al., 2013). Additionally, additional training in medical schools related to meeting individuals with different sociodemographic backgrounds may also be helpful (Verlinde et al., 2012).
Methodological considerations
Hospital self-harm and risk of fatal and non-fatal recurrence: systematic review and meta-analysis. Intentional self-harm and the link between violence, victimization and mental health problems in the United States.