Abnormal clinical renal findings such as proteinuria, hematuria or chronic renal failure (CRF) are commonly seen in patients with RA (Sørensen 1962; Richards et al. 1988; Cantagrel et al. 1990; Koseki et al. 2001), but reports on the incidence of these findings in early RA patients are minor (Koseki et al. 2001).
Abnormal clinical renal findings in patients with RA
Proteinuria
- Prevalence and incidence of proteinuria in RA patients and in the normal population
- Associations of proteinuria in patients with RA
Proteinuria was detected in 10% and persistent proteinuria (≥3 month period) in 7% of these patients (Koseki et al. 2001). Amyloidosis has been the most common renal morphological finding in RA patients with nephrotic syndrome (Helin et al. 1995).
Hematuria
- Prevalence and incidence of hematuria in RA patients and in the normal population
- Associations of hematuria in patients with RA
Also in the general population, a remarkable proportion of microhaematuria has been found to be transient (Froom et al. 1984). No excess mortality has been identified in RA patients with isolated haematuria (Sihvonen et al. 2004).
Chronic renal failure
- Prevalence and incidence of chronic renal failure in RA patients and in the normal
- Associations of chronic renal failure in patients with RA
In an unselected outpatient group of 167 advanced RA patients, serum creatinine exceeded 130 µmol/l in 3% of patients (Richards et al. 1988). Mortality has been found to be within expected limits in RA patients with isolated CRF, whereas CRF associated with other renal findings predicts increased mortality (Sihvonen et al. 2004).

RA-associated renal diseases
Renal AA-amyloidosis
Amyloid deposition in abdominal adipose tissue is seen exclusively in systemic amyloidosis (Libbey et al. 1983). Nevertheless, the survival of patients with AA-amyloidosis has improved in recent decades; Gerz et al.

Mesangial glomerulonephritis (MesGN)
Isolated hematuria in RA patients with MesGN does not appear to be associated with DMARD therapy (Hordon et al. Mortality in RA patients with MesGN has been shown to be within expected limits (Sihvonen et al. 2004).
Other diseases
Renal diseases related to DMARDs and NSAIDs
- Gold salts and D-penicillamine
- Cyclosporine
- Other disease-modifying antirheumatic drugs (DMARDs)
- Non-steroidal anti-inflammatory drugs (NSAIDs)
Renal toxicity of sulfasalazine has not been a concern in the treatment of patients with rheumatoid arthritis (Jones et al. 1991), but nephrotic syndrome, minimal change nephropathy and. However, a beneficial effect of anti-TNF-α agents on proteinuria and renal function has been reported in rheumatoid arthritis patients with renal amyloidosis (Elkayam et al. 2002; Gottenberg et al. 2003).
Measurement of renal function in RA patients
- Chronic kidney disease and glomerular filtration rate
- The significance of estimating glomerular filtration rate in RA patients
- Measurement of exogenous substances
- Plasma creatinine and creatinine clearance
- Creatinine-based prediction equations
- Plasma cystatin C
- Plasma urea
Significant extrarenal elimination of creatinine by bacterial degradation in the gastrointestinal tract can occur in patients with severe CKD (Levey et al. 1988). Serum cystatin C has been shown to decrease hypothyroidism and increase hyperthyroidism (Manetti et al. 2005).
Populations
- Study I
- Study II
- Study III
- Study IV
All met the 1987 American College of Rheumatology criteria for RA (Arnett et al. 1988) and RF was positive in 44 of them. This study population consisted of a cohort of 195 DMARD- and glucocorticoid-naïve patients with recent onset RA (duration of symptoms < 2 years) who participated in the FIN-RACo study from April 1993 to May 1999 (Möttönen et al. 1999). After two years, the choice and dosage of DMARDs and prednisolone was not limited, but treatment was still aimed at achieving or maintaining remission (Korpela et al. 2004; Rantalaiho et al. 2009).
One hundred and seventy-eight patients completed the two-year follow-up, 160 completed the five-year follow-up and 138 attended the 11-year follow-up visit (Rantalaiho et al. 2009).
Methods
- Determination of abnormal clinical findings and renal diseases in the cross-sectional study in
- Assessment of the prognosis of clinical and histologically proven renal disease and new
- Evaluation of the diagnostic accuracy of various methods to estimate GFR in RA patients
- Evaluation of the cumulative incidence of abnormal clinical renal findings and the influence of
- Statistical analyses
If any of the abnormal findings were detected for the first time (since 1988), a renal ultrasound examination was performed. In study III, laboratory determinations were made in connection with a routine follow-up in the outpatient clinic at the Departments of Nephrology or Rheumatology at Tampere University Hospital. In study III, the Pearson correlation coefficient was used for correlation analysis of the measured parameters (plasma cystatin C, creatinine, creatinine clearance, urea and estimated GFR using CG and MDRD formulas) with plasma 51Cr-EDTA clearance.
The comparison of the differences between the obtained correlation coefficients was done by Statistica version 7.0 for Windows using the Difference Tests module.
Ethical considerations
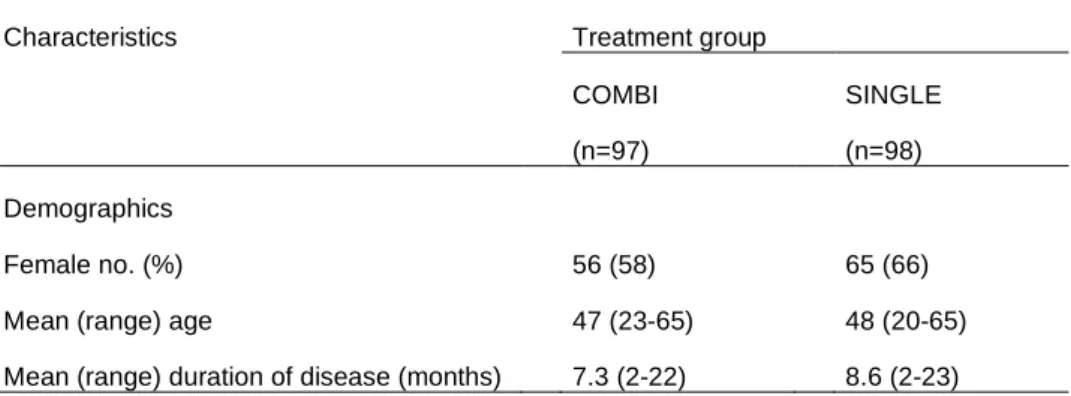
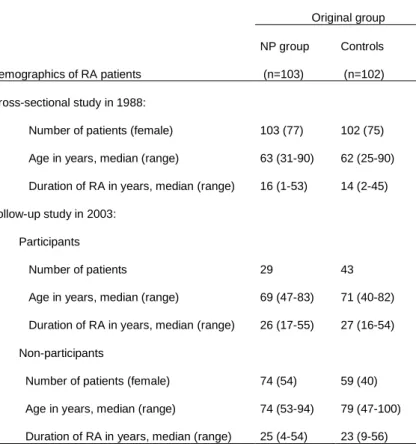
Demographics and details of treatments in the advanced and early RA study populations
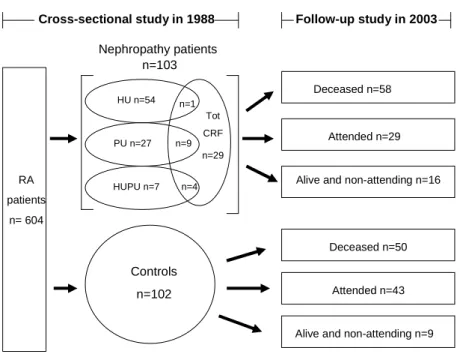
Demographics of patients with rheumatoid arthritis in primary nephropathy (NP) and controls in a cross-sectional study in 1988 and at follow-up in 2003 in Study I. Incidence and persistence of abnormal clinical renal findings in a follow-up study of the population with advanced RA (Study I). CRF in total=chronic renal failure in combination with or without hematuria and/or proteinuria includes patients who also belong to PU, HU, HUPU, CRFisol groups.
Proteinuria
Incidence of proteinuria in advanced RA
Persistence and prognosis of proteinuria in advanced RA
Incidence of proteinuria in early RA
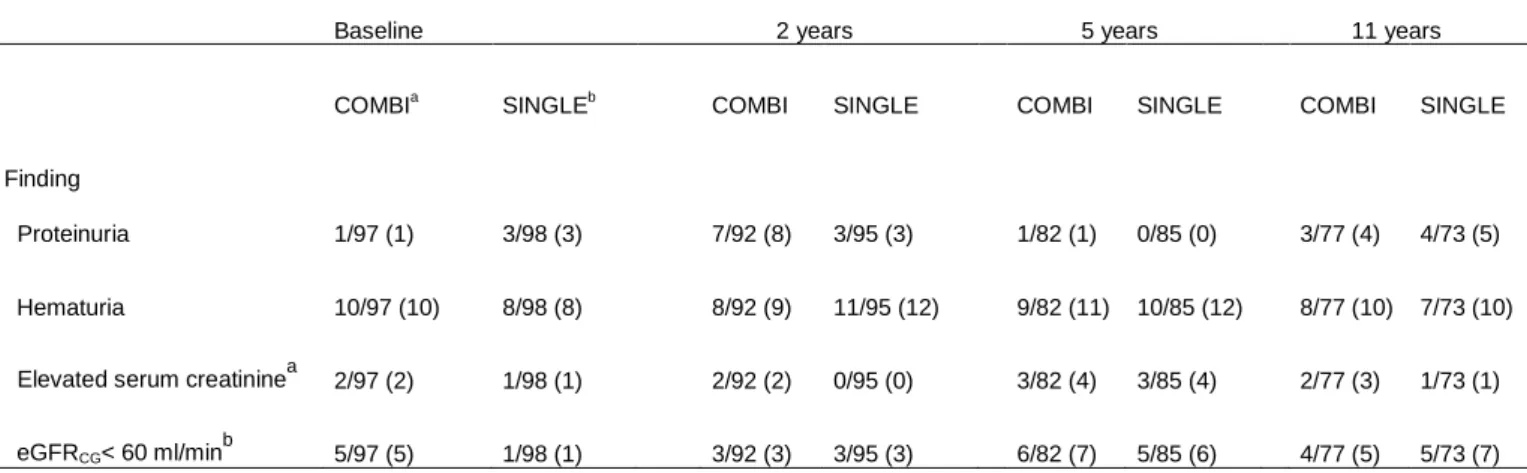
Cross-sectional (time-to-time analysis) prevalence (number of patients, %) of abnormal clinical renal findings among patients attending follow-up visits in study IV.
Hematuria
Incidence of hematuria in advanced RA
Persistence and prognosis of hematuria in advanced RA
Incidence of hematuria in early RA
Chronic renal failure (CRF)
Incidence of chronic renal failure in advanced RA
Persistence and prognosis of chronic renal failure in advanced RA
Incidence of chronic renal failure in early RA
The cross-sectional prevalence of elevated serum creatinine values was 2-4% and for glomerular filtration rates < 60 ml/min 1-7% throughout the study in both groups (Table 6). During the entire follow-up, serum creatinine was elevated in 90 measurements, and the finding was associated with cyclosporine use in three cases. Cumulative Incidence of Repeat Elevated Serum Creatinine Findings in Combination (COMBI) and Single (SINGLE) Treatment Groups (Study IV).
Cumulative incidence of recurrent GFR < 60 mL/min/1.73 m2 estimated by the CG formula (eGFRCG) in the combined (COMBI) and single (SINGLE) treatment groups (Study IV).
Long-term prognosis of renal diseases
Renal AA-amyloidosis
The available tissue samples for the detection of amyloid in the NP group during the cross-sectional study in 1988 through 2003 are shown in Table 7. All but one of the 20 definite or probable renal amyloidosis patients in the NP group had CRF at follow-up. Data on tissue samples obtained to detect amyloid in the NP group in the baseline study in 1988 and in the follow-up in 2003 (study I).
In the 1988 baseline study, tissue samples for detection of amyloid were not obtained systemically from the control group, and thus samples were available for only four of the 102 control RA patients.
Mesangial glomerulonephritis
By 2003, tissue samples were available for 64 patients (63%) at follow-up and 13 of these (20%) showed amyloid deposits on histological examination. There was one patient with histologically confirmed renal amyloidosis and three patients with probable renal amyloidosis. Three of these four patients had isolated CRF (serum creatinine above 200 µmol/l in all) and one patient had isolated proteinuria.
Occurrence of abnormal clinical renal findings in RA patients with mesangial glomerulonephritis (MesGN) at baseline.
Diagnostic accuracy of measurements of renal function in RA patients
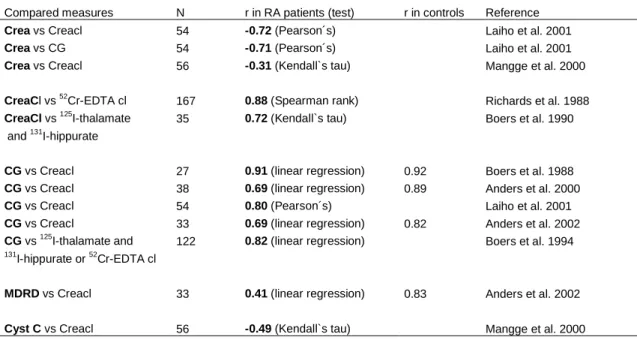
GFRMDRD = GFR estimated by diet change in renal disease formula GFRCG = GFR estimated by Cockcroft-Gault formula. Plasmacystatin C remained within normal range in 29% and 12% of patients with stage 2 (GFR<90ml/min) or stage 3 (GFR<60ml/min) CKD, respectively, while CG and MDRD estimates for GFR and plasma creatinine clearance showed better sensitivity. Pearson correlation coefficients (CC) between the studied markers of GFR and plasma 51Cr-EDTA clearance.
The GFR level estimated by the GC and MDRD formulas appears to be about 20.

Incidence of abnormal clinical renal findings in advanced and early RA
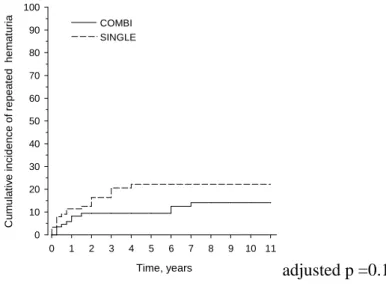
However, the percentage of intermittent findings in the present study was significantly higher than in the last mentioned (Koseki et al. 2001). Persistent proteinuria in early RA patients has been mainly associated with DMARDs (DPA, gold salts, bucillamine) (Koseki et al. 2001), but in the present study only one of the proteinuria findings was significantly associated with DMARD use. nephrotoxic. DPA). In the early RA population (study IV) recurrent hematuria was frequently detected (14-22%), and the cumulative incidence of the first single findings was even double, the results were more or less identical to those in a previous report (Koseki et al. 2001).
In the aforementioned report, all medications used during follow-up were recorded, and most findings of elevated serum creatinine were therapy-related, but only occasionally with DMARD therapy (Koseki et al. 2001).
Prognosis and etiology of abnormal clinical renal findings
The nonspecific and transient nature of neurologic isolated hematuria may partially contribute to the good prognosis of the finding observed in this study. The prevalence of definite or probable renal amyloidosis in the isolated CKD group was clearly lower than in the complete CKD group, which also included patients with proteinuria and/or hematuria. In the group with complete chronic renal failure, the overall renal prognosis was worse than in isolated patients with chronic renal failure.
Accordingly, in the original population-based cross-sectional study in 1988, isolated chronic deficiency was associated with aging and hypertension, which probably explains the good prognosis at follow-up (Korpela 1993).
Prognosis of renal AA-amyloidosis and mesangial glomerulonephritis
In the present study, the long follow-up period allowed the appearance of clinical signs of amyloidosis in addition to e.g. positive results in subcutaneous biopsy. They considered the prognostic value of positive subcutaneous biopsy questionable because at least 73% of the findings remained subclinical in the average 6 years of follow-up. The poorer prognosis associated with the MesGN occurring with proteinuria was not confirmed in the.
In conclusion, the good clinical prognosis of MesGN in RA patients was confirmed in the current median follow-up of 15 years, as was the poor clinical prognosis of renal amyloidosis, at least in patients treated with traditional DMARDs.
Usefulness of the estimates of GFR in detecting chronic renal failure in RA patients
This is in agreement with a previous report on the good performance of the CG formula in RA patients with a correlation coefficient of 0.82 between the formula and directly measured GFR (Boers et al. 1994). The CG formula and also the MDRD formula overestimated GFR by about 20%, which is in agreement with a previous report comparing CG with creatinine clearance (Boers et al. 1988). Only one previous study has been conducted in RA patients (Mangge et al. 2000), and it found that plasma cystatin C is better at detecting early renal failure than plasma creatinine.
Estimation of GFR by serum creatinine or creatinine clearance is influenced by changes in muscle mass, diet, physical activity and inflammatory processes (Perrone et al. 1992).
Limitations of the study and future directions
However, according to a recent paper (Karie et al. 2008), as many as half of RA patients studied did not have adequate methotrexate dose adjustment based on their level of renal function. A limitation of Study IV was that estimates of the occurrence of proteinuria and hematuria were based on dipstick urinalysis. Second, detailed information on the use of individual DMARDs was not analyzed, but the association of the use of individual nephrotoxic DMARDs (DPA, gold salts, and cyclosporine) with cases of proteinuria and impaired renal function was identified.
However, the finding does not preclude the need for regular monitoring for changes in urinalysis and kidney function in RA patients in general.
Clinical implications of the study
Boers M, Dijkmans BA, Breedveld FC, and Mattie H (1988): Errors in the prediction of creatinine clearance in patients with rheumatoid arthritis. Laiho K, Kaarela K, Kautianen H, and Kauppi M (2001): Evaluation of renal function in patients with rheumatoid arthritis and amyloidosis. Cyclosporine in common clinical practice: an estimate of the benefit-risk balance in patients with rheumatoid arthritis.
Sørensen AWS (1964): Renal function in patients with rheumatoid arthritis in relation to disease onset. Background/Purpose: There is little knowledge about the usefulness of cystatin C measurement in the detection of chronic kidney disease in patients with rheumatoid arthritis (RA). Boers M, Dijkmans BAC, Breedveld FC: Prediction of glomerular filtration rate in patients with rheumatoid arthritis: satisfactory performance of the Cockcroft formula.