Army to date, robotic surgery has developed significantly and found applications in many medical specialties. The first automated endoscopic system for optimal positioning (AESOP) marked the launch of robotic surgery revolution in 1994. There are three types of robotic systems: the "passive robot", which is completely controlled by the surgeon, the "semi-active" robot, which requires input from the surgeon to perform force-directed activity and the "active robot", which is programmed to perform an entire procedure and require no surgical intervention. The first two types are the most common in surgery.
For the patient, robotic surgery has many advantages over classic open surgery in many respects. To date, robotic surgery has been used in up to 50 pediatric surgical procedures, primarily abdominal and thoracic. In thoracic surgery, the DaVinci robot was used in 1998 for cardiac bypass. Other thoracic procedures include coronary artery bypass, transplantation, harvesting, and mitral valve repair as well as the ressection of thoracic tumors. The development of endoscopes has greatly facilitated the work of ENT doctors, leading to a reduction in tissue damage, blood loss and transfusion needs, and minimizing hospitalization. The operative time became considerably shorter and the postoperative morbidity also appeared to decrease.
In contrast to other specialties, the use of robotic surgery in otolaryngology was delayed mainly because the console and instruments were best suited for abdominal use. The initial attempt was followed by many more, such as the one in 2005 at the University of Pennsylvania, where a transoral robotic supraglottic partial laryngectomy was performed in a dog model using a da Vinci console. Walter Reed Army Medical Center (Washington DC) has also used canine and porcine models to investigate the feasibility of transoral robotic surgery for upper airway procedures. The canine model has also been used for procedures related to the anterior and midline of the skull base, nasopharynx, clivus, sphenoid,. Previous studies in animal and cadaver models have enlightened head and neck surgeons to the advantages and limitations of robotic surgery.
In addition to TORS, other applications of robotic surgery in otolaryngology, head and neck surgery include robotic-assisted thyroidectomy/parathyroidectomy, robotic-assisted neck surgery, craniomaxillofacial robotic surgery, neurosurgical robotic stereotactic biopsy and intracranial procedures, transsphenoidal skull base surgery using a hexapod robotic system, and robot-assisted functional endoscopic sinus surgery.
2.SPECIAL SECTION
- Objectives – Hypotheses
- Materials - Methods
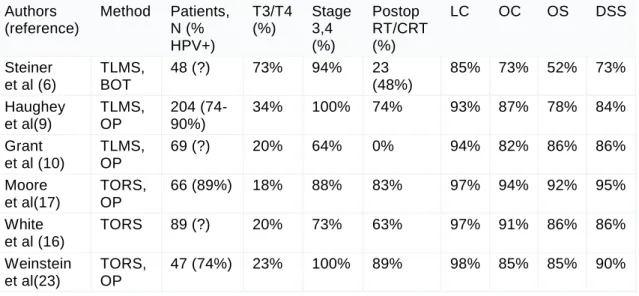
- Results
- Tables Table 1
- Discussion
- Conclusion
With regard to the anatomical area, the study produced the following results: apart from the reviews, most of the studies concerned the pharynx and the oral cavity (35), a large number of publications the larynx and the supraglottic area (17), while some others of the tongue (5), the area of the tonsils (2), the nasopharynx (3), the parapharyngeal space (2), and the base region of the skull (3). The advanced T stage and the overall stage and percentage of the patient series that were HPV+ is shown (if reported). After the successful preliminary data, several attempts were made to apply the method to patients.
These patients with T1 to T4 tumors of the oral cavity, oropharynx, hypopharynx, and larynx all had negative surgical margins after TORS resection. The tumor extended to the base of the tongue in 3 patients, the preepiglottic space in 2 patients and the pyriform sinus in 2 patients. Traditionally, the nasopharynx is considered one of the most challenging anatomical areas for the ENT surgeon.
In 2012, another case report published by the otolaryngology team of the University of Hong Kong verified the feasibility of robotic surgery in the management of nasopharyngeal lesions. The lower part of the resection was performed with a DaVinci surgical robot transorally after splitting the soft palate to expose the nasopharynx. The upper part of the resection, including removal of the anterior wall and floor of the sphenoid, was performed transnasally under endoscopic vision. The tumor was removed en bloc with the sphenoid sinus wall with a clear resection margin.
It is limited medially by the superior pharyngeal constrictor and laterally by the mandibular ramus, deep lobe of the parotid and the medial pterygoid muscle. Regarding the parapharyngeal wall and infratempral fossa, the feasibility of the method was demonstrated in the dog and cadaver model. TORS was also performed in two patients with benign neurogenic tumors of the prestyloid parapharyngeal space (Lee HS, Kim J, Lee HJ, Koh YW, Choi EC).
Surgical visibility was excellent in the two cases, mainly because there was adequate visibility of the lateral aspect of the dissection plan. Both patients were satisfied with the aesthetic result, the absence of complications in postoperative morbidity and the shortened hospital stay (5 to 6 days). The rapid learning curve of the Da Vinci Surgical System can be explained by the intuitive movement of the system.
In 2012, the team from the Department of Otolaryngology-Head and Neck Surgery, Johns Hopkins Hospital, Baltimore, Maryland 21218, USA (Curry M, et al), published a prospective blinded data collection and objective evaluation study (Objective Structured Assessment of Technical Skills) of three several stages using the Da Vinci robotic surgery system in an academic university medical engineering/computer science lab environment. Among the advantages of robotic surgery are greater precision in small and confined anatomical areas, a better view in the operating field, 3D magnification and refinement of the surgeon's movements, making the procedure safer and less tiring.
ABSTRACT
The role of transoral robotic surgery in the treatment of oropharyngeal cancer: a review of the literature. Transoral robotic surgery and adjuvant therapy for oropharyngeal carcinomas and the influence of p16 (INK4a) on treatment outcomes. Transoral robotic surgery for oropharyngeal carcinoma and its impact on patient-reported quality of life and function.
Transoral robot-assisted surgery for head and neck squamous cell carcinoma: one- and 2-year survival analysis. Selective neck dissection and intensified postoperative radiation and chemotherapy for oropharyngeal cancer: a subgroup analysis of transoral robotic surgery at the University of Pennsylvania. Transoral robotic surgery for oropharyngeal squamous cell carcinoma: a prospective study of feasibility and functional outcomes.
Transoral robotic surgery using a flexible carbon dioxide laser for tumors of the upper aerodigestive tract.
