Cognitive engineering and risk assessment in complex systems: applications in the healthcare domain / Alessandro Jatobá. Next, we present the motivation, exploring the relevance of the research problem to the Brazilian healthcare system at a higher level of detail.
Research Problem, Significance, and Objective
The specific characteristics in complex systems make them difficult to support by technology, as design for such work environments requires techniques capable of handling variability, uncertainty, emergence, and dependencies between systems. Thus, this thesis aims to describe promising contributions from cognitive engineering in the design of complex sociotechnical systems, applied in the field of health care.
Research (Sub) Questions
We initially address the problem of finding ways to construct consistent factual descriptions of the work of patient triage processes in the primary care domain to drive the design of improved work situations and support devices. By addressing this question, we can understand the advantages and limitations of technology tools in decision support for patient triage in primary care.
Motivation
The transformation of health work situations is particularly difficult because health work relies on the competences of experts and these experts require autonomy in the performance of their tasks. Furthermore, primary health care in Brazil has become the most important source of health care assistance.
Research Settings
In this case we claim that health care systems – whether public or private – are extremely dependent on the skills and specialties possessed by their professionals, many of them obtained through academic education – and, consequently, on the protocols it has developed any profession. Moreover, in primary health care, actions and activities occur "at the edge of the health care system" and involve many interrelationships between the planning and management of the system and its work processes, raising crucial issues for assistance such as health promotion and disease prevention (SCHREIBER, PEDUZZI, et al., 1999) s.
Structure of the Thesis
Recommendation or implementation of improvements in risk assessment work situations in health care: This class of results is fulfilled by articles. Design for patient risk assessment in primary care: a case study for ergonomic work analysis.
Complex Sociotechnical Systems
Therefore, even with the intrinsic or extrinsic interference of external or internal agents, the system is able to maintain its purposes (VIDAL and CARVALHO, 2008). While the positive self-regulation increases fluctuations in system operation that promote changes that affect its stability, negative self-regulation outweighs the variations observed to stabilize the operation of the system.
Cognitive Ergonomics
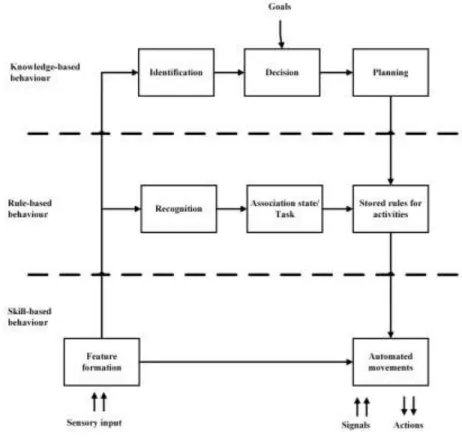
Moreover, to include essential aspects of work in the analysis - such as the context in which it takes place - more is required than describing activities, but describing the cognition of employees. The purpose of CTA is to capture how the mind works – cognition – to understand how people perform their tasks, or how employees view the way their work takes place.
Triage, Prioritization, and Risk Assessment
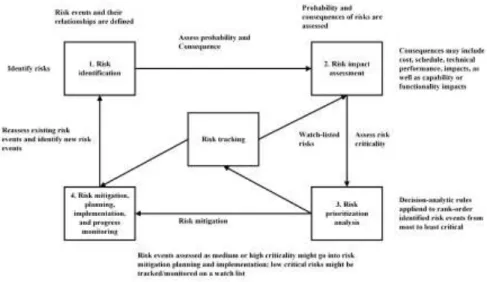
According to the authors of the ISO standards, effects are deviations from the normal conditions. Similarly, Garvey (2009) proposes a five-phase risk management cycle that begins with tracking risk.
Ergonomic Work Analysis
Differences between the results of prescribed and normative work reveal opportunities for designing improved work situations. By focusing on the essential role of the signal rather than on the movements of workers on machines, ergonomic work analysis becomes the opposite of work analysis based on the study of time and motion (OMBREDANE e FAVERGE, 1955; WISNER, 1995).
Cognitive Work Analysis
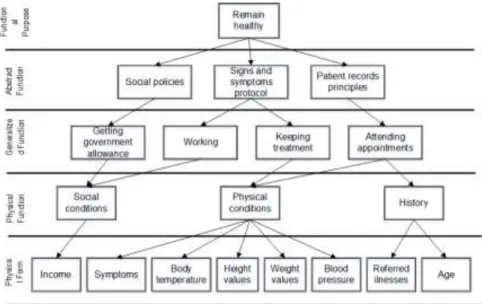
Models of physical form: represent the spatial distribution of matter in the environment, as a portrait of the physical landscape. Models of physical function: represent the physical structure of the system and its functional properties, e.g.
Fuzzy Sets Theory and Fuzzy Logic
During fuzzyfication, the input values are evaluated and calculated according to fuzzy rules inherent in the fuzzy model used. Each fuzzy function of the model produces output values between 0 and 1, which represent the membership level of the output value compared to the fuzzy rule.

Introduction
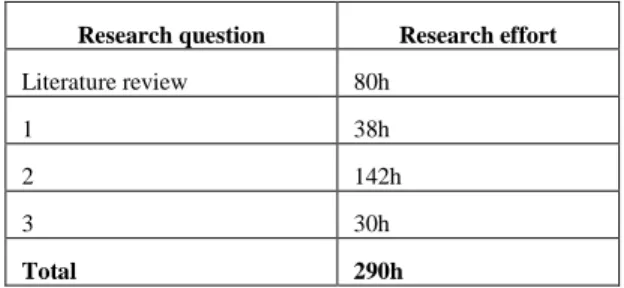
In this chapter we present a systematic literature review, which was carried out to identify, analyze and interpret scientific evidence related to the contributions of human factors and ergonomics to the design of tools, devices and work processes for risk assessment in the to support the context of healthcare. The purpose of this paper is therefore to present a systematic literature review that aims to identify, analyze and interpret available scientific evidence related to the contributions of cognitive engineering (HOLLNAGEL e WOODS, 2005; . RASMUSSEN , PEJTERSEN e GOODSTEIN, 1994) to the design of tools, devices and work processes to support patient triage and risk assessment.
Materials and Methods
Research Questions
Should we expect more effective patient triage and risk assessment when applying human factors and ergonomics to the design of supporting tools and processes? What evidence is there that applying human factors tools and techniques produces more significant results in understanding the real work of patient triage and risk assessment?
Selection Criteria
Cognitive work analysis” OR “Cognitive task analysis”) AND (“Risk assessment” OR “Triage” OR “Patient triage” OR “Risk management”) AND (“Care”). Studies presenting good practices, lessons learned and success factors in applying human factors and ergonomics concepts in the design of patient triage and risk assessment;
Definition of Outcomes
A tenured professor, head of the ergonomics and human factors laboratory, supervised the committee during the process. The final score for each criterion of methodological quality represents consensus among committee members.
Results
Design of risk assessment decision support for health care
Regarding our second research question, according to Hundt et al. the use of proactive risk assessment can help designers identify potential problems that, if ignored, often result in poor health IT implementation. Regarding our sub-question, Johnston et al's study uses Healthcare Failure Mode and Effects Analysis (HFMEA) (STALHANDSKE, DEROSIER e WILSON, 2009).
Analysis of the impacts of new technologies or processes to risk
However, the authors highlight aspects of complexity in healthcare services, particularly how variability hinders the identification of patterns; and suggest ways to improve health assistance. Both the model and surgeons were also able to pinpoint the risk for specific health complications for patients, partially addressing our first and second sub-question.
Discussion
This shows that the implications of a lack of understanding of actual work performance in design for the complexity of risk assessment in healthcare require further investigation. We can also see that most PubMed publications focused on proposing improvements in occupational risk assessment in healthcare settings.
Conclusions
An opportunity for further study would be to broaden the search to include other contributions of human factors and ergonomics to healthcare design – rather than specific contributions to patient risk assessment – as well as contributions from other fields to healthcare risk assessment. care. This could address important aspects, for example, which areas have recently contributed to the improvement of healthcare services and, consequently, risk assessment in healthcare settings.
Article 1: Designing for Patient Risk Assessment in Primary Health Care: a
Foreword
We wrote four scientific papers to address such research questions – two articles addressed the third research question. All papers have been published or submitted, so we present citation information for all of them in the introduction to the relevant section.
Introduction
Research Problem and Questions
How working conditions can be improved and support devices designed to improve the risk assessment process in primary health care. What are the contributions of ergonomics to the design of improved work situations and support devices for risk assessment in healthcare.
Research Setting
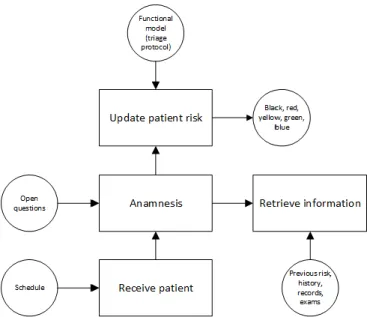
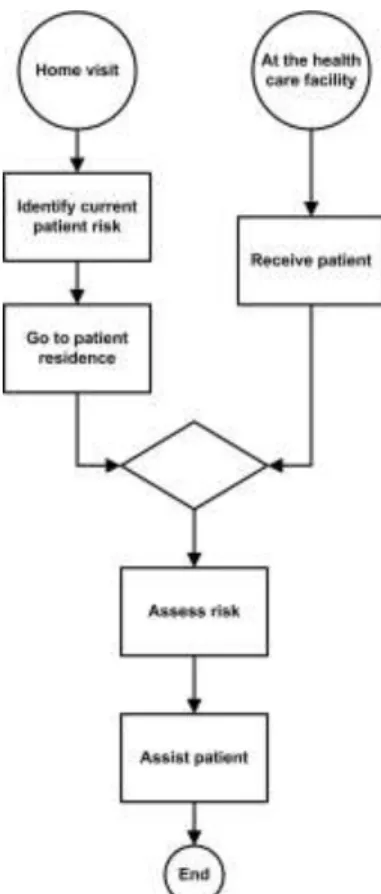
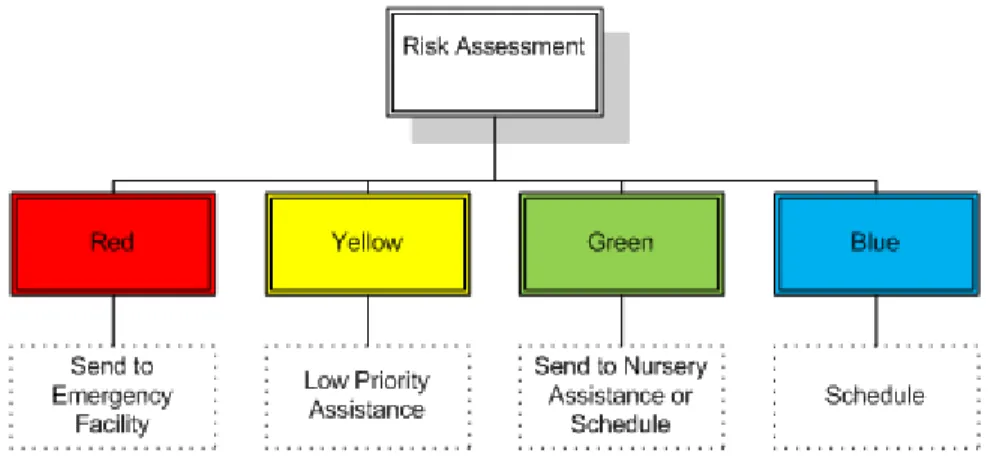
Regardless, all primary care patients must undergo a risk assessment before receiving assistance. The risk assessment process consists of evaluating patients' degree of severity and vulnerability, which results in the prioritization of care measures.
Methods
EWA as a Formative Work Analysis Approach
Through the study of workers' behavior in work situations, EWA increases the understanding of how workers actually see their problems, indicates obstacles to the performance of activities and makes it possible to remove these obstacles through ergonomic action (WISNER, 1995). In order to gain access to the workers' situated cognition and thus the workers' intelligence, we must carry out detailed observation of their behavior (WISNER, 1995).
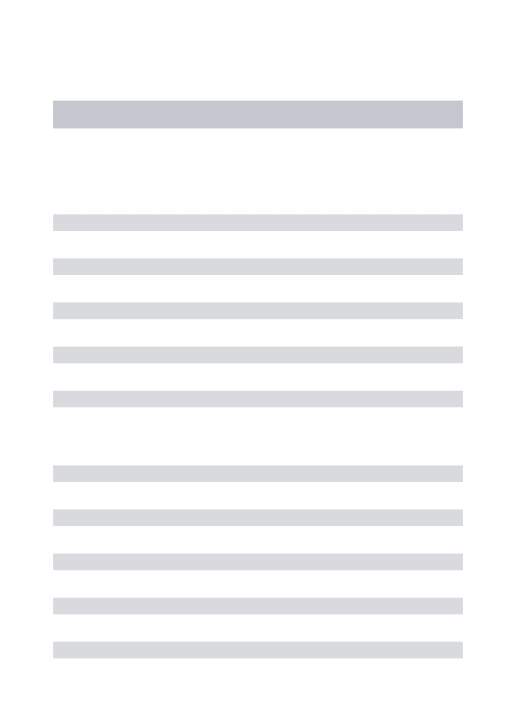
A Four-phase Approach to Ergonomic Work Analysis
Guidance group: professionals who work in the organization and will join ergonomics as part of the analysis team. To achieve this phase's objective, the functional context of the organization must be described, e.g.

Results
In the case of non-compliance in the workplace area criterion, we can conclude that the workers are used to the size of the hazard assessment room. These protocols relate to clinical practice or the use of the color scale of risk assessment.

Discussion
Systematic approaches such as EWA facilitate domain understanding and problem identification by considering different perspectives. Although there have been some efforts by software experts to involve users in the development of health care information technology, this has not been sufficient to ensure a proper understanding of users' needs, and many cases of failure remain.
Conclusions
Article 2: Contributions from Cognitive Engineering to Requirements
Foreword
Introduction
Considering the healthcare context, effective evaluations of healthcare information systems are necessary to ensure that systems adequately meet the requirements and information processing needs of users and healthcare organizations (KUSHNIRUK e PATEL, 2004). Human factors and ergonomics are recognized as a discipline that allows healthcare systems to be redesigned to achieve better quality of care.
Research Problem and Objective
This suggests that organizations focus on high-value requirements rather than meeting 100% of requirements. Focusing on the 20% of features that provide 80% of the software's value can maximize investment in software development and increase user satisfaction (THE STANDISH GROUP, 2013).
Research Questions
If we are to support complex work, real-world knowledge about the complex world of work must be obtained to efficiently design appropriate information systems, as organizations require knowledge to be easily accessed and shared in order to cope with work effectively. (GREENSPAN, MYLOPOULOS and BORGIDA, 1982; WANG and CHOUNG, 2015; COLOMBO, KHENDEK and LAVAZZA, 2012). Furthermore, to provide job support, one must first understand the nature of the system to be supported, as how we see the system determines what is important to support it (CHECKLAND, 1999).
Material and Methods
Typically, the people involved in starting the requirements engineering process have many roles, experiences, and expectations. The phases of the approach should be performed iteratively (ie, it is not necessary to complete one step in order to start the next one).
Results
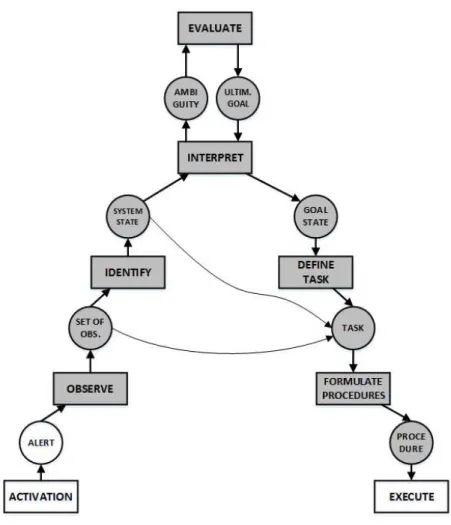
Patient Call: According to the passwords displayed on the panel, patients are called Schedule an appointment. However, in the decision-making scale, states of knowledge are described as the results of the information processing activities that enable them.
Towards Requirements Specifications
Therefore, the requirements that can be derived from the information processing activities, and their inputs, outputs, constraints and processing rules, are also described in the decision ladder. Fields should appear in the FHS protocol in the following order: vital signs, arterial pressure, weight, and height.
Discussion
In these interviews, healthcare professionals saw all models produced and the resulting specifications. Regarding the identification of inputs and outputs of activities, more than half of respondents stated that they were 'moderately' represented.
Conclusions
When asked how they could benefit from adopting IT to support specific candidates in their domain, only one of the professionals interviewed responded. Furthermore, process models have been used to represent the boundaries of the process, providing means for deeper analysis and modeling with adequate tools.
Article 3: Supporting Decision Making in Patient Risk Assessment Using a
Foreword
Introduction
Motivation
In the specific case of patient risk assessment, there are protocols that describe decision-making criteria. Therefore, we developed a model based on MCDM principles to represent the decision problem of patient risk assessment in primary care.
Research Problem and Question
We demonstrate the potential of the proposed approach by applying it to a primary care facility in Brazil. How the practices, protocols, mental models and decision-making of healthcare professionals can be built into an inference engine capable of providing a decision support tool to improve work situations in patient risk assessment in primary care.
Materials and Methods
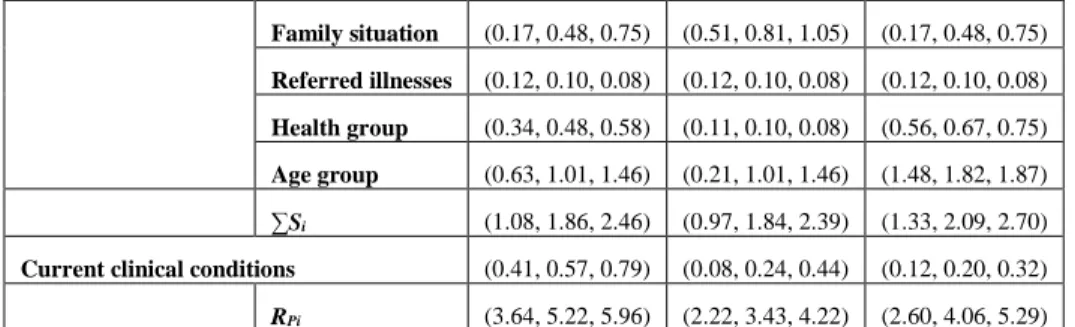
One of the most important normative approaches to decision theory is the expected utility model. Finally, equation 5-2 shows the risk to the patient (Rp), obtained by the sum of each sub-criterion, multiplied by its relative weight (λs), and multiplied by the relative weight of the main criterion (λC).
Results
For example, we can see in Figure 5-28 that the risk of the first patient is located between the green, yellow and red fuzzy sets, but most of its area occupies the yellow space, which means that according to the approach we propose in this paper, the patient must potentially be assigned the risk yellow. Similarly, in figure 5-29 we see the conditions for the second patient, where the calculated risk mainly occupies the green fuzzy set, which shows the potential for the risk green for this scenario.
Discussion
Furthermore, we see in Figure 5-30 shows slightly greater potential for the color green rather than the color yellow, with little potential for the color red in the third scenario. Regarding the third scenario, 60% of the respondents said that the color should be assigned to the patient green, and 26% said that the patient should be assigned yellow.
Conclusions
Aspects of shared decision-making in the medical context, many of which emphasize patient-physician shared participation in the medical decision-making process, should be considered in these cases (MOUMJID, GAFNI, et al., 2007). It would therefore be interesting to implement such a function in the fuzzy model to support this problem and provide more consistent risk suggestions.
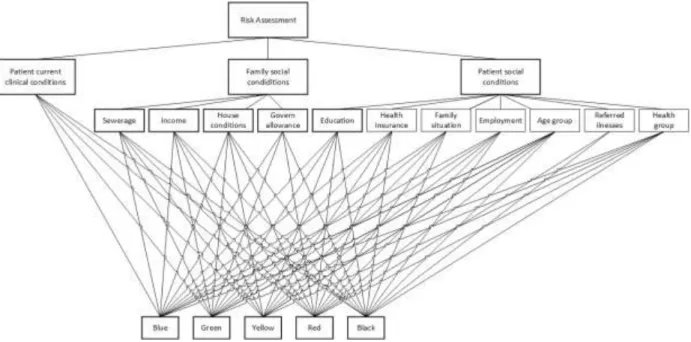
Article 4: A Hierarchical Approach for Triage on Family Health Care
Foreword
Introduction
Thus, the approach proposed in this work is inspired by Primary Health Care Institutions (PHFs) implementing a family health care strategy in the city of Rio de Janeiro. In this paper, we propose an approach to provide multiple inputs to the risk assessment process in primary health care.
Motivation
We use concepts of Fuzzy Logic and Analytical Hierarchy Process (AHP) to contribute to the standardization of this process, to minimize discrepancies in patient risk assessments between teams, thereby improving the quality of decision making. Considering the range of decisions that professionals make in carrying out their activities, the complexity of the system in which their work is carried out, which literally involves the life and death of people – the approach presented in this article can make an important contribution to improving working conditions, providing more input for decision-making.
Results
This set of criteria/symptoms proposed by the authors was presented to the professionals working in PHF. In the case shown in this work, for each degree of risk represented by a color there is a series of criteria.
Conclusions and Further Work
In this chapter we present a discussion of the results of this thesis, as a summary of the discussions presented in the results chapter. Making Health Care Safer II: An updated critical analysis of the evidence for patient safety practices.