Fernando Carlos de Landér Schmitt Fernando Manuel Mendes Falcão Reis Francisco José Miranda Rodrigues da Cruz Inês Maria Falcão Sousa Pires Marques Isaura Ferreira Tavares. José Carlos de Magalhães Silva Cardoso José Henrique Dias Pinto de Barros José Luís Dias Delgado. José Manuel Pereira Dias de Castro Lopes José Paulo Alves Vieira de Andrade Manuel Jesus Falcão Pestana Vasconcelos Maria Augusta Vieira Coelho.
Maria Dulce Cordeiro Madeira Maria Leonor Martins Soares David Patrício Manuel Vieira Araújo Soares da Silva Raquel Ângela Silva Soares Lino. Ovídio António Pereira van Costa Rui Manuel Almeida Mota Cardoso Rui Manuel Bento de Almeida Coelho Serafim Correia Pinto Guimarães.
CONTENTS
AMI — acute myocardial infarction aOR — adjusted odds ratio AUC — area under the curve BMI — body mass index (kg/m2) CACC — carotid artery cross-clamping CAD — coronary artery disease CBC — complete blood count. PAD — peripheral arterial disease PLR — platelet to lymphocyte ratio PSM — propensity match score RA — regional anesthesia RBC — red blood cells.
ABSTRACT
Carotid endarterectomy (CEA) has been established as the recommended treatment for symptomatic internal carotid stenosis (CS) and for all asymptomatic patients with a CS grade of 60–99% who were classified as representing a potentially high risk of a further stroke. Previous guidelines recommended tighter Doppler ultrasound monitoring (DUS) in patients with CACC-associated intraoperative neurologic deficit (IND) due to higher likelihood of long-term hemodynamic stroke, although evidence for its benefit is lacking. The assumption that IND patients have a higher risk of developing a hemodynamic stroke if the ipsilateral carotid artery becomes stenosed or occluded justified the recommendation for the need for additional monitoring of the risk of restenosis after endarterectomy.
For inclusion in the control group, the next consecutive patient who underwent the same surgical procedure but without IND was selected in a 1:1 ratio. The current study does not support the hypothesis that patients who presented with IND during internal carotid test clamping are at a higher risk of developing late stroke.
RESUMO
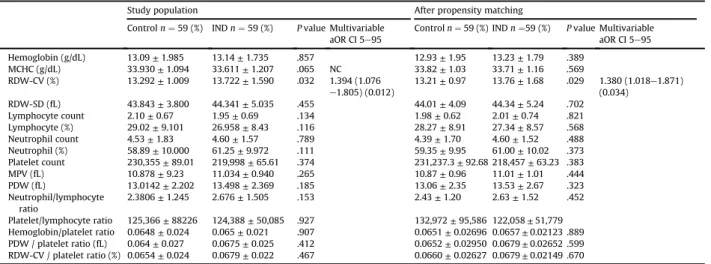
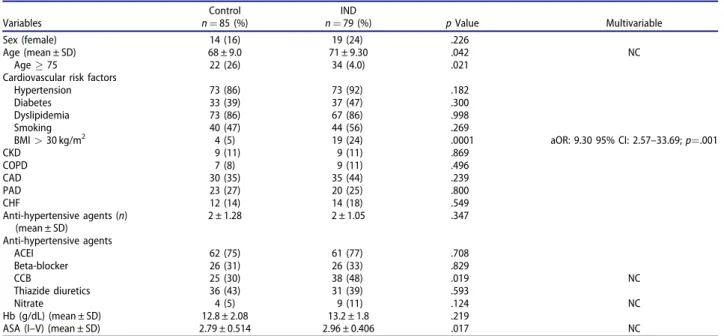
A endarterectomia carotídea (CEA) é o tratamento de escolha para a estenose carotídea sintomática (EC) e para todos os pacientes assintomáticos com um grau EC de 60-99% que são classificados como potencialmente de alto risco para um AVC de novo. A hipótese de que pacientes com IND têm maior risco de desenvolver um AVC hemodinâmico se a artéria carótida ipsilateral tornar-se reestenótica ou ocluída justificaria a necessidade de vigilância adicional com DUS em relação ao risco de reestenose após endarterectomia. Aumento do RDW-CV, idade, obesidade, menor taxa de CS ipsilateral e maior taxa de CS contralateral mostraram-se significativos para predizer IND.
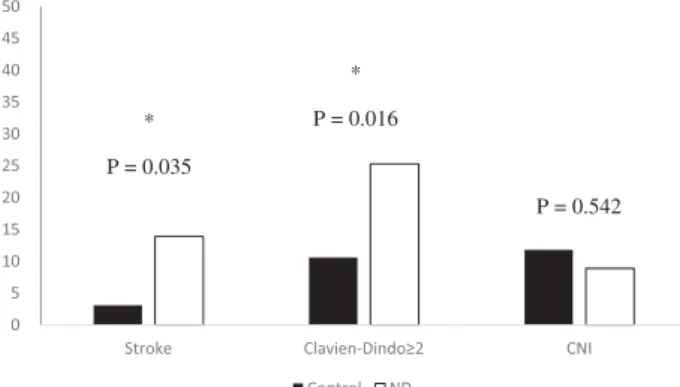
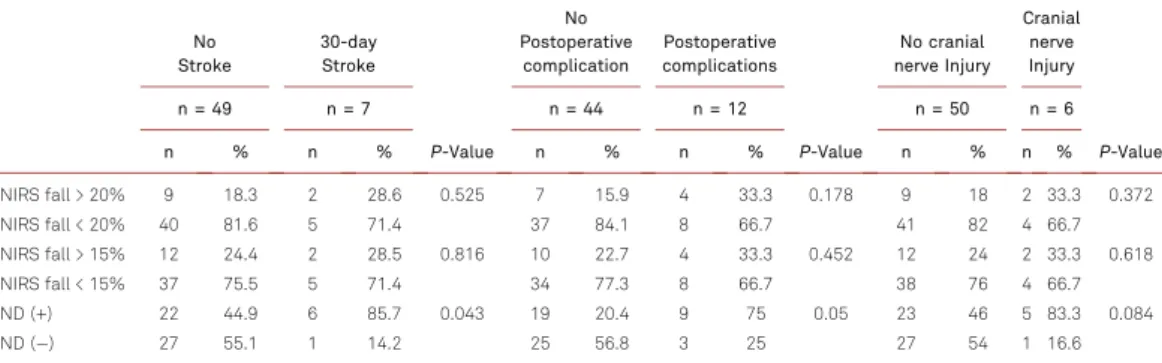
Por outro lado, a presença de IND foi um fator de risco independente para acidente vascular cerebral em 30 dias e complicações pós-operatórias com Clavien-Dindo ≥ 2. Este estudo não suporta a tese de que pacientes que tiveram IND durante o pinçamento da carótida interna têm maior risco de desenvolver AVC tardio (<31 dias).
INTRODUCTION
In addition, these vascular parameters were associated with an increased risk of death within 2 years after major vascular surgery (34), a higher risk of progression or de novo chronic limb-threatening ischemia (CLTI) (35), and the rate of amputations in patients with CLTI ( 36-38), worse limb survival after embolectomy for acute limb ischemia (39), higher risk of complications after surgical repair of abdominal aortic aneurysm (40), and worse prognosis after acute mesenteric ischemia (41, 42). Carotid shunting is the only proven method that can reduce the risk of perioperative stroke due to hypoperfusion (102, 103). Therefore, carotid shunting is a strategy commonly recommended in patients with IND, as it may reduce the risk of persistent ischemic lesions due to temporary interruption of cerebral blood flow (102).
Several studies have attempted to determine whether restenosis is associated with an increased risk of ipsilateral stroke that may warrant routine DUS surveillance after the procedure (128). The effect of age on the risk of restenosis is conflicting between studies, with some authors reporting a higher incidence in patients with increasing age (129) and others in patients younger than 65 years (131).
THESIS OVERVIEW
Neurological examination of the awake patient is considered the most reliable method to assess IND. The rationale for this thesis is the assumption that patients who develop IND during CACC have a higher risk of developing a complete stroke. Evaluation of the perioperative prognostic value of CACC-related IND was central to the significance of this work.
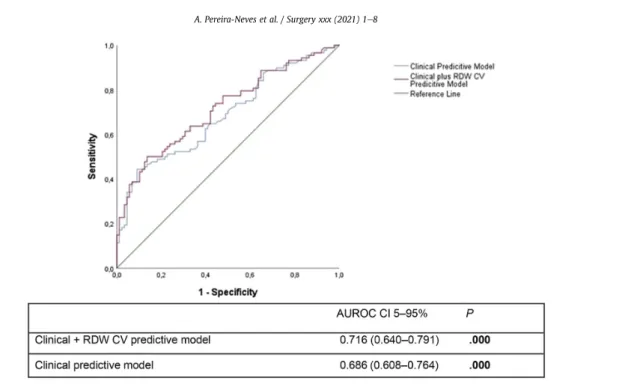
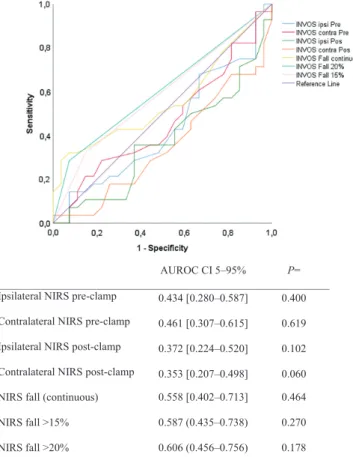
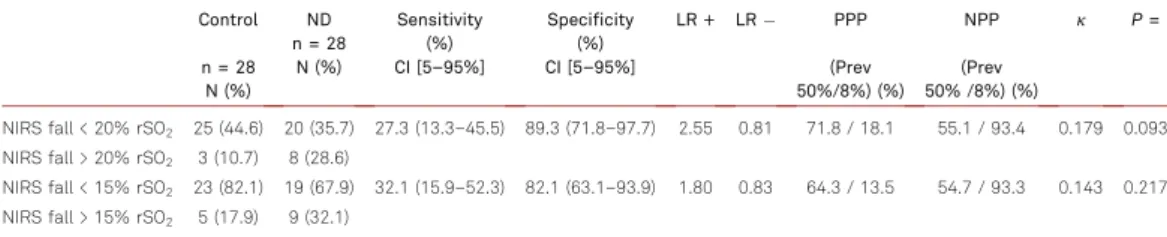
RBC distribution width is associated with hypoperfusion in carotid endarterectomy under regional anaesthesia. 2 Evaluate the diagnostic and discriminatory value of the NIRS cerebral oximeter in detecting cerebral hypoperfusion and determining a high risk of neurological decline;. Efficacy of near infrared spectroscopy cerebral oximetry in detection of critical cerebral perfusion during carotid endarterectomy under regional anaesthesia.
3 Characterize and compare technical approaches - selective shunting or routine non-shunting - in relation to adverse event rates in IND patients under regional anesthesia;. 5 Address the occurrence of adverse CV events, including stroke during the postoperative period and long-term follow-up of patients who had manifested IND. In this subset of patients, progression of stenosis may be more likely to be associated with major hemodynamic shock.
Onset of neurological deficit during carotid artery clamping with carotid endarterectomy under regional anesthesia is not a predictor of carotid artery restenosis. Web of Science Journal of Citation Reports (JCR) Impact Factor from year of publication. Quartile rankings based on Journal Impact Factor (JIF) rankings from year of publication.
Impact of intraoperative neurologic deficits in carotid endarterectomy under regional anesthesia
Routine or selective carotid artery shunting for carotid endarterectomy (and different monitoring methods in selective shunting). This group accounted for 8% of all carotid endarterectomies performed at the center during this time frame. Outcome analysis of carotid clamp cross intolerance during carotid endarterectomy under locoregional anesthesia.Ann Vasc Surg.
Carotid endarterectomy (CEA) is the standard treatment for asymptomatic high-grade carotid stenosis (CS) and >50% symptomatic CS [ 1 ]. Routine or selective carotid artery shunting for carotid endarterectomy (and different monitoring methods in selective shunting).
DISCUSSION
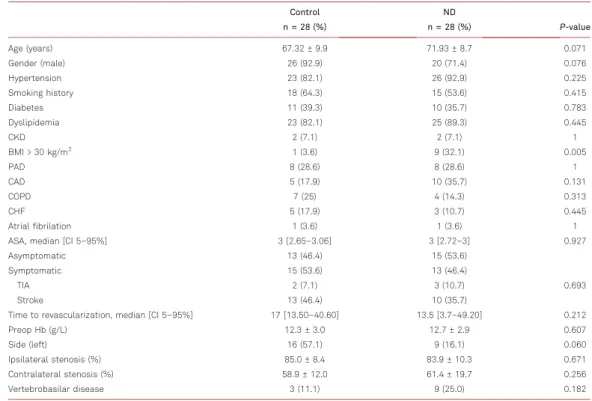
Some ischemic lesions are associated with damage to the ischemic penumbra surrounding the recent infarct, in addition to the traditional association between procedure-related embolization and intra- and postoperative stroke (88). Evaluation of the degrees of strenosis of both carotids using imaging techniques is important, as it is related to impairment of cerebral perfusion and compensatory mechanisms (160, 161). Therefore, it is not surprising that contralateral CS is an exclusion criterion in clinical trials because of the increased perioperative risk of stroke (163, 164).
Some ischemic lesions are associated with damage to the ischemic penumbra surrounding the recent infarct, in addition to the traditional association between procedure-related embolization and intra- and postoperative stroke (88, 144). Consequently, preservation of cerebral autoregulation may contribute to the reduction of ischemic episodes. The option of shunting after a diagnosis of clamping-related IND was left to the surgeon's judgment and experience (199).
Currently, no method of routine or selective shunting has been linked to the production of better outcomes, although the stroke rate was still increased compared to the patients with IND who did not undergo carotid shunting (shunters vs. non-shunters) (199) . For this reason, it cannot be discarded whether stroke related to restenosis in patients with IND is more relevant, since the lack of cerebral vascular reserve leading to deficits during clamping may also cause less tolerance for the progression of restenosis. Several limitations are inherent in the papers that are the basis of the present thesis.
The lack of randomization option may have confounded the results, although the stroke rate was still increased compared with the patients with IND who did not undergo carotid shunting (shunters vs. non-shunters) (199). Finally, limitations also arise from the long recruitment time frame due to the low rate of patients with post-CACC neurological deficit (8%), although a considerably large sample is presented together with a control group. NIRS does not appear to add substantial clinical benefits to the awake test due to its low association with postoperative outcomes.
Circle of Willis incompleteness is associated with EEG-based shunting during carotid endarterectomy.
ACKNOWLEDGMENTS
Concluo esta dissertação com profundo sentimento de dever cumprido e gratidão pelas oportunidades que me foram dadas neste percurso tão diferente como especial. Gostaria de agradecer especialmente ao Professor Doutor José Paulo Andrade, promotor desta tese, pela sincera amizade. Por todas as oportunidades acadêmicas que você me deu, mesmo antes de provar qualquer valor.
Professor Dr. Ricardo Vaz, que me despertou desde cedo para a exigência da técnica e a pequena possibilidade de erro. Ao Professor Doutor Pedro Pereira, Professora Susana Sá, Professora Susana Silva e Professor Armando Cardos pelo apoio e incentivo no crescimento científico e técnico e pelas oportunidades oferecidas. Não posso deixar de agradecer à Professora Carla Lopes e à Professora Ana Azevedo pelo privilégio de poder contar com toda a sua disponibilidade e ser um exemplo no meu percurso académico e profissional durante muitos anos.
Professor Doutor Adelino Leite Moreira que me deu a oportunidade de iniciar o doutoramento em Ciências Cardiovasculares. No Serviço de Cirurgia Vascular, recebi apoio fundamental para conciliar prática, pesquisa e ensino, inicialmente os Drs. José Teixeira e atualmente o Professor Doutor Armando Mansilha, a quem agradeço também pelo importante apoio e orientação durante a maior parte do processo.
Sua visão pessoal da sociedade e o modo de vida das relações interpessoais são valores importantes que ele me transmitiu. À professora Marina Neto, ao professor José Pedro Pinto e ao mestre Joel Sousa, meus amigos e companheiros de geração. Claúdia Pimenta e à Professora Joana Mourão pela coragem e vontade de inovar, o que lhes permitiu implementar um programa de anestesia regional para doença carotídea.