ORI GI N AL ART I CLE
Abstract: Background:
distressing for the patient, anaesthesiologist and the surgeon, especially when the patient is under regional anaesthesia. Aim and Objectives:
was designed to evaluate the efficacy of butorphanol and tramadol in the control of shivering under spinal anaesthesia and to compare their side effects. To compare the efficacy, potency, response time, hemodynamic alterations, and adverse effects of intravenously administered tramadol and butorphanol for relief of shivering occurring during spinal anaesthesia. Material and Methods:This randomised prospective study was conducted in 100 patients who developed shivering under spinal anaesthesia during various abdominal, orthopaedic, urological and gynaecological procedures. Patients with fever, acute infections, drug allergy and compromised cardiorespiratory functions were not included in the study. On shivering, patients were randomly allocated in two groups of 50 patients each who received intravenously 1mg of butorphanol or 50 mg of tramadol in a double blinded manner. Control of shivering, time taken for cessation, recurrence, hemodynamic changes, axillary temperatures and side effects were noted and compared for both the groups. Collected data were analysed using Chi square test and Student's unpaired t test. Results: All patients were relieved of shivering after butorphanol, 58% within 1 min, 82% within 3min and 100% within 5 min. Tramadol relieved shivering in 98% of patients, 32% within 1 min, 60% within 3 min, 98% within 5 mins (p< 0.05). There was higher incidence of side effects like nausea and vomiting with tramadol (16% and 12% respectively) as compared to butorphanol. Conclusion:
Shivering is very uncomfortable and
The present study
Control of Intraoperative Shivering Under Spinal Anaesthesia- A Prospective
Randomized Comparative Study of Butorphanol with Tramadol
1* 1
Astha Palan , N.K Agrawal
1
Department of Anaesthesiology, Jawaharlal Nehru Medical College, Datta Meghe Institute of Medical Sciences Sawangi, Meghe, Wardha- 442001 (Maharashtra) India
Both the drugs, tramadol and butorphanol are effective to control shivering after spinal anaesthesia. Butorphanol is better as compared to tramadol in treating shivering under spinal anaesthesia because of its quicker onset of action, higher success rate and fewer side effects like nausea and vomiting.
Keywords: Butorphanol, Perioperative Shivering, Spinal Anaesthesia, Tramadol
Introduction:
Subarachnoid block is a widely used and safe method for various surgical procedures. Shivering occurs after both regional and general anaesthesia. The incidence of shivering has been found to be quite high, approximately 40-60% with the volatile anaesthetics [1]. Shivering occurring after regional anaesthesia is one of the very common complications and around 30% of patients even under epidural anaesthesia develop shivering [2]. Shivering is usually defined as readily detectable tremor or fasciculation of face, neck, jaw, head, trunk or extremities lasting longer than 15 seconds [3]. Shivering is very uncomfortable and distressing for the patient, anaesthesiologist and the surgeon, especially when the patient is under regional anaesthesia. Apart from this, it is also physiologically stressful for the patient. So it deserves prevention and rapid control.
lead to increase in oxygen consumption by 100-600% with increased carbon dioxide production [5]. It can cause arterial hypoxemia, raised intracranial and intraocular pressure [4]. It can lead to adverse post operative outcomes like increased wound pain and infection which leads to delayed discharge of the patient [6].
The exact cause of shivering under spinal anaesthesia is not well understood. Spinal anaesthesia prevents peripheral vasoconstriction and increases cutaneous heat loss. The threshold for vasoconstriction and shivering is decreased by 0.6°C above the level of block and this reduction is directly proportional to the number of segments blocked [7, 8]. Spinal anaesthesia causes redistribution of heat from core (below the level of block) to periphery due to spinal induced vasodilatation [3]. All these factors under spinal anaesthesia cause shivering and predispose patients to hypothermia. Other causes of shivering include- pre existing fever or septicemia, cold temperature of operation theatre, rapid infusion of cold or contaminated IV fluids, drug allergies, blood transfusion reactions, etc.
The various treatment modalities to control shivering include pharmacological and non pharmacological methods. The non pharmaco-logical methods include use of heaters, warming blankets, radiant heat, forced air warmers, infusing warm IV fluids, etc [9-11]. Pharmacotherapy still remains the most widely accepted method for controlling shivering because of the ease in availability of various drugs which are cheap and inexpensive.
Various pharmacological interventions including pethidine, tramadol, butorphanol, clonidine, ondensetron, ketamine, doxapram, etc have been tried in control of shivering [12-14]. As all the available drugs to control shivering have various adverse effects, still there is no single well accepted drug for control of shivering.
Over the past few years, tramadol has gained popularity and is most widely used drug to control shivering after spinal anaesthesia. But use of tramadol is associated with many side effects like nausea, vomiting and dizziness which are unpleasant for the patient [15]. Butorphanol, an easily available opioid, is commonly used as an IV analgesic agent but there are very few studies demonstrating its use for control of shivering. Hence, in search of a more safer, effective and faster acting drug, we have conducted this study to compare the efficacy, potency, response time, hemodynamic alterations, and adverse effects of intravenously administered tramadol and butorphanol for relief of shivering occurring during spinal anaesthesia.
Material and Methods:
After obtaining Institutional Ethics Committee approval and written/informed consent from patients, we performed this prospective, randomized comparative study in cases of both genders between 20 to 50 years of age from July 2014 to May 2016. Patients of American Society of Anaesthesiologists Physical Status (ASA) I-II, posted for procedures (lower abdominal, uro-genital, orthopaedic and gynaecological) under spinal anaesthesia, who developed shivering during the intra operative period were included in the study. Patients with fever, hypo or hyperthyroidism, morbid obesity drug allergy, compromised cardiopulmonary functions and neuromuscular diseases were excluded.
temperature was recorded using a mercury thermometer in the axilla placed in the vicinity of the axillary artery. Operation theatre temperature
o
was maintained at 22-25 C. All patients included in the study were premedicated with tablet Diazepam 5mg on the night before surgery. All patients in our study received spinal anaesthesia in sitting or lateral position using 25G Quinke needles via midline approach in the L3-L4 intervertebral space under strict aseptic precautions. Following free flow of CSF, 15-20mg of 0.5% Bupivacaine (hyperbaric) was injected depending on the duration and type of surgery (3-4ml). All patients were adequately covered with surgical drapes. No other warming device was used.
100 patients who developed shivering after administering spinal anaesthesia were included in the study and data was recorded from patients who continued to shiver for at least 2 minutes. Shivering of grades 2 and above as per the Scale of Shivering was considered to require treatment. The intensity of shivering was graded on the following scale [16].
When patients developed shivering of above mentioned grades for a minimum period of 2 minutes, the axillary temperature was recorded at the onset of shivering and they were randomly allotted by draw of lots method, to one of the two study groups of fifty each: Group B - Butorphanol group (1mg) and Group T - Tramadol group (50mg).
The study drug was then administered slowly intravenously (over 30 seconds) as per the allotted group. The time from drug administration till the patient stopped shivering was accurately noted (using a stopwatch). Response to the drug was assessed as: Success (absence of shivering or Null (shivering intensity not controlled). Patients were monitored for- grade of shivering, temperature, heart rate, oxygen saturation, respiratory rate and blood pressure at intervals of 1 minute for the first 5 minutes and thereafter 10, 20 and 30 minutes till the cessation of shivering. Patients were closely monitored for failure of the drug, recurrence of shivering, sedation score and side effects such as nausea, vomiting, pruritis, respiratory depression, bradycardia and hypotension. Respiratory depression was defined as respiratory rate less than 8 per min and bradycardia as heart rate below 20% of baseline. Level of sedation was assessed using the following scale- Grades of sedation [17] Grade Clinical Signs
0 No shivering
1 Piloerection, peripheral vaso-constriction, peripheral cyanosis without other cause but without visible muscular activity.
2 Visible muscular activity confined to one muscle group
3 Visible muscular activity in more than one muscle group
4 Gross muscular activity involving the entire body
Grade Sedation
0 Alert
1 Arouse to voice
2 A r o u s e w i t h g e n t l e t a c t i l e stimulation
3 Arouse with vigorous tactile stimulation
Injection Ondensetron 4mg was administered intravenously to patients who developed nausea and vomiting. Treatment that stopped shivering was considered to be successful. Episodes of recurrence or incomplete control were treated with active warming measures using convection heaters, infusing moderately warm fluids or multimodal therapy (Injection Promethazine 25mg, Injection Pheniramine maleate 10 mg) and the test drug was considered unsuccessful.
Statistical Analysis:
Demographic profiles and vital parameters were expressed as mean ± standard deviation. Statistical analysis was done by using descriptive and inferential statistics using Chi square test and Student's unpaired t test. Software used in the analysis were SPSS 17.0 version, EPI-INFO and GraphPad Prism 5.0 and p < 0.05 is considered as level of significance.
Results:
Patients of both the groups were comparable with no significant difference regarding demograhic profile, ASA grading and duration of surgery (Table 1). The patients of both the groups were comparable with respect to the grade of shivering (Table 2). None of the patients of either group had shivering of grade 4.
There was a significant fall in the axillary temperature during shivering in both the groups as compared to the baseline temperature (Table 3).
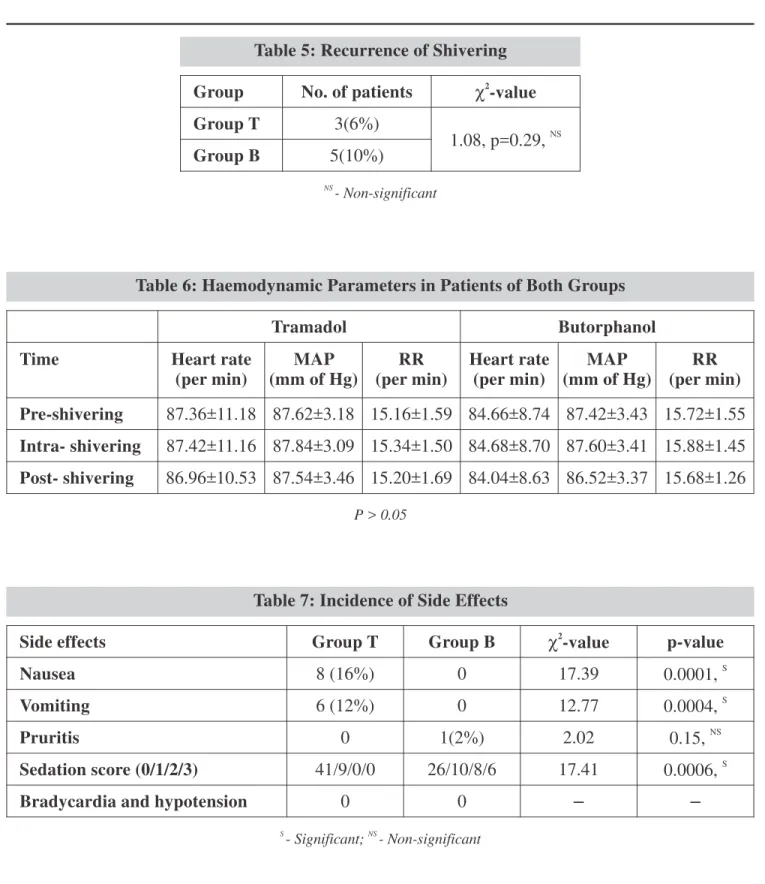
All patients were relieved of shivering in butorphanol group, 58% within 1 min, 82% within 3 min and 100% within 5 min. In tramadol group, 32% within 1 min, 60% within 3 min, 98% within 5 min and 2% of patients had no relief. There was a statistically significant difference in the relief of shivering at 1 min among both the groups. Both butorphanol and tramadol were found to be equally effective after 5 min (Table 4). The recurrence of shivering occurred after 30 min in 5 patients (10%) in butorphanol group and 3 patients (6%) in tramadol group which was statistically not significant (Table 5). All the patients remained haemodynamically stable throughout the study period and no statistically significant difference was noted in heart rate, mean arterial pressure and respiratory rate between both the groups (Table 6). The incidence of nausea and vomiting were found in 8 patients (16%) and 6 patients (12%) respectively in tramadol group as compared to none in butorphanol group which was statistically significant. One patient in butorphanol group complained of pruritis as compared to none in tramadol group (Table 7).
All patients in both the groups were assessed for sedation 5 mins after giving the study drug. We observed that butorphanol group is associated with statistically significant higher sedation scores. None of the patients in either of the groups had sedation score of 4 (Table 7).
Patient variables Group T Group B P value
Age (years) 36.84±8.33 36.20±7.74 NS
0.36,
Sex (M/F) 32/18 30/20 0.68, NS
Weight (kg) 58.14±7.98 57.46±8.63 0.93, NS
ASA Status (I/II) 27/23 24/26 0.54, NS
Duration of Surgery (min) 76.16±15.84 74±18.18 0.58, NS Table 1: Demographic Profile of Patients in Both Groups
NS
Group Grade 2 Grade 3 c2-value p-value
Group T(n=50) 27(54%) 23(46%)
0.72 0.39
Group B(n=50) 24(48%) 26(52%) NS
p>0.05
Groups Baseline (pre shivering)
Mean ± S.D.
During shivering Mean ± S.D.
Post-shivering Mean ± S.D.
Group T 98.36±0.40 96.91±0.39
S (t=22.97, p-value=0.0001, )
98.47±0.38 NS
(t=1.33, p-value=0.18, , p>0.05)
Group B 98.44±0.38 96.88±0.46
S (t=20.40, p-value=0.0001, )
98.51±0.39 NS
(t=1.08, p-value=0.28, , p>0.05) Table 2: Shivering Grade in Both the Groups
Table 3: Mean Data of Fluctuations in Axillary T (°F) Observed at Different Time Intervals in Both Groups
Relief after injecting the drug Group T(n=50) Group B(n=50) c2
-value
Within 1 min(0-60sec) 16(32%) 29(58%) 13.66
S p=0.002,
Between 1 to 3 min(61-180sec) 14(28%) 12(24%) 0.41
NS p=0.51,
Between 3 to 5 min(181-300sec) 19(38%) 9(18%) 9.92
S p=0.0016,
Between 5 to 10 min(301-600sec) 0 0 0
Between 10 to 20 min(600-1200sec) 0 0 0
No relief at all 1(2%) 0 2.02
NS p=0.15, Table 4: Time Taken for Relief of Shivering after Giving Study Drugs
NS
- Non-significant
S
- Significant; NS
- Non-significant
S
- Significant; NS
Group No. of patients c2-value
Group T 3(6%)
NS 1.08, p=0.29,
Group B 5(10%)
Table 5: Recurrence of Shivering
Tramadol Butorphanol
Time Heart rate
(per min)
MAP (mm of Hg)
RR (per min)
Heart rate (per min)
MAP (mm of Hg)
RR (per min)
Pre-shivering 87.36±11.18 87.62±3.18 15.16±1.59 84.66±8.74 87.42±3.43 15.72±1.55
Intra- shivering 87.42±11.16 87.84±3.09 15.34±1.50 84.68±8.70 87.60±3.41 15.88±1.45
Post- shivering 86.96±10.53 87.54±3.46 15.20±1.69 84.04±8.63 86.52±3.37 15.68±1.26 Table 6: Haemodynamic Parameters in Patients of Both Groups
P > 0.05
Side effects Group T Group B c2
-value p-value
Nausea 8 (16%) 0 17.39 S
0.0001,
Vomiting 6 (12%) 0 12.77 S
0.0004,
Pruritis 0 1(2%) 2.02 NS
0.15,
Sedation score (0/1/2/3) 41/9/0/0 26/10/8/6 17.41 S
0.0006,
Bradycardia and hypotension 0 0 – –
Table 7: Incidence of Side Effects NS
- Non-significant
S
- Significant; NS
Discussion:
Shivering presents as a common perioperative problem causing increased metabolic demands, tachycardia and hypertension. It also interferes with routine monitoring like ECG, blood pressure and pulse oximerty. Shivering is seen approximately 40-60% after volatile anesthetics [1]. It has also been observed that around 30% of patients under epidural anaesthesia develop shivering [2].
Intra and post operative shivering is distressing and unpleasant experience for the patient. The exact mechanism of shivering during spinal anaesthesia is not very clear. The possible reasons could be internal redistribution of heat from core to periphery, impaired central thermoregulatory mechanisms, peripheral vasodilatation and heat loss to the environment [3].
Risk factors for hypothermia under spinal anaesthesia are ageing, cold temperature of operation theatre, cold IV fluid, duration of surgery and level of sensory block and the rate of IV fluid infusion [8, 18]. In our study we have tried to minimize the effects of these risk factors by- including patients of age between 20-50 years, maintaining operation theatre temperature at 22-25°, infusing IV fluids at room temperature and at the rate of 2-4ml/kg/hour, keeping the duration of surgery to 90 minutes and keeping the level of sensory block around T6.
There are various non-pharmacological and pharmacological methods to decrease shivering and reduce body heat loss. Pharmacological agents are still the most popular mode for treatment of post anaesthetic shivering because of their easy availability and cost effectiveness. Various neurotransmitter pathways are involved in shivering like opioids, alpha 2 adrenergic, anticholinergic and serotenergic receptors [1]. So
drugs acting on these systems are used to control shivering. Pharmacological methods do not raise the body temperature but resets the shivering threshold to a lower level, which leads to decreased rigors and its frequency. Various drugs like opioids (eg. pethidine, nalbuphine, tramadol or butorphanol) [19, 20] clonidine [21], doxapram [12], ketanserin [12], ondensetron [20], nefopam [12], ketamine[13] etc.; have been used in the treatment of shivering.
Tramadol is an opioid receptor agonist with maximum action on the u- opioid receptors. It prevents shivering by inhibiting the reuptake of norepinephrine and serotonin, hence activating the descending inhibitory spinal pathways. The antishivering effect of tramadol is mediated via serotonergic or noradrenergic receptor or both [22]. The efficacy of tramadol to control shivering is well established [23]. The main adverse effect with the use of tramadol is nausea and vomiting [15, 24].
All the patients were relieved of shivering after giving butorphanol. 58% within 1 min, 82% within 3 min and 100% within 5min. Whereas tramadol relieved shivering in 98% of patients out of which 32% within 1 min, 60% within 3 min and 98% within 5 min. 2% i. e. single patient who received tramadol had no relief at all. On comparing both these groups, butorphanol was found to be more effective in controlling shivering within 1 min and this was found to be statistically significant. Both the drugs tramadol and butorphanol were found to be equally effective to control shivering at the end of 5 mins. Joshi et al.
[20] also found similar results where within 1 min 66.66% of patients in butorphanol group and 46.15% of patients in tramadol group were relieved of shivering. They further observed that at the end of 5 min 100% patients in butorphanol group and 92.3% patients in tramadol group were relieved of shivering. They also found that 7.7% of patients in tramadol group were not relieved at all from shivering. Another study done by Bansal and Jain [26] also found similar difference in butorphanol (83%) and tramadol (73%) in respect of complete cessation of shivering. They also found that butorphanol acts faster (1.8±0.5 min) than tramadol (2.1±1.0 min) to control post spinal shivering.
In our study there were no haemodynamic alterations after treatment with either tramadol or butorphanol. The results were comparable with the study done by Maheshwari et al. [17]
Shivering reappeared after 30 min in 10% of the patients in butorphanol group as compared to 6% in tramadol group which was statistically not significant. Maheshwari et al. [17] have observed a higher rate of recurrence with butorphanol as compared to tramadol (20% versus 8% respectively).
We found that butorphanol causes significant grade 2 and grade 3 sedation (28%) as compared to tramadol (0%). This was comparable to observations made by Joshi et al. [20] and Bansal and Jain [26].
In our study we found that tramadol had a potential to cause side effects like nausea and vomiting. The incidence of nausea (16%) and vomiting (12%) is higher with tramadol as compared to butorphanol. These findings were similar to the findings of other researchers like Shukla et al. [15], Mittal et al. [24] and Mohta et al. [27] who compared tramadol with other drugs having anti-shivering property. In butorphanol group, none of the patients had nausea and vomiting. The results were comparable with studies done by Saini and Mullick [25]. One patient (2%) in butorphanol group had pruritis as compared to none in tramadol group. This was comparable with the study done by Joshi et al. [20] They found 6.67% of patients receiving butorphanol had itching.
Conclusion:
References
1. De Witte, Sessler DI. Perioperative shivering: Physiology and Pharmacology. Anaesthesiology 2002; 96(2):467-84.
2. Sessler DI, Ponte J. Shivering during epidural anaesthesia. Anaesthesiology 1990; 72(5):816-21. 3. Buggy DJ, Crossley AW. Thermoregulation, mild
perioperative hypothermia and post-anaesthetic shivering. Br J Anaesth 2000; 84(5):615-28.
4. Sessler DI. Temperature regulation and monitoring. In: Ronald D. Miller, editor. Miller's anaesthesia. 7th ed. Philadelphia: Churchil Livingstone; 2010: 1539-40. 5. Dal D, Kose A, Honca M, Akinci SB, Basgul E, Aypar
U. Efficacy of prophylactic ketamine in preventing postoperative shivering. Br J Anaesth 2005; 95(2):189–192.
6. Doufas AG. Consequences of inadvertent perioperative hypothermia. Best Pract Res Clin
Anaesthesiol 2003; 17(4):535-49.
7. Kurz A, Sessler DI, Schroeder M, Kurz M. Thermoregulatory response thresholds during spinal anesthesia. Anesth Analg 1993; 77(4): 721-26.
8. Leslie K, Sessler DI. Reduction in the shivering threshold is proportional to spinal block height.
Anesthesiology 1996; 84(6):1327-31.
9. Dyer PM, Heathcote PS. Reduction of heat loss during transurethral resection of the prostate. Anaesth
Intensive Care 1986; 14(1):12-6.
10. Sharkey A, Lipton JM, Murphy MT, Giesecke AH. Inhibition of postanesthetic shivering with radiant heat. Anaesthesiology 1987; 66(2): 249-52.
11. Camus Y, Delva E, Cohen S, Lienhart A. The effects of warming intravenous fluids on intra-operative hypothermia and postoperative shivering during prolonged abdominal surgery. Acta Anaesthesiol
Scand 1996; 40(7): 79-82.
12. Kranke P, Eberhart LH, Roewer N, Tramer MR. Pharmacological treatment of postoperative shivering: a quantitative systematic review of randomized controlled trials. Anesth Analg 2002; 94(2):453-60. 13. Wason R, Jain N, Gupta P, Gogia AR. Randomized
double blind comparison of prophylactic ketamine, clonidine and tramadol for the control of shivering under neuraxial anaesthesia. Indian J Anaesth 2012; 56(4): 370-5.
14. Bhatnagar S, Saxena A, Kannan TR, Punj J, Panigrahi M, Mishra S. Tramadol for postoperative shivering: a double blind comparison with pethedine. Anaesth
Intensive care 2001; 29(2): 149-54.
15. Shukla U, Malhotra K, Prabhakar T. A comparative study of the effect of clonidine and tramadol on postspinal anaesthesia shivering. Indian J Anaesth
2011; 55(3): 242–6.
16. Crossley AWA, Mahajan RP. The intensity of postoperative shivering is unrelated to axillary temperature. Anaesthesia 1994; 49(3): 205-7.
17. Maheshwari BS, Shah SK, Chadha IA. Tramadol and butrophanol for control of shivering: Randomised double blind comparative study. J Anaesthes Clin
Pharmacol 2008; 24(3):343.
18. Vassilieff N, Rosencher N, Sessler D, Conseiller C. Shivering threshold during spinal anesthesia is reduced in elderly patients. Anesthesiology 1995; 83(6):1162-6. 19. Koay CK, Chan WY, Chin MK. Shivering during
regional anaesthesia and its control with Pethidine.
Singapore Med J 1991; 32:160-62.
20. Joshi SS, Arora A, George A, Shidhaye RV. Comparison of intravenous butorphanol, ondansetron and tramadol for shivering during regional anesthesia: A prospective randomized double-blind study. Anaesth Pain & Intensive Care 2013; 17(1):33-9.
21. Attal P, Chhaya A, Singh T, Upadhayaya RM. Comparison of clonidine and tramadol for the control of shivering under spinal anaesthesia. IJBAR 2015; 6(1):25-31.
22. De Witte JL, Kim JS, Sessler DI, Bastanmehr H, Bjorksten AR. Tramadol reduces the sweating, vasoconstriction, and shivering thresholds. Anesth
Analg 1998; 87(1):173-9.
23. Aditi A. Dhimar, Mamta G. Patel, Swadia VN. Tramadol for control of shivering (comparison with pethidine). Indian J Anaesth 2007; 51(1): 28-31. 24. Mittal G, Gupta K, Katyal S, Kaushal S. Randomised
double-blind comparative study of dexmedetomidine and tramadol for post-spinal anaesthesia shivering.
Indian J Anaesth 2014; 58(3): 257.
25. Saini S. A comparative evaluation of butorphanol with pethidine for treatment of postspinal shivering. IJMHS
2014; 4(2): 86-89.
26. Bansal P, Jain G. Control of shivering with clonidine, butorphanol, and tramadol under spinal anesthesia: a comparative study. Local Reg Anesth 2011; 4: 29-34. 27. Mohta M, Kumari N, Tyagi A, Sethi AK, Agarwal D,
Singh M. Tramadol for prevention of postanaesthetic shivering: a randomised double-blind comparison with pethidine. Anaesthesia 2009; 64(2): 141-6.
*