Research Article
Effect of Homocysteine ,Vitamin B12 , Folic acid during pregnancy
Arpita P. Patel, Chandan Chakrabarti*, Arjun Singh, Jatin D Patel, Hitesh A.Mewada, S.L.Sharma*
Department of Biochemistry, Smt N. H. L. Municipal Medical College, Ahmedabad.
Email:[email protected]
Abstract:
Vitamin B12, folic acid and homocysteine are metabolically closely related. At the same time homocysteine is found to be offending factor for vascular pathology causing preeclampsia. On the other hand periconceptional nutritional status influences the vitamin B12 & folic acid level. Which further affect the homocysteine level thus may affect pregnancy outcome. Various contributory factors lead these vitamin deficiencies, maternal nutrition is one of them. Ahmedabad being a predominantly vegetarian city, its population is at higher risk of vitamin B12 deficiency. But no systematic study has been done in Ahmedabad to know whether B12, folic acid and homocysteine levels influence pregnancy. To know this answer this study was planned to know total homocysteine level and its correlation in preeclampsia and normotensive pregnant women.Vitamin B12, folic acid and homocysteine were measured in all the subjects using fluorescence polarized immunoassay in AxSym Immunochemistry analyzer on 60 non vitamin supplemented vegetarian women. Vitamin levels were within lower normal limit. Homocysteine level was higher among preeclampsia patient. From the findings of the present study it can be concluded that measurement of these biochemical parameter in ante natal care are useful for further management and prevention of complication of pregnancy like preeclampsia.
Key words: Homocysteine, Preeclampsia, Vitamin
B12, Folic acid
Introduction:
Preeclampsia, a serious metabolic disturbance of pregnancy that occurs most often following the twentieth week of pregnancy is one of the leading causes of feto-maternal morbidity and mortality. Vascular damage in the maternal utero-placental and fetal umbilical-utero-placental circulation deterioration is the center of the reason of
is uncertain whether such an imbalance occurs before clinical recognition or whether it is related to diet16. On the other hand homocysteine is considered as an individual risk factor for arterial and peripheral vascular disease 11. This aminoacid is derived from demethylation of methionine requiring folate, vitamin B12, B6 as a co-enzyme. Malnutrition or malabsorption of this vitamins / inherited enzymes deficiency also leads to increase in tHcy level 9. On the other hand, endothelial dysfunction, smooth muscle cell proliferation and coagulation abnormalities, stress etc have been attributed for pregnancy complication10,13. Considering this bio-pathological mechanism that result in vascular damage, a relation between serum homocysteine level and vascular related pregnancy complications is possible. But relatively very few data are available on these biochemical parameters in vegetarian women who were not supplemented with B12 and folic acid. Ahmedabad is a perfect platform for elaborate the correlation between serum tHcy and vascular related complications like preeclampsia in pregnant women and also in normotensive pregnant women. Most important aspect is that it is very difficult to know the brand, biological availability & ascertain the exact dose of vitamin that might have received by the patient. So a group of population required who are beyond this doubt. Because of lack of consistency in data, dose response relationship and biological plausibility in this regard, prompted us to undertake this biological study.
Materials and Methods:
included who were not supplemented with vitamins, out of which 20 subjects were healthy normotensive nonpregnant women. Forty antenatal women with singleton pregnancy were considered as study group. In this study pregnant women in Study Group I and II were between 28-40 weeks of gestational age and in most of them are between 36-40 weeks of gestational age. No statistical differences in age of three groups were observed in the present study. All the groups were matched according to socio-economical status and dietary habits. Further all these subjects were divided into two groups. Study group I comprises 20 clinically and laboratory confirmed normotensive pregnant women. Study group II comprising 20 patients with B. P. ≥ 140/90 mm Hg on more than two occasions and persistent proteinuria (>30 mg/day) confirmed by the laboratory as well as by the clinician and or presence of pitting oedema.
Women with diabetes mellitus, chronic hypertension, preexisting renal or liver disorder, H/O thromboembolism, repeated miscarriage, H/O abruption placenta, anemia, preterm labor, H/O smoking, and prior significant illness, women with vitaminB12 and folic acid supplementation were excluded.
Total homocysteine (tHcy) was measured in serum of all subjects using Fluorescence Polarized Immuno Assay technique by AxSym immunochemistry analyser. Commercial kit manufactured by same company was used. Results were assured as per standard quality control regime. The study was approved by institutional review committee.
Table –I
Homocysteine, Vitamin B12, and Folic acid levels in different groups
For the purpose of the analysis,‗t‘ test , analysis of variance , p value have been used. For the purpose of this study 95% confidence level has been chosen and corresponding ‗p‘ value < 0.05 has been taken as significant. Pearson‘s correlation coefficient test was utilized for correlation between variables.
Results
After analysis of samples and calculations of data shows that the control group had the mean homocysteine levels of ( 17.15 ± 6.65 µmol/L) while Study Group I had least homocysteine level of (13.45 ± 4.40 µmol/L ) and Study Group II had highest homocysteine level (19.96 ± 6.43 µmol/L) (Table I)
Mean of vitamin B-12 in control group was 271.7 pg/ml, in Group I was 243.7 pg/ml and in Group II was 157.9 pg/ml whereas folic acid values were 12.18 ng/ml, 9.5 ng/ml, and 6.4 ng/ml respectively. A graphical presentation of Vitamin B12 and Folic acid levels is shown in Fig. 1 and Fig. 2 respectively.
Both vitamin and folic acid levels were found within normal limits but in the lower range in all groups.
Significant difference is observed in the levels of Homocysteine between control and Study Group I (p<0.05) and also between Study Group I and II
Group Homocysteine (Normal : 5-20µmol/L)
Vitamin B12 (Normal : 211-911pg/mL)
Folic Acid (Normal: 7-25 ng/mL)
Control (n=20)
17.15 ± 6.65 271.7 ± 86.87 12.18 ± 4.71
Study Group-I (n=20)
13.45 ± 4.39 243.7 ± 60.90 9.5 ± 4.42
Study Group-II (n=20)
(p<0.001). Study Group-II showed highest mean levels, while the Study Group-I had least mean homocysteine level. Significant difference of homocysteine between Study Group-I and & II (<0.001) was observed. Same significant finding was observed between control and Study Group-I (p<0.05) (Table II)
Table -II
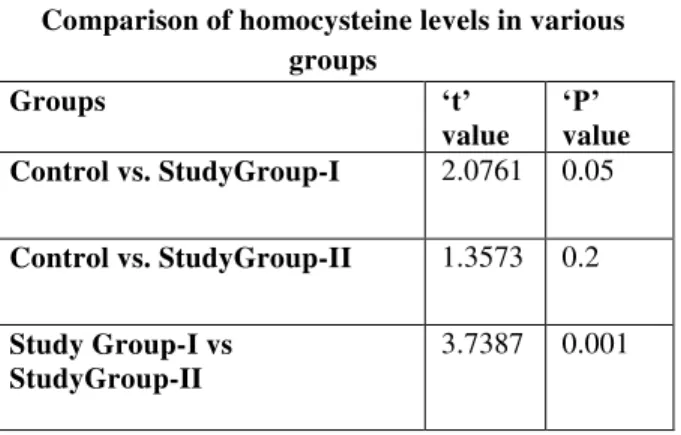
Comparison of homocysteine levels in various groups
Groups „t‟
value
„P‟
value
Control vs. StudyGroup-I 2.0761 0.05
Control vs. StudyGroup-II 1.3573 0.2
Study Group-I vs StudyGroup-II
3.7387 0.001
Our results depict an increase in the value of homocysteine in patients with preeclampsia when compared with normal healthy control and normal pregnant females.
Discussion
Though the exact cause of preeclampsia is still unknown but there are many scientific evidence to prove that it is caused by endothelial dysfunction and increase vasospasm 8 . Altered metabolism of homocysteine, B12, folic acid may lead to this pathology because Homocysteine derived from methionine an essential amino acid requires B12 and folic acid. Dietary habits of people of Ahmedabad may influence these vitamin level and thus homocysteine metabolism. Vegetarian food is also a poor source of methionine so have reduced methylation activity. It is true that microorganisms responsible for synthesis of vitamin B12 are available only in animal kingdom but poor socioeconomic, hygienic & malabsorption would affect the level of these vitamins. As homocysteine, B12 and folic acid metabolism are interlinked, so this may influence the pregnancy complication like preeclampsia.
Endothelial cell dysfunction may also occur and other vital cellular components leading to tissue damage by different factors. This molecule has been implicated
in the pathogenesis of a large number of human diseases including preeclampsia. So we thought it would be interesting to know the relation between homocysteine level in these special groups of population. The present study provides interesting insights that a substantial number of women attend our hospital without any antenatal care and/or vitamin supplementation. This is mainly because of lack of awareness, rapid urbanization, and poor socio economic status in certain group of population in Ahmedabad. Another major limiting factor is that to ascertain the exact dose of vitamin supplementation that has been received by the patients is difficult. So we have considered those populations who were not supplemented with vitamin during the time of sampling/at the time of admission. Relatively small sample size observed in the present study because of these factors. It has been reported that tHcy value between 5 µmol/L to 15µmol/L in fasting subject are considered normal 5. In the present study the mean homocysteine levels in control group was 17.15 ± 6.65 µmol/L and in study group I ( normotensive pregnant ) was 13.45 ± 4.40µmol/L. In study group-II ( preeclamptic pregnant) homocysteine level was
19.96 ± 6.43 µmol/L. Significant difference found
between these two study group. Our findings are supported by the study of walker et al2 .This lower level of homocysteine are observed because of physiological response to pregnancy, increase in estrogen level , hemodilution or increased demand for methionine by both mother and fetus 7 .
In the present study mean of vitaminB12 in control group was 271.7pg/ml, in group I was 243.7pg/mL and in group-II was 157.9pg/mL, and folic acid value was 12.18ng/ml, 9.5ng/ml and 6.4ng/ml respectively. It was observed in the present study that homocysteine level was higher in the preeclamptic group. This high level might get influence by lower concerned vitamins, which were seen in preeclampsia group.
that usually decrease homocysteine level during normal pregnancy. These findings correlate well with study of Singh Urmila et al 1 .In another study done by Power et al 3 analyzed the homocysteine and folate level in women with preeclampsia and normal uncomplicated pregnancies and found significantly higher homocysteine level in preeclampsia than in normal pregnancy (p<0.04).The study of Hogg et al 4 also showed elevated homocysteine levels in women with pregnancy-induced hypertension, preeclampsia at 37 weeks gestation.
Though dietary habits of western population and in Indian population are different, these findings can not be compared with our study, vitamin levels were within normal limit in our study. We could not get exact comparable reference for our study so we have judged our data with most related studies. Looking into these facts, our data is comparable with above mention studies.
In preeclampsia there is elevated homocysteine injuries and abnormal vascular endothelium, which contribute to the pathogenesis of the preeclampsia. In addition, vascular endothelium in pregnant women may be more sensitive to homocysteine injury. Therefore moderate elevation of tHcy level compare to normal pregnant may lead to endothelial injury with subsequent activation of various factors that eventually results in preeclampsia 12.
Our studies demonstrate an increase in the homocysteine levels in patients with preeclampsia. In case of normal pregnancy there is conversion of spiral arteries from its highly tortuous thicken walled vessels to flaccid sinusoidal conduits of low resistance. The muscular coats of spiral arteries are retained in preeclampsia. They are now susceptible to maternal, humoral, and neuronal constrictor influences.
Clinical alarm is always late so to detect preeclampsia, thus laboratory plays an important role in such situation. So estimation of these biochemical parameters is useful to prevent preeclampsia thus reducing the undesired outcome in pregnancy. It was not possible to know the level of studied biomolecules in preconception or in early stage of
pregnancy. However further longitudinal interventional studies are required to know the cause of hyperhomocysteinemia as observed in pregnant women with preeclampsia with or without vitamin supplementation.
Reference
1. Singh U, Gupta HP, Singh RK, Shukla M, Singh R, Mehrotra SS, et al. A study of changes in homocysteine leels during normal pregnancy and pre-eclampsia. J Indian Med Assoc 2008; 106: 503-5.
2. Walker MC, Smith GN, Perkins SL, et al. Changes in homocysteine levels during normal pregnancy. Am J Obstet Gynecol 1999;180:660-4.
3. Powers RW, Evans RW, Majors AK et al. Plasma homocysteine concentration is increased in preeclampsia and associated with evidence of endothelial activation. Am J Obstet Gynecol 1998;179:1605-11
4. Hogg BB, Tamura T, Kelley E, et al. Second-trimester plasma homocysteine levels and pregnancy-induced hypertension, preeclampsia, and intrauterine growth restriction. Am J Obstet Gynecol 2000;183:805-9.
5. Ueland PM, Refsum H, Stabler SP et al. Total homocysteine in plasma or serum: methods and clinical applications. Clin Chem 1993;39:1764-79. 6. Refsum H, Ueland PM, Svardal AM. Fully
automated fluorescence assay for determining total homocysteine in plasma. Clin Chem 1989;35:1921–7.
7. Andersson A, Hultberg B, Brattstrom L, Isaksson A. Decreased serum homocysteine in pregnancy. Eur J Chem Clin Biochem 1992;30:377–9. 8. Lentz SR. Mechanisms of thrombosis in
hyperhomocysteinemia. Curr Opin Hematol 1998;5:343–9.
9. Grandone E, Margaglione M, Colaizzo D, et al. Factor V Leiden, C>T MTHFR polymorphism and genetic susceptibility to preeclampsia. Thromb Haemost 1997;77:1052–4.
10. Kanani PM, Sinkey CA, Browning RL, Allaman M, Knapp HR, Haynes WG. Role of oxidant stress in endothelial dysfunciton produced by experimental hyperhomocysteinaemia in humans. Circulation 1999; 100: 1161-8.
11. Welch GN, Loscalzo J. Homocysteine and atherothrombosis. N Engl J Med 1998; 338:1042- 50.
13. Mignini LE, Latthe PM, Villar J, Kilby MD, Carrolli G, Khan KS. Mapping the theories of Pre-eclampsia: the role of homocysteine. Obstet Gynecol 2005; 105: 411-25.
14. Noris M, Todeschini M, Cassis P, Pasta F cappellini A, Bonazzola S, Macconi D, Maucci R, Porrti F, Benigni A, Piccciolo C, Remuzzi G. L-arginine depletion in preeclampsia orient nitric oxide synthase toward oxidant species. Hypertention. 2004; 43: 614-22.
15. Roberts JM, Taylor RN, Musci TJ, Rodgers GM, Hubel CA, McLaughlim MK. Preeclampsia: an endothelial cell disorders. American Journal of Obstetrics and Gynecology. 1989; 161: 1200-1204.
16. Walsh SW. Maternal-placental interactions of oxidative stress and antioxidants in preeclampsia.
Semin Reprodective Endocrinology. 1998;16:93-104.
17. Benyo DF, Miles TM, Condrad KP. Hypoxia stimulates cytokines production by villous explants from human placenta. Journal of Clinical Endocrinology and Metabolism. 1997; 82: 1582-1588.