UNIVERSIDADE FEDERAL DO RIO GRANDE DO NORTE CENTRO DE CIÊNCIAS DA SAÚDE
PROGRAMA DE PÓS-GRADUAÇÃO EM CIÊNCIAS DA SAÚDE
ENSAIO CLÍNICO RANDOMIZADO SOBRE A PRÁTICA DA ATENÇÃO FARMACÊUTICA NAS FARMÁCIAS COMUNITÁRIAS
PATRÍCIA TRINDADE COSTA PAULO
ii
PATRICIA TRINDADE COSTA PAULO
ENSAIO CLÍNICO RANDOMIZADO SOBRE A PRÁTICA DA ATENÇÃO FARMACÊUTICA NAS FARMÁCIAS COMUNITÁRIAS
Orientadora: Profª Dr.ª Ivonete Batista de Araújo
Co-Orientador: Prof. Dr. Eryvaldo Sócrates Tabosa do Egito
NATAL – RN 2013
iii
Catalogação da Publicação na Fonte
Universidade Federal do Rio Grande do Norte - UFRN
Paulo, Patricia Trindade Costa.
Ensaio clínico randomizado sobre a prática da atenção farmacêutica nas farmácias comunitárias / Patricia Trindade Costa Paulo. - Natal, 2013.
76f: il.
Orientadora: Profa. Dra. Ivonete Batista de Araújo.
Co-Orientador: Prof. Dr. Eryvaldo Sócrates Tabosa do Egito. Tese apresentada ao Programa de Pós-Graduação em Ciências da Saúde da Universidade Federal do Rio Grande do Norte como requisito para a obtenção do título de Doutor em Ciências da Saúde.
1. Atenção farmacêutica - Tese. 2. Paciente diabético - Tese. 3. Farmácia comunitária - Tese. I. Araújo, Ivonete Batista de. II. Egito, Eryvaldo Sócrates Tabosa do. III. Título.
iv
MINISTÉRIO DA EDUCAÇÃO
UNIVERSIDADE FEDERAL DO RIO GRANDE DO NORTE CENTRO DE CIÊNCIAS DA SAÚDE
PROGRAMA DE PÓS-GRADUAÇÃO EM CIÊNCIAS DA SAÚDE
v
PATRÍCIA TRINDADE COSTA PAULO
ENSAIO CLÍNICO RANDOMIZADO SOBRE O IMPACTO DA ATENÇÃO FARMACÊUTICA NO ACOMPANHAMENTO DOS PACIENTES DIABÉTICOS NAS
FARMÁCIAS COMUNITÁRIAS
Aprovada em: 05/07/2013
Banca Examinadora:
Presidente da Banca: Prof.ª Dr.ª Ivonete Batista de Araújo
Membros da Banca: Prof. Dr. Aldo da Cunha Medeiros
Prof.ª Dr.ª Amália Cinthia Meneses do Rego
vi
DEDICATÓRIA
A Deus e aos meus pais,
José Ivo e Ednalva,
pela vida que me concederam.
A Nosman, esposo e companheiro;
aos meus filhos Marcello, Nosman Filho
vii
AGRADECIMENTOS
Expresso o meu estimável reconhecimento, as pessoas que contribuíram para a realização e éxito deste trabalho, em especial:
A Deus, luz que sustenta e guia a minha vida, semente de amor que me fortalece e Dom supremo que concede aos seus filhos, raciocínio, inteligência e compreensão para aprender e transmitir aos outros o aprendizado.
A Profª. Drª. Ivonete Batista de Oliveira, pela orientação, competência e por confiar no meu trabalho no desenvolvimento desta pesquisa.
Ao Prof. Dr. Eryvaldo Sócrates Tabosa do Egito, o meu reconhecimento pela pessoa que representa e o meu agradecimento pelo aceite inicial como orientanda e acompanhamento no desenvolvimento deste estudo.
Aos pacientes, voluntários masculinos e femininos anônimos, o meu eterno reconhecimento e caloroso agradecimento. Sem eles, este trabalho não seria realizado.
A minha amiga Palas Atenéia, o meu muito obrigada pela sua colaboração efetiva na realização desta pesquisa.
Ao colega farmacêutico Jailson Vilberto de S. e Silva pela sua incansável busca em prol da aprovação desta pesquisa junto a Secretaria de Saúde Municipal.
À Diretora do Laboratório de Análises Clínicas (LACEN) do município de João Pessoa –PB, Ranilda Clemente, pela sua disponibilização dos serviços laboratoriais para a realização dos exames bioquímicos necessários aos pacientes.
viii
A médica Verônica de Fátima Oliveira pela sua contribuição importante na avaliação clínica dos voluntários.
A Jackson e a todos os funcionários da Farmácia Popular do Brasil pela acolhida, apoio e colaboração aos pacientes selecionados.
À Universidade Estadual da Paraíba (UEPB), a Chefia do Departamento de Farmácia e aos seus professores, o meu agradecimento por concederem a minha liberação para cursar este Doutorado.
O meu reconhecimento e agradecimento a todos os professores deste Programa de Pós-Graduação, pela a construção deste aprendizado integral.
Aos funcionários do Programa de Pós-Graduação, o meu agradecimento.
Ao Prof. Dr. Paulo Medeiros, pela colaboração e contribuição importante nas análises estatísticas.
Aos colegas do Curso de Pós-Graduação, Rodrigo, Viviane, Karla, Dailton e outros pela amizade e companheirismo.
As minhas colegas de trabalho, Ana de Lourdes e Lilian pelo o incentivo e compreensão na realização desta pesquisa.
ix
“Vitórias fáceis são vitórias
baratas as únicas dignas,
de se ganhar,
são aquelas que vem como
resultado de uma dura LUTA”.
x
RESUMO
Introdução: A criação de programas de equipe multiprofissional de saúde desponta
como uma alternativa eficiente para controlar a evolução dos pacientes portadores de diabetes, e a inserção do farmacêutico em tais programas tem contribuído para melhorar o acompanhamento desses pacientes. Objetivo: Avaliar o impacto da intervenção do farmacêutico no acompanhamento dos pacientes diabéticos tipo 2, em farmácias comunitárias. Métodos: Ensaio clínico randomizado, uni-cego envolvendo 100 pacientes diabéticos tipo 2 de ambos os gêneros, usuários de farmácia comunitária, com idade igual ou superior a 30 anos, em uso de hipoglicemiantes orais com adição ou não de insulina e foram acompanhados por 6 meses. Os pacientes do grupo controle receberam o tratamento habitual existente em qualquer farmácia, e os de intervenção receberam o acompanhamento do farmacêutico incluindo intervenções aos problemas relacionados aos medicamentos. Os desfechos primários avaliados foram os valores da hemoglobina glicada (HbA1c), glicose basal e um questionário de qualidade de vida validado denominado de
Diabetes Quality of Life Measure (DQOL) - Brasil; e como desfechos secundários as
dosagens dos triglicérides, colesterol total, (HDL) colesterol, (LDL) colesterol, tensão arterial e a satisfação do usuário com o serviço prestado. Essa pesquisa contou com a colaboração de vários profissionais das diferentes áreas do conhecimento a seguir nominados: médico, farmacêutico bioquímico, enfermeiro, nutricionista e estatístico.
Resultados: Finalizaram o estudo 89 pacientes. Durante o acompanhamento 95,7%
xi
estatisticamente significantes quando comparados o final com o início do acompanhamento nos grupos de intervenção e controle. Conclusão: Os resultados indicam que as modificações das variáveis clínicas não apresentaram valores significativos no controle da enfermidade e comorbidades, enquanto que na avaliação da qualidade de vida os pacientes afirmaram que melhoraram; portanto, pode-se postular que a intervenção farmacêutica é uma atividade necessária, mas que a prática do Pharmaceutical Care trará benefícios com sustentabilidade para os pacientes se houver uma efetiva integração do farmacêutico numa equipe multiprofissional de saúde, o que está indisponível nas Farmácias Comunitárias.
xii
SUMÁRIO
1. INTRODUÇÃO ... 12
2. JUSTIFICATIVA ... 14
3. OBJETIVOS ... 15
3.1. Objetivo geral ... 15
3.2 Objetivos específicos ... 15
4. MÉTODOS ... 16
4.1 Critérios de Seleção de Pacientes... 16
4.2 Intervenções Realizadas ... 16
4.3 Medidas de Desfechos Utilizados ... 18
4.4 Tamanho Amostral ... 19
4.5 Processo de Randomização e Alocação ... 19
5.1 Artigo 1 ... 22
5.2 Article 2 ... 45
6. COMENTÁRIOS, CRÍTICAS E CONCLUSÕES ... 66
REFERÊNCIAS ... 68
APÊNDICES ... 70
Apêndice 1 ... 71
Apêndice 2 ... 72
ANEXOS ... 73
Anexo 1 ... 75
1. INTRODUÇÃO
As novas alternativas de tratamento promovem um aumento da sobrevida de indivíduos diabéticos que está diretamente proporcional ao aparecimento das complicações crônicas decorrentes dessa enfermidade, as quais estão associadas ao tempo de exposição à hiperglicemia1. Os procedimentos diagnósticos, terapêuticos, hospitalizações, absenteísmo, invalidez e morte elevam substancialmente os custos diretos e indiretos da assistência à saúde da população diabética. Sendo assim, um dos principais desafios para o sistema de saúde é prevenir ou minimizar essas complicações e desenvolver novas estratégias para retardar o seu aparecimento2.
Em termos mundiais, 135 milhões apresentaram a doença em 1995, 240 milhões em 2005 e há projeção para atingir 366 milhões em 2030, sendo que dois terços habitarão países em desenvolvimento3. No Brasil, a prevalência média nacional é de 9,5% e João Pessoa é 12ª capital com maior número de diabéticos (Fonte DATASUS/MS, 2009). Os custos diretos com diabetes mellitus variam entre 2,5% e 15% do orçamento anual da saúde, estimativas de custo para o Brasil oscilam em torno de 3,9 bilhões de dólares4.
Inserido numa variedade de programas assistenciais que trabalham a prevenção e o controle do diabetes, a assistência multiprofissional da equipe de saúde é uma alternativa para o tratamento desta enfermidade e de várias doenças crônicas. Alguns estudos relatam que os farmacêuticos podem contribuir com tais programas através de um acompanhamento farmacoterapêutico dos pacientes2,5. Foi descrito por Mino-León et al6 que o controle metabólico do portador de diabetes tipo 2 depende do cumprimento da prescrição e que os estudos de utilização de medicamentos são úteis para identificar os problemas relacionados com a adesão do paciente ao tratamento e portanto viabilizar as intervenções para corrigir o uso irracional dos medicamentos e contribuir para a melhoria da qualidade de vida do paciente.
medicamentosa com o propósito de alcançar resultados definidos, que melhorem a qualidade de vida do paciente”8.
A busca pela qualidade de vida tem se tornado evidente nos últimos anos, podendo se traduzir em benefícios fundamentais para a saúde da população. A avaliação da saúde relacionada à qualidade de vida é importante para mensurar o efeito de algum tratamento terapêutico, atualmente medido através de alguns instrumentos psicométricos estruturados e validados9.
Outra forma de avaliação da saúde considera os resultados humanísticos e, portanto, a qualidade das intervenções em torno do grau de satisfação do paciente. A satisfação é um parâmetro subjetivo que reflete também as preferências e expectativas dos pacientes com o serviço prestado, especialmente em aspectos técnicos e interpessoais, permitindo a avaliação do desempenho dos profissionais e os resultados com a saúde10.
Neste contexto, a atenção farmacêutica sugere que os farmacêuticos, como profissionais de saúde, assumam a responsabilidade pelos resultados terapêuticos, através da adoção de um papel ativo na gestão da atenção ao paciente, buscando controlar a enfermidade e melhorar a sua qualidade de vida11.
2. JUSTIFICATIVA
Considerando que os pacientes portadores de Diabetes Mellitus são continuamente polimedicados e que em virtude da singularidade biológica podem apresentar diferentes manifestações relacionadas com riscos e benefícios é necessário proporcionar um atendimento personalizado, de acordo com as necessidades de cada um, observando a natureza e duração do tratamento, via de administração dos medicamentos, sua posologia, seu regime de administração, possíveis efeitos adversos, interações medicamentosas, buscando garantir a eficácia e segurança desses pacientes.
3. OBJETIVOS
3.1. Objetivo geral
Avaliar o impacto da intervenção do farmacêutico no acompanhamento dos pacientes diabéticos tipo 2, em farmácias comunitárias.
3.2 Objetivos específicos
Avaliar os desfechos primários através dos valores da hemoglobina glicada (HbA1c), glicose basal e um questionário de qualidade de vida denominado de Diabetes Quality of Life Measure (DQOL) - Brasil;
Identificar os desfechos secundários medindo os valores de triglicérides, colesterol total, high density lipoprotein (HDL) colesterol, low density lipoprotein (LDL) colesterol e tensão arterial;
Medir a satisfação do usuário com o serviço prestado;
Evidenciar os grupos farmacológicos mais utilizados pelos pacientes de ambos os grupos de acompanhamento;
Quantificar, classificar e resolver os problemas relacionados com os medicamentos (PRM) que os pacientes apresentaram durante o estudo, de acordo com a metodologia proposta;
Avaliar a aceitação médica das intervenções realizadas e o índice de resoluções destas;
4. MÉTODOS
Ensaio clínico randomizado, controlado e uni-cego, realizado em duas unidades de farmácias comunitárias, em João Pessoa-PB, no período de setembro de 2009 a dezembro de 2011. Cada paciente foi acompanhado por 6 meses, recebendo atendimentos mensais, totalizando seis encontros.
4.1 Critérios de Seleção de Pacientes
A seleção dos pacientes ocorreu nas farmácias no momento da aquisição dos medicamentos. Os critérios de inclusão adotados foram: ter idade igual ou superior a 30 anos, ser portador de diabetes mellitus tipo 2, fazer uso de hipoglicemiantes orais com adição ou não de insulina e realizar os exames bioquímicos propostos no laboratório previamente determinado. Foram excluídos aqueles que tiveram doenças infectocontagiosas no decorrer da pesquisa, ou que faltaram três entrevistas consecutivas, ou que suspenderam os medicamentos hipoglicemiantes por ordem médica ou aqueles que não assinaram o Termo de Consentimento Livre e Esclarecido (TCLE). Este estudo foi aprovado pelo o Comitê de Ética em Pesquisa da Universidade Estadual da Paraíba sob o nº 0166.0.133.000-08 (ANEXO 1).
4.2 Intervenções Realizadas
Os encontros foram realizados para ambos os grupos; no grupo intervenção foi realizado o acompanhamento farmacoterapêutico baseado na metodologia Phamacotherapy WorKup7 adotada pelo Projeto de Atenção Farmacêutica de Minnesota (Minnesota Pharmaceutical Care Project) e aferidas as medidas de peso, altura e tensão arterial repetidas nos 6 encontros.
O grupo controle recebeu o tratamento habitual existente em qualquer farmácia e apenas foram acrescidas as aferições citadas anteriormente.
Posteriormente, era feita uma avaliação da história clínica e medicamentosa de cada paciente para detectar problemas relacionados com os medicamentos (PRM), e quando eram identificados, medidas resolutivas foram implementadas.
Os PRM foram classificados pela metodologia Pharmacotherapy Workup7 nos domínios de indicação (medicamento desnecessário e necessidade de medicamento adicional), efetividade (medicamento diferente é necessário, necessita de farmacoterapia sinérgica e dose baixa), segurança (reação adversa ao medicamento e dose alta) e adesão (paciente prefere não tomar o medicamento).
Quanto às intervenções foram divididas em resolutividade dos PRM, orientações farmacêuticas sobre o uso e armazenagem dos medicamentos e ações educativas para mudança no estilo de vida. Para resolver os PRM foram utilizadas reopções de horários, aconselhamento sobre adesão aos medicamentos e detecção das reações adversas. E para os problemas envolvendo o prescritor, o farmacêutico encaminhava uma carta ao médico por intermédio do paciente, que a levava na sua próxima consulta. Também foram feitos alguns encaminhamentos para o Programa Saúde da Família (PSF), na tentativa de agendar uma consulta com o endocrinologista, por meio do enfermeiro ou agente comunitário de saúde.
Em seguida, foi elaborado um plano de cuidados para cada paciente contendo informações relativas aos cuidados com a saúde e com os seus medicamentos. Este plano era acordado com o paciente, depois era registrado e documentado em fichas individuais e seu cumprimento era avaliado nos encontros posteriores.
As orientações farmacêuticas priorizavam o uso seguro e racional dos medicamentos, bem como a maneira correta de armazená-los. Aos pacientes foi entregue uma tabela com os horários organizados sobre como tomar os medicamentos, contendo figuras para auxiliar o entendimento.
Nas ações educativas, as tentativas para a resolução dos problemas de saúde foram direcionadas à modificação do estilo de vida, estímulo a uma alimentação saudável e incentivo à prática de atividade física. Foram entregues folders sobre a doença diabetes, guia alimentar para diabéticos, saúde do coração e o bom uso dos medicamentos.
4.3 Medidas de Desfechos Utilizados
Os desfechos primários adotados como critérios de avaliação foram os indicadores de HbA1c e glicose basal, estes foram realizados no início do acompanhamento, após 3 e 6 meses nos dois grupos. Os valores de referência para estes indicadores seguiram as recomendações da American Diabetes Association, 201118 .
Foi utilizado também como desfecho primário, a medida da qualidade de vida aferida pelo instrumento de avaliação Diabetes Quality of Life Measure (DQOL), um questionário validado em Português no Brasil19. Este é composto por 44 questões de múltipla escolha, organizadas em quatro domínios: satisfação (15), impacto (18), preocupação social/vocacional (7), preocupações relacionadas com a diabetes (4). A escala de medição do instrumento é do tipo Likert, numeradas de 1 a 5 de acordo com a intensidade da satisfação (1 - excelente satisfação, 2 - muito satisfeito, 3 - moderadamente satisfeito, 4 - pouco satisfeito, 5 - nada satisfeito), ou frequência (1 - nunca, 2 - quase nunca, 3 - às vezes, 4 - muitas vezes, 5 - sempre).
O DQOL-Brasil foi aplicado no início e após os 6 meses de acompanhamento nos dois grupos, por meio de autopreenchimento ou entrevista estruturada para pacientes com limitações de leitura ou escrita. Os farmacêuticos foram treinados para que mantivessem uma postura neutra durante o preenchimento do questionário, cooperando apenas para que os pacientes respondessem o total de perguntas.
Os desfechos secundários foram medidos através dos valores de triglicérides, colesterol total, high density lipoprotein (HDL) colesterol, low density lipoprotein
(LDL) colesterol e tensão arterial. Estes foram realizados no início do acompanhamento, após 3 e 6 meses nos dois grupos. Os valores de referência para o perfil lipídico foi de acordo com a IV–Diretriz Brasileira sobre Dislipidemias e Prevenção da Aterosclerose, 200720, e a tensão arterial conforme The Eighth Report
of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment
of High Blood Pressure-JNC8, 200921.
geral com o atendimento recebido. É formado por 14 perguntas numa escala de resposta composta por cinco alternativas (5 = sempre, 4 = quase sempre, 3 = às vezes, 2 = quase nunca, 1= nunca).
O preenchimento deste questionário foi realizado apenas no final do acompanhamento e respondido pelos pacientes isoladamente, sem a presença do farmacêutico pesquisador. Quando algum paciente apresentava limitações para responder, outro farmacêutico se apresentava com um diálogo franco e direto com ele, e aplicava o questionário deixando-o totalmente à vontade para respondê-lo. Nesta etapa, a correta participação do entrevistador minimizará suas interferências nos resultados do estudo. Por questões éticas, a confidencialidade das respostas foi mantida até o final do estudo, de modo que os questionários permaneceram anônimos, sendo revelados apenas na análise dos dados.
4.4 Tamanho Amostral
O tamanho amostral foi calculado para 100 pacientes (50 por grupo), para detectar uma redução de dois pontos percentuais da HbA1c, considerando um α=0,05, um β=0,2 e uma taxa de perdas de 10%24.
4.5 Processo de Randomização e Alocação
4.6 Análises Estatísticas
Para o tratamento estatístico foi utilizado o Programa Statistica 7.0. As variáveis quantitativas foram descritas como proporções e média ± desvio padrão.
Para avaliar a qualidade de vida e satisfação dos usuários foi utilizado o sistema R, versão 2.14.
Foram realizados testes de comparação de proporções e testes T de Student para populações independentes e para os casos de observações pareadas. Estabeleceram-se intervalos de 95% de confiança para médias e os testes de hipóteses foram realizados considerando significantes aqueles em que p-valor < 0,05.
5. ARTIGOS PRODUZIDOS
5.1
O artigo 1 - Randomized Trial of the Impact of Pharmaceutical Care on theHealth of Type 2 Diabetic Patients foi submetido no periódico Plos One que possui
fator de impacto 4.092 e Qualis A1 na classificação da CAPES para área Medicina II .
5.1 Artigo 1
Randomized Clinical Trial of the Impact of Pharmaceutical Care on the Health of Type 2 Diabetic Patients
Patricia Trindade C. Paulo, MSc¹,², Palas Atenéia D. Medeiros, Ph.D³, Rodrigo dos Santos Diniz, MSc1, Paulo Roberto M. Azevedo, PhD4, Eryvaldo Socrates T. Egito, PhD¹, Ivonete Batista Araujo, PhD¹*.
1Pós-Graduação em Ciências da Saúde, Universidade Federal do Rio Grande do
Norte, Natal-RN, Brasil.
2Departamento de Farmácia, Universidade Estadual da Paraíba (UEPB), Campina
Grande-PB, Brasil.
3Programa de Pós-Graduação em Saúde Pública, UEPB, Campina Grande/PB,
Brasil.
4Departamento de Estatística, Centro de Ciências Exatas e Tecnológicas,
Universidade Federal do Rio Grande do Norte, Natal-RN, Brasil.
Abstract
Objective - To evaluate the impact of Pharmaceutical Care practice on the health of type 2 diabetic patients in community pharmacies.
Methods - Randomized uni-blinded clinical test with 100 community pharmacy users:
type 2 diabetic patients of both genders, aged equal to or over 30 years, using oral hypoglycemic agents with or without addition of insulin and followed for 6 months. Patients were divided into control and intervention groups. The first group received the usual treatment. The second one had a monitoring program, performed by a pharmacist, which included evaluating the drug-related problems (DRPs). The primary outcomes evaluated were the values of HbA1c and fasting glycemic index. The secondary outcomes were the values of triglycerides, total cholesterol, high density lipoprotein (HDL) cholesterol, low density lipoprotein (LDL) cholesterol, and blood pressure.
Results - Eighty-nine patients concluded the study. During the follow-up, 95.7% of the patients from the intervention group presented DRPs (n=141), with an average of 3 events per patient. Among the DRPs, effectiveness was the category that revealed more cases with 34.1%. Concerning the studied pharmacological groups, oral hypoglycemic agents presented 35% of the DRPs. A resoluteness of 61.7% was achieved among those DRPs. The outcomes, for both groups, were not statistically significant when comparing the beginning and the end of the follow-up.
Conclusions - Our results reveal that the presence of only a pharmacist responsible
for a Pharmaceutical Care practice program is not enough to provide good results and to maintain the sustainability of such activities. Therefore, a multi-professional health care team is recommended to achieve the best results.
Trial Registration
Citation:Paulo PTC, Medeiros PAD, Diniz RS, Azevedo PRM, Egito EST, Araújo IB A Randomized Trial of the Impact of Pharmaceutical Care on the Health of Type 2 Diabetic Patients.
Copyright: © Paulo et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: This work was supported by the National Council of Technological and Scientific Development (CNPq) and the Coordination for the Improvement of Higher Education Personnel (CAPES). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Introduction
The technological advancements and new therapeutic alternatives still do not guarantee effective control of the exposure time to hyperglycemia, generating chronic complications and several consequences for patients with diabetes mellitus, especially because of the age of those individuals [1]. Therefore, one of the main challenges for the health care system is to develop new strategies to prevent and minimize these drawbacks or delay its appearance [2].
Programs with a multi-professional health care team are emerging as an efficient alternative to control the development of diabetes mellitus. The involvement of the pharmacist in such programs has contributed to improving the monitoring of these patients [3].
The metabolic control of diabetes mellitus depends on the compliance with the treatment. Therefore, studies about the correct use of drugs are useful to identify problems such as adherence to the treatment and to support interventions to improve the clinical development of the patient [4].
Some studies reveal that there is a high rate of morbidity and mortality related to the incorrect use of drugs in such patients. Pharmaceutical Care services can contribute to reducing these rates [5-6]. In 1990, Hepler and Strand proposed the practice of Pharmaceutical Care, creating methodologies to enable the "responsible provision of drug therapy as a way of achieving defined results, which improve the quality of life of the patient" [7].
Several reports related clinically significant results for HbA1c [3] with the practice of Pharmaceutical Care programs. This is true not only concerning the monitoring involving small groups of patients [8-9], but also in large non-randomized trials [10-11]. However, there is still a lack of information concerning the randomized practice of Pharmaceutical Care in community pharmacies and its influence on the public health system.
Methods
The protocol was approved by the Ethical Committee fromof the State University of Paraiba, Brazil. Written informed consent was obtained from all patients and controls.
This is a prospective randomized, controlled, and single-blind study performed at two community pharmacies in João Pessoa/Paraíba, Brazil, from September 2009 to December 2011. The patients, who were divided into two groups, were followed for 6 months, receiving monthly appointments.
Setting and Eligibility criteria for participants
The selection of patients was made at two pharmacies at the moment of their purchasing drugs. The adopted inclusion criteria were (i) to be equalor superior to 30 years of age, (ii) to be a patient with type 2 diabetes mellitus, (iii) to use oral hypoglycemic agents with or without addition of insulin, and (iv) to perform all the established biochemical tests to assure the clinical follow-up. The exclusion criteria were (i) to have an infectious disease during the study, (ii) to miss three consecutive appointments, (iii) to stop the use of the hypoglycemic drugs by order of the doctor, and (iv) to deny the acceptance of the term of free and informed consent (TFIC).
Interventions
During the monthly appointments, anthropometrical data, such as height and weight, and clinical data, such as blood pressure, were collected for both groups. However, for the intervention group, a pharmacotherapeutic follow-up based on the Pharmacotherapy Workup methodology, adopted by the Minnesota Pharmaceutical Care Project [7], was performed.
Aiming to detect drug-related problems (DRPs), an evaluation of the clinical history of each patient of the intervention group along with the patient’s drugs was performed by the principal investigator. In case of the existence of DRPs, a set of remedial actions were suggested and deployed to resolve them.
The DRPs were classified by the Pharmacotherapy Workup Methodology [12] as follows: (i) indication (unnecessary drug therapy and need additional drug), (ii) effectiveness (ineffective drug or dosage too low), (iii) safety (adverse drug reaction or dosage too high), and (iv) compliance (noncompliance).
On the other hand, the interventions were divided into (i) resoluteness of the DRP, (ii) pharmaceutical orientation on the use and storage of drugs, and (iii) educational activities to change lifestyle. To resolve the DRP options for adjustments of posology, counseling on medication adherence and detection of adverse reactions were used. Concerning problems involving the prescriber, the pharmacist forwarded a letter to the physician through the patient, who takes it at his/her next appointment. In an attempt to schedule a consultation with an endocrinologist, through the nurse or the healthcare agent, some appointments to the Family Health Program (FHP) were also made.
Afterwards, a plan of care containing information relating to their health care and medications was designed for each patient. The conception of this plan, which was made with full agreement of the patient, was kept in the patient’s individual records and the patient compliance with it was evaluated during the subsequent face-to-face meetings.
Outcomes
The primary outcomes evaluated were the values of HbA1c and fasting glycemic index. The secondary outcomes were the values of triglycerides, total cholesterol, high density lipoprotein (HDL) cholesterol, low density lipoprotein (LDL) cholesterol, and blood pressure. All exams were performed at the beginning of the study, and after 3 and 6 months in both the control group and intervention group. The reference values for HbA1c and fasting glycemic index followed the American Diabetes Association recommendations [13]. The blood pressure evaluation was based on The Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure - JNC8, 2009 [14], and the lipid profile according to the IV - Brazilian Guideline for Dyslipidemia and Atherosclerosis Prevention, 2007 [15].
Sample size
The sample size calculated to detect a reduction of two percentage points on the HbA1c of type 2 diabetes mellitus patients, considering anα = 0.05, a β = 0.2, and a loss rate of 10% [16] was 100 patients (n = 50 per group). Patients (n=100) were divided into two groups, the control group (n=50) and the intervention group (n=50).
Randomization e Allocation
Statistical Analysis
The statistical analysis was performed using the Statistic Program, Version 7.0 (Statsoft, Sao Paulo – Brazil). Quantitative variables were described as proportions and as average± standard deviation (SD). A confidence interval of 95% was established and results where p <0.05 were considered significant. Finally, the Student's T test was used to compare the averages.
Results
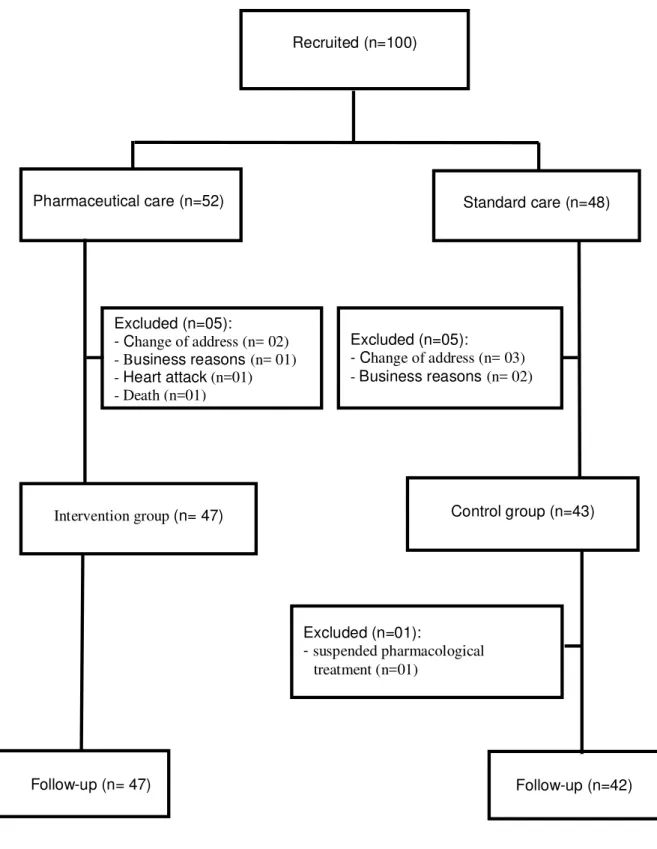
Only 89% (89/100) patients, among the 100 included on this study, completed it. Forty-seven patients belonged to the intervention group and 42 from the control group. Concerning the losses (n=10) and exclusions (n=1), 5 were from the intervention group, in which 2 patients had changed addresses, 1 reported a business reason, 1 had a heart attack and 1 died during the follow-up. The other 6 losses occurred in the Control Group, in which 3 patients had changed addresses, 3 reported business reasons, and 1 was excluded due to the suspending of the oral hypoglycemic by the doctor (Figure 1). In total, 562 pharmacist-patient face-to-face meetings were performed during the entire study.
Demographic and Biochemical Characteristics
The composition of the intervention group and the control group was 57.5% (27/47) women and 42.5% (20/47) men, and 52.4% (22/42) women and 47.6 % (20/42) men, respectively. The average age was 56.89 ± 10 years for the intervention group and 59.62 ± 9.0 years for the control group. Additionally, the IMC was 28.6 ± 3.8 and 27.6 ± 3.7 for the intervention group and the control group, respectively. Therefore, no significance (p<0.05) was found for these variables regarding these two groups.
patients in the intervention group had it detected at about 6 (6.8) years while the control group had it at around 7.2 ± 6.6 years.
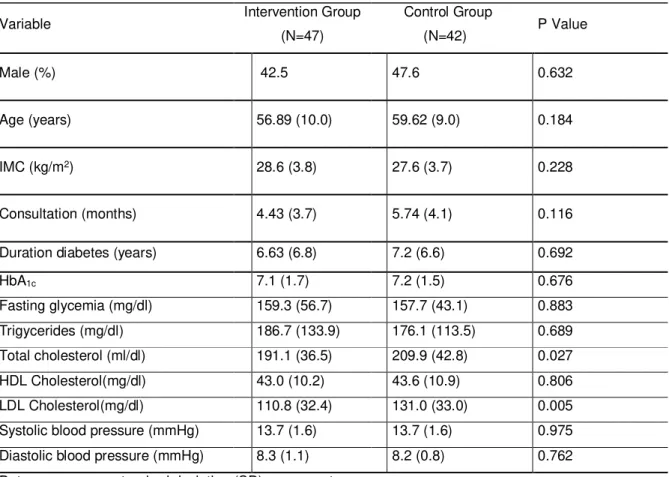
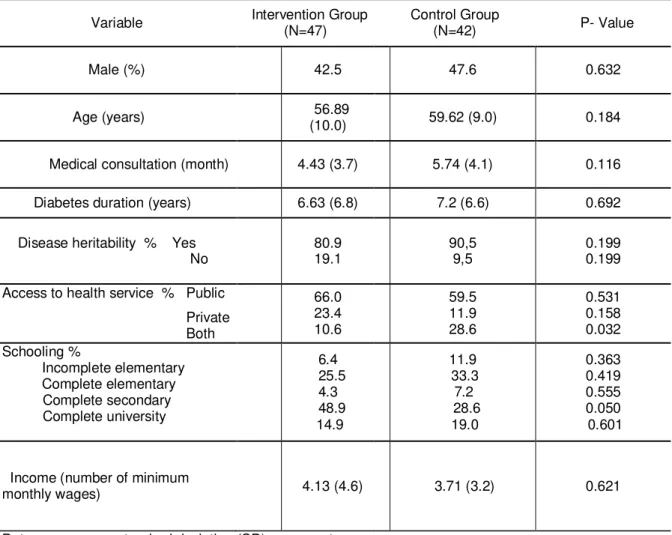
Concerning the clinical and metabolic characteristics, both groups of patients were very homogeneous (Table 1). Such similar profiles indicate that the intervention and control groups were a good fit for this kind of research.
Classification of the used drugs by the patients
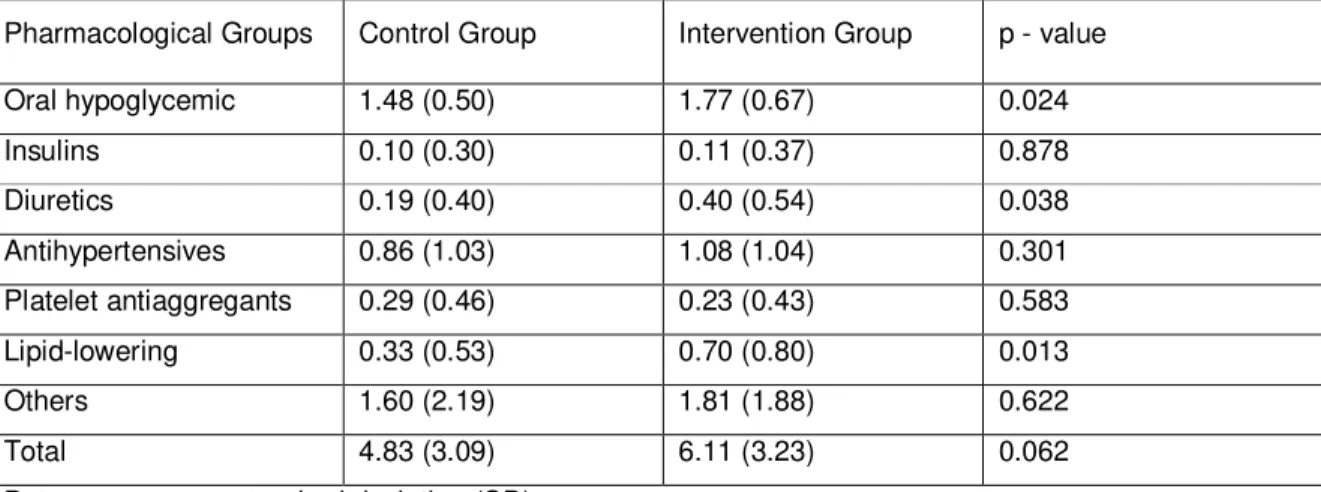
Table 2 describes the panel of drugs used to treat the type 2 diabetes mellitus and its comorbidities following the Anatomical Therapeutic Chemical (ATC) Classification. As it can be seen, the most used pharmacological groups were oral hypoglycemic agents (A10B), anti-hypertensive agents (C02), lipid-modifying agents (C10), and diuretics (C03). Three of them, hypoglycemic agents (A10B), lipid-modifying agents (C10), and diuretics (C03), presented high statistical significance when the quantitative evaluation of use was made between the control group and the intervention group.
The average number of drugs used by members of the intervention group was 6.11 ± 3.23, while for the control group this was 4.83 ± 3.09. However, this parameter was not statistically significant.
Drug-related problems (DRPs)
During the follow-up of the patients, 95.7% (45/47) from the intervention group presented DRPs, with an average of 3 events per patient, reaching a total of 141 DRPs. They were then classified into the following categories: indication 21.2% (30/141); effectiveness 34.1% (48/141); security 23.4% (33/141), and adherence 21.3% (30/141). The majority of the DRPs, 35% (49/141), were reported by the patients who used oral hypoglycemic agents (A10B) followed by the ones who used antihypertensive agents (C02), 18.4% (26/141); lipid modifying agents (C10),16.3% (23/141); and other groups, 30.03% (43/141). The resoluteness of the DRP occurred in 61.7% (87/141) of cases.
Non-pharmacological interventions
Some health problems (81) were detected in the patients during the initial exams. To resolve them, a pharmaceutical orientation procedure was carried out and some educational measures, such as encouraging the practice of physical exercise, healthful eating, and discontinuation of tobacco and alcohol, were adopted. At the end, 79% (64/81) of these cases were resolved, with confirmation in the subsequent exams.
Comparative evolution between both groups
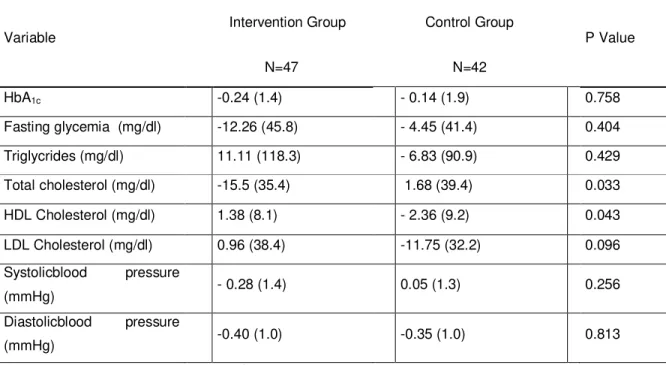
Patients were followed for a period of 6 months (180 days). Table 3 presents the average values of the biochemical variables and the differences between the beginning of the study and the 3rd month for both the control and the intervention groups. Not only HbA1c and fasting glycemia, the primary outcomes, but also the secondary outcomes such as the triglyceride values, LDL cholesterol, systolic blood pressure (SBP), and diastolic blood pressure (DBP) were not statistically significant. The only statistically significant difference was found between the total cholesterol and the HDL cholesterol.
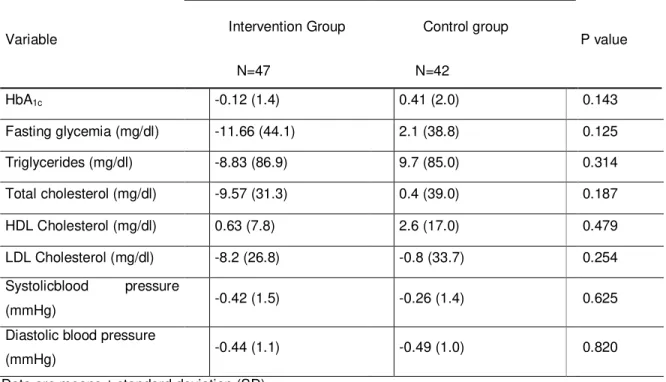
In the same way, the evaluation of the biochemical variables between the beginning of the study and the 6th month were not statistically significant for the primary and the secondary outcomes in both groups (Table 4). This result allows one to infer that the novelty of the service produced a motivation among patients seeking to improve their health, and as a result, the outcomes were quite promising in the first 3 months. However, after this period the patients became accommodated and no further development was observed on the clinical outcomes.
Discussion
similar to those found in other works [19-20]. Surprisingly, the study of Choe et al. [21] and Rao et al. [22] demonstrated a lower value of patient’s age and their IMC, while in the study of Fornos et al. [12] the patients presented an average age superior to the one found here. The large number of women who joined this study (Table 1) suggests that this gender attends the community pharmacies more often. A
similar result was evidenced in another study already published by Sarkadi et al. [23]. The average duration of diabetes in patients of this study was lower than that of
another study reported in the literature [3]. However, all these data did not interfere with the results of primary and secondary outcomes.
The clinical and metabolic control variables of the patients in both groups presented homogeneous at the beginning of the study. A slightly superior average HbA1c was observed in the control group, but this was not statistically significant. On the other hand, total cholesterol and LDL cholesterol also had elevated averages in the control group, and these were statistically significant. However, these differences did not hinder the comparison between both groups.
The researchers’ interventions did not significantly change the average number of drugs used by the patients (Table 2). This average was lower than that found in another study [24], although the use of oral hypoglycemic agents and insulin, in this research, were higher than in other studies of pharmaceutical intervention [10-25]. There was a greater use of medications in the intervention group than in the control group (Table 2), which was also seen in the study of Choe et al. [21]. This can be justified by the intervention performed for the resolution of the DRP and health problems detected during the monitoring process, since the patients were referred to a doctor for evaluation. Moreover, some of these problems were resolved with the addition of another medication. Furthermore, there were reports of significant reduction in the total number of medications used by patients at the end of the follow-up [26].
According to the consulted literature, due to cultural aspects, integration does not always happen between the pharmacist and the multidisciplinary health team. In fact, depending on the geographical location of the pharmacist, he or she has limited influence on prescribing decisions [2].
The mostly present DRPs were related to the effectiveness of drug treatment of the patient, which is in agreement with the results of Caballero et al. [29], followed by security, adherence, and indication of DRPs. This high incidence of ineffectiveness may be due to the poor essential infrastructure for medical care, creating a poor use of medications with dose, interval, and duration that were ineffective. However, other studies by Rao et al. [22] and Lyra-Jr. et al. [30] revealed a greater number of DRPs related to the adherence and the security, respectively. The acceptance rate of the referrals to doctors mentioned in this study was around 86%, the same percentage as described in the study by Fornos et al. [12], but differing from that obtained by Odegard et al. [31], who failed to achieve the same level of acceptance.
The content and length of pharmaceutical interventions are not equivalent in all studies, leading to achieve different results. For example, in the work of Sarkadi et al. [23], the pharmaceutical intervention consisted of education, advice on medications, insulin initiation, and adjustment on the basis of HbA1c and fasting glycemia. In another study [18] in which pharmaceutical interventions were compared to those of other professionals, pharmacists achieved better results in the metabolic control. In the present study, pharmaceutical researchers reviewed the values of metabolic variables and blood pressure, and evaluated the use of medications to detect DRPs and fix them through therapeutic recommendations to the doctor. Even when it was identified that non-pharmacological interventions had a problem-resolving rate of 79%, the variables such as HbA1c, fasting glycemia, lipid profile, and blood pressure remained without a statistically significant result. Although there are studies that claim otherwise [10-11], our study argues that the success of pharmacists monitoring of patients depends on their integration in a multi-professional health care team, which is in line with the study of Odegard et al. [31].
Another drawback that could be assigned to this study is that each selected pharmacy received members of both groups and an exchange of information between them could occur because the pharmacist interviewed sequentially patients in the intervention group and the control group. However, we believe that these facts did not produce significant effects, because each member received a standardized protocol, which was specific to each service group.
Conclusions
It is important to emphasize that the sale and dispensing of drugs should be the main activity of the Community Pharmacy. Of course, the Pharmaceutical Care practice using a multi-professional health care team would be a wonderful tool to provide the best service to the patients. However, this is a utopia in that the high cost of such strategy hampers this achievement. Our results reveal that the presence of only a pharmacist responsible for a Pharmaceutical Care practice program is not enough to provide good results and to maintain the sustainability of such activities.
Authors’ contributions
REFERENCES
1. Huckfeldt PJ, Meeker D, Peters A, Guterman JJ, Diaz Jr G, Goldman DP (2012) Diabetes management for low income patients in Los Angeles: Two strategies improved disease control in the short term. Health Affairs 31:. 168 -176
2. Silva-Castro MM, Valls LTI, Faus MJ (2010) Systematic review of the
implementation and evaluation of pharmaceutical care in hospitalised patients. Farmacia Hospitalaria 34:. 106−124
3. Clifford RM, Davis WA, Batty KT, Davis TME (2005) Effect of a pharmaceutical care program on vascular risk factors in type 2 diabetes: The Fremantle Diabetes Study. Diabetes Care 28:. 771-776
4. Mino-Léon D, Figueras A, Amato D, Laporte JR (2005) Treatment of type 2 diabetes in primary health care: a drug utilization study. Ann Pharmacother 39:. 441-445
5. Melchiors AC, Correr CJ, Venson R, Pontarolo R (2012) An analysis of quality of systematic reviews on pharmacist health interventions. Int J Clin Pharm 34:. 32-42 6. Sriram S, Chack LE, Ramasamy R, Ghasemi A, Ravi TK, Sabzghabaee AM (2011) Impact of pharmaceutical care on quality of life in patients with type 2 diabetes
Mellitus. J Res Med Science 16:. 412–S418
7. Hepler CD, Strand LM (1990) Opportunities and responsabilities in pharmaceutical care. Am J Hosp Pharm 47:. 533-543
8. Lyra Junior DP, Abriata JP, Amaral RT, Pelá IR (2005) Satisfacción como resultado de un programa de atención farmacéutica para pacientes ancianos en Ribeirão Preto - São Paulo (Brasil). Seguimiento Farmacoterapéutico 3:. 30-42 9. Lyra Junior DP, Rocha CE, Abriata JP, Gimenes FRE, Gonzales MM, Pelá IR (2007) Influence of Pharmaceutical Care intervention and communication skills on the improvement of pharmacotherapic outcomes with elderly brazilian outpatients. Patient Educ Couns 68:. 186-192
10. Correr CJ, Pontarolo R, Souza RAP, Venson R, Melchiors AC, Wiens A (2009) Effect of a Pharmaceutical Care Program on quality of life and satisfaction with pharmacy services in patients with type 2 diabetes mellitus. Braz J Pharm Sci 45:. 809-817
11. Correr CJ, Melchiors AC, Fernandez-Llimos F, Pontarolo R (2011) Effects of a pharmacotherapy follow-up in community pharmacies on type 2 diabetes patients in Brazil. Int J Clin Pharm 33:. 273-280
12. Cipolle RJ, Strand LM, Morley PC (2004). Pharmaceutical care practice: the clinician’s guide. New York: McGraw-Hill. 52-68
14. Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC8) (2009) Public Health Service: National Institutes of Health. National Heart, Lung, and Blood Institute of the USA
15. Brazilian Cardiology Association, Department of Atherosclerosis (2007) IV Brazilian Guidelines on Dyslipidemia and Atherosclerosis Prevention. Arq Bras de Cardiol 88:. 2-19
16.Fornos JA, Andrés NF, Andrés JC, Guerra MM, Ege B (2006) A pharmacotherapy follow-up program in patients with type-2 diabetes in community pharmacies in Spain. Pharm World Sci 28:. 65-72
17. Callegari J, Sidia M (2003) Bioestatística: Princípios e Aplicações. Porto Alegre: Artmed. 52p
18. Mehuys E, Van LB, Bolle L, Tongelen IV, Annemans L, Remon JP, Giri M (2011) Effectiveness of a community pharmacist intervention in diabetes care: a randomized controlled trial. J Clin Pharm Ther 36:. 602–613
19.Rothman RL, Malone R, Bryant B, Shintani AK, Crigler B, Dewalt DA, Dittus RS, Weinberger M, Pignone MP (2005) A randomized trial of a primary care-based disease management program to improve cardiovascular risk factors and glycated hemoglobin levels in patients with diabetes. Am J Med 118:. 276-284
20. Mino-Léon D, Reyes-Morales H, Jasso L, Doubova SV (2012) Physicians and pharmacists: collaboration to improve the quality of prescriptions in primary care in Mexico. Int J Clin Pharm 34:. 475–480
21. Choe HM, Mitrovich S, Dubay D, Hayward RA, Krein SL, Vijan S (2005) Proactive case management of high-risk patients with type 2 diabetes mellitus by a clinical pharmacist: A randomized controlled trial. J Manag Care Pharm 11:. 253-260 22. Rao D, Gilbert A, Strand LM, Cipolle RJ (2007) Drug therapy problems found in ambulatory patient populations in Minnesota and South Australia. Pharm World Sci 29:. 647–654
23. Sarkadi A, Veg A, Rosenqvist U (2005) The influence of participant's self-perceived role on metabolic outcomes in a diabetes group education program. Patient Educ Couns 58:. 137-145
24. Borgsteede SD, Westerman MJ, Kok IL, Meeuse JC, Vries TPGM, Hugtenburg JG (2011) Factors related to high and low levels of drug adherence according to patients with type 2 diabetes. Int J Clin Pharm 33:. 779–787
25. Kaae S, Sørensen EW, Nørgaard LS (2011) Exploring communications around medication review in community pharmacy. Int J Clin Pharm 33:. 529–536
hypertension: report of a double-bind clinical trial with ambulatory blood pressure. Am J Hypertens 19:. 528-533
27. Padiyara RS, D’Souza JJ, Rihani RS (2011) Clinical Pharmacist Intervention and the Proportion of Diabetes Patients Attaining Prevention Objectives in a
Multispecialty Medical Group. J Manag Care Pharm 17:. 456-462
28. Bremberg ER, Hising C, Nylen U, Ehrsson H, Eksborg S (2006) An evaluation of pharmacist contribution to an oncology ward in Swendish hospital. J Oncol Pharm Pract 12:. 75 – 81
29. Caballero SC, Torres JMM, Pérez MAC, Rio SG, Calleja HMA (2006) Problemas relacionados con los medicamentos en el área de observación de urgencias de un hospital de tercer nivel. Farmacia Hospitalaria 30:. 1130-1143
30. Lyra Junior DP, Kleir N, Abriata JP, Rocha CE, Santos CB, Pelá IR (2007) Impact of pharmaceutical care interventions in the identification and resolution of drug-related problems and on quality of life in a group of elderly outpatients in Ribeirão Preto (SP), Brazil. Ther Clin Risk Manag 3:. 989-998
31. Odegard PS, Goo A, Hummel J, Williams KL, Gray SL (2005) Caring for poorly controlled diabetes mellitus: A randomized pharmacist intervention. Ann
Table 1: Demographic and biochemical characteristics of the intervention and the control Group: preliminary data
Variable Intervention Group
(N=47)
Control Group
(N=42) P Value
Male (%) 42.5 47.6 0.632
Age (years) 56.89 (10.0) 59.62 (9.0) 0.184
IMC (kg/m2) 28.6 (3.8) 27.6 (3.7) 0.228
Consultation (months) 4.43 (3.7) 5.74 (4.1) 0.116
Duration diabetes (years) 6.63 (6.8) 7.2 (6.6) 0.692
HbA1c 7.1 (1.7) 7.2 (1.5) 0.676
Fasting glycemia (mg/dl) 159.3 (56.7) 157.7 (43.1) 0.883
Trigycerides (mg/dl) 186.7 (133.9) 176.1 (113.5) 0.689
Total cholesterol (ml/dl) 191.1 (36.5) 209.9 (42.8) 0.027
HDL Cholesterol(mg/dl) 43.0 (10.2) 43.6 (10.9) 0.806
LDL Cholesterol(mg/dl) 110.8 (32.4) 131.0 (33.0) 0.005
Systolic blood pressure (mmHg) 13.7 (1.6) 13.7 (1.6) 0.975
Diastolic blood pressure (mmHg) 8.3 (1.1) 8.2 (0.8) 0.762
Table 2: Average drug use by the patients of the intervention and the control group.
Pharmacological Groups Control Group Intervention Group p - value
Oral hypoglycemic 1.48 (0.50) 1.77 (0.67) 0.024
Insulins 0.10 (0.30) 0.11 (0.37) 0.878
Diuretics 0.19 (0.40) 0.40 (0.54) 0.038
Antihypertensives 0.86 (1.03) 1.08 (1.04) 0.301
Platelet antiaggregants 0.29 (0.46) 0.23 (0.43) 0.583
Lipid-lowering 0.33 (0.53) 0.70 (0.80) 0.013
Others 1.60 (2.19) 1.81 (1.88) 0.622
Total 4.83 (3.09) 6.11 (3.23) 0.062
Table 3: Statistical analysis of the differences among the biochemical data between the initial and the third month of evaluation
Average differences (third month-starter) in each patient
Variable Intervention Group Control Group P Value
N=47 N=42
HbA1c -0.24 (1.4) - 0.14 (1.9) 0.758
Fasting glycemia (mg/dl) -12.26 (45.8) - 4.45 (41.4) 0.404
Triglycrides (mg/dl) 11.11 (118.3) - 6.83 (90.9) 0.429
Total cholesterol (mg/dl) -15.5 (35.4) 1.68 (39.4) 0.033
HDL Cholesterol (mg/dl) 1.38 (8.1) - 2.36 (9.2) 0.043
LDL Cholesterol (mg/dl) 0.96 (38.4) -11.75 (32.2) 0.096
Systolicblood pressure
(mmHg) - 0.28 (1.4) 0.05 (1.3) 0.256
Diastolicblood pressure
(mmHg) -0.40 (1.0) -0.35 (1.0) 0.813
Table 4: Statistical analysis of the differences among the biochemical data between the initial and the sixth month of evaluation.
Average differences (final-initial) in each patient (DE)
Variable Intervention Group Control group P value
N=47 N=42
HbA1c -0.12 (1.4) 0.41 (2.0) 0.143
Fasting glycemia (mg/dl) -11.66 (44.1) 2.1 (38.8) 0.125
Triglycerides (mg/dl) -8.83 (86.9) 9.7 (85.0) 0.314
Total cholesterol (mg/dl) -9.57 (31.3) 0.4 (39.0) 0.187
HDL Cholesterol (mg/dl) 0.63 (7.8) 2.6 (17.0) 0.479
LDL Cholesterol (mg/dl) -8.2 (26.8) -0.8 (33.7) 0.254
Systolicblood pressure
(mmHg) -0.42 (1.5) -0.26 (1.4) 0.625
Diastolic blood pressure
(mmHg) -0.44 (1.1) -0.49 (1.0) 0.820
Supporting Information
Protocol S1.
O Pharmaceutical Care Influenciando na Qualidade de Vida dos Pacientes Diabéticos e sua Satisfação com o Serviço Prestado: Ensaio Clínico Randomizado. (DOC)
Checklist S1.
CONSORT 2010 checklist contained in the article.
Figura 1 - CONSORT 2010 Flow Diagram
Pharmaceutical care(n=52) Usual care (n=48)
Excluded (n=05):
- Change of address (n= 03) -Business reasons (n= 02)
Intervention group (n= 47) Control group (n=43)
Follow-up (n= 47)
Excluded (n=01):
- suspended pharmacological treatment (n=01)
Follow-up (n=42) Excluded (n=05):
- Change of address (n= 02) - Business reasons (n= 01) - Heart attack (n=01) - Death (n=01)
Section/Topic Item No CONSORT Checklist item Reported on page No Title and abstract
1a Identification as a randomised trial in the title √
1b Structured summary of trial design, methods, results, and conclusions (for specific guidance see CONSORT
for abstracts) √
Introduction
Background
and objectives 2a 2b Scientific background and explanation of rationale Specific objectives or hypotheses √√
Methods
Trial design 3a Description of trial design (such as parallel, factorial) including allocation ratio √
3b Important changes to methods after trial commencement (such as eligibility criteria), with reasons √
Participants 4a Eligibility criteria for participants √
4b Settings and locations where the data were collected √
Interventions 5 The interventions for each group with sufficient details to allow replication, including how and when they were
actually administered √
Outcomes 6a Completely defined pre-specified primary and secondary outcome measures, including how and when they
were assessed √
6b Any changes to trial outcomes after the trial commenced, with reasons √
Sample size 7a How sample size was determined √
7b When applicable, explanation of any interim analyses and stopping guidelines √
Randomisation: Sequence
generation 8a 8b Method used to generate the random allocation sequence Type of randomisation; details of any restriction (such as blocking and block size) √√ Allocation
concealment mechanism
9 Mechanism used to implement the random allocation sequence (such as sequentially numbered containers), describing any steps taken to conceal the sequence until interventions were assigned
√
Implementation 10 Who generated the random allocation sequence, who enrolled participants, and who assigned participants to interventions √ Blinding 11a If done, who was blinded after assignment to interventions (for example, participants, care providers, those
assessing outcomes) and how √ 11b If relevant, description of the similarity of interventions No Statistical
methods
12a Statistical methods used to compare groups for primary and secondary outcomes √
12b Methods for additional analyses, such as subgroup analyses and adjusted analyses √
Results
Participant flow (a diagram is strongly recommended)
13a For each group, the numbers of participants who were randomly assigned, received intended treatment, and
were analysed for the primary outcome √
13b For each group, losses and exclusions after randomisation, together with reasons √
Recruitment 14a Dates defining the periods of recruitment and follow-up √
14b Why the trial ended or was stopped √
Baseline data 15 A table showing baseline demographic and clinical characteristics for each group √
Numbers analysed
16 For each group, number of participants (denominator) included in each analysis and whether the analysis
was by original assigned groups No
Outcomes and
estimation 17a For each primary and secondary outcome, results for each group, and the estimated effect size and its precision (such as 95% confidence interval) √
17b For binary outcomes, presentation of both absolute and relative effect sizes is recommended √ Ancillary
analyses
18 Results of any other analyses performed, including subgroup analyses and adjusted analyses, distinguishing
pre-specified from exploratory √
Harms 19 All important harms or unintended effects in each group (for specific guidance see CONSORT for harms) √
Discussion
Limitations 20 Trial limitations, addressing sources of potential bias, imprecision, and, if relevant, multiplicity of analyses √
Generalisability 21 Generalisability (external validity, applicability) of the trial findings √
Interpretation 22 Interpretation consistent with results, balancing benefits and harms, and considering other relevant evidence √
Other information
Registration 23 Registration number and name of trial registry √
Protocol 24 Where the full trial protocol can be accessed, if available √
5.2 Article 2
Pharmaceutical Care Practice and consequences on quality of life and
satisfaction of diabetic patients: a randomized clinical trial
Patrícia Trindade C. Paulo1, Palas Atenéia D. de Medeiros2, Paulo Roberto M. de Azevedo3, Rodrigo dos Santos Diniz 4, Eryvaldo Sócrates T. do Egito5, Ivonete Batista de Araújo5
1Faculty of Pharmacy, State University of Paraiba, Campina Grande, Brazil.
2Postgraduate Collective Health Program, State University of Paraiba, Campina Grande, Brazil.
3 Department of Statistics, Federal University of Rio Grande do Norte, Natal, Brazil. 4 Postgraduate Health Science Program, Federal University of Rio Grande do Norte, Natal, Brazil.
5 Faculty of Pharmacy, Federal University of Rio Grande do Norte, Natal, Brazil.
ABSTRACT
Objective –
This study aimed at assessing the quality of life of patients with type 2 diabetes who received pharmaceutical care and their satisfaction with the service provided by Community Pharmacies.Methodology –
This is a single-blind, randomized controlled clinical trial involving 100 patients of both sexes with type 2 diabetes followed for 6 months. Control group patients received standard treatment while the intervention group was submitted to the pharmacotherapy workup process. The primary outcome was quality of life as measured by the Diabetes Quality of Life Measure (DQOL) questionnaire – Brazil and the secondary outcome was satisfaction with the service provided, using an instrument validated and translated into Portuguese.Results –
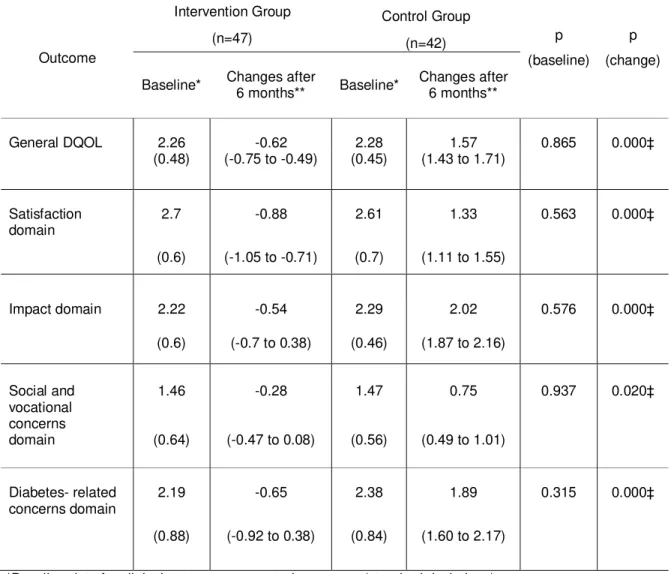
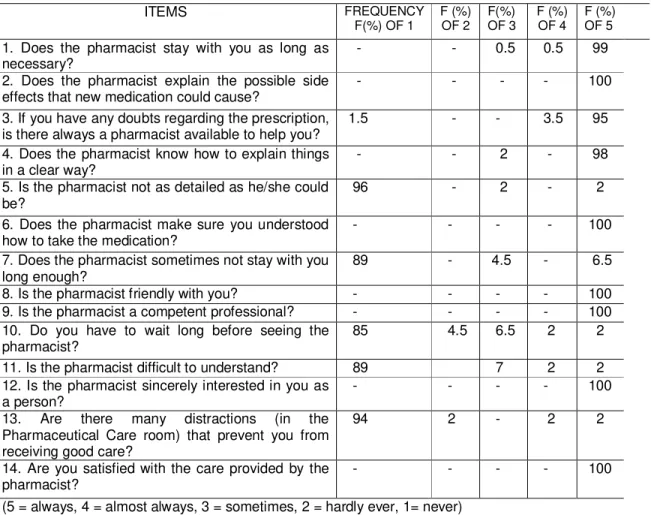
Statistically significant differences were observed between the intervention and control groups for total DQOL score (-0.62 vs 1.57 95% CI for p = 0.000) and in all domains assessed at the end of follow-up. The goal was reached in terms of patient satisfaction with the care provided, with 100% frequency in the 14 questions and final scores of 96%.Conclusion –
The advice provided by pharmacists in community pharmacies using Pharmaceutical Care practices resulted in higher quality of life and satisfaction levels. Thus, consolidating pharmaceutical advice activities is a professional and human commitment in our profession. Moreover, the practice complements prevention and health recovery measures for the population.Trial Registration
Reference:Paulo PTC, Medeiros PAD, Azevedo PRM, Diniz RS, Egito EST, Araújo IB. Pharmaceutical Care Influencing the Quality of Life of Diabetic Patients and their Satisfaction with the Service Provided: Randomized Clinical Trial.
Author’s rights: © Paulo et al. This is an open access article distributed under the
terms of the Creative Commons Attribution License, which allows unrestricted use, distribution and reproduction in any medium, provided the original author and source are referenced.
Financing: The authors received no financing or other support.
Introduction
The importance of quality of life (QOL)-related health and its value as a health outcome has evolved over the last 20 years [1]. The health-disease process has come to depend on external factors such as living, working, cultural and environmental conditions, among others [2].
The pursuit of quality of life, which has become evident in recent years, has translated into important health benefits for the population. Assessing quality of life-related health is vital in measuring the effect of therapy, currently measured using structured and validated psychometric instruments [3].
Another way of evaluating health considers the humanistic results and, therefore, the quality of interventions aimed at measuring the degree of patient satisfaction. Satisfaction is a subjective parameter that reflects patient preferences and expectations with the care provided, especially in terms of technical and interpersonal aspects, thereby allowing assessment of professional performance and health outcomes [4].
One of the practical activities by which pharmacists influence the health of patients is through the pharmaceutical care program. This was defined as “the responsible provision of drug therapy in order to obtain concrete results that improve the quality of life of patients” [5]. This definition suggests that in their capacity as health professionals, pharmacists assume responsibility for therapeutic results by playing an active role in patient care management, seeking to control infirmity and improve quality of life [6].
This strategy is more evident in the treatment of chronic diseases such as type 2 diabetes mellitus, due to its high prevalence and serious complications, which may lead to biological, psychological and social repercussions [7]. Possible health improvements should be measured using a suitable and sufficiently sensitive assessment instrument to reflect changes in quality of life over time [8].
Thus, the aim of the present study was to assess the quality of life of patients with type 2 diabetes who received pharmaceutical care and their satisfaction with the service received in Community Pharmacies.
Methods
The protocol for this trial and the CONSORT checklist, along with support information, are available. The study was approved by the Research Ethics Committee of the Paraiba State University-Brazil and registered in ClinicalTrials.gov under identifier NCT01580904.
This is a single blind randomized controlled clinical trial involving 100 patients with type 2 diabetes mellitus, at two Community Pharmacies in João Pessoa, Paraíba state, between September 2009 and December 2011. These facilities had the necessary infrastructure to develop the research, including an exclusive room for pharmacists to treat patients.
Patients who gave their informed consent were divided into two groups, both of which received monthly treatment, totaling six sessions for each patient. In the intervention group, the pharmacist conducted pharmacotherapy follow-up based on the Pharmacotherapy Workup adopted by the Minnesota Pharmaceutical Care Project [13], and the control group received standard treatment, with no added service.
Patient Selection Criteria
Interventions Used
Personal and clinical data, family history, life habits and clinical conditions were collected from the intervention group at the first session. Patients were also instructed to bring the medication they were currently taking. At the end of each session, they were given a card containing the date of the next meeting.
Afterwards, the clinical history and drug use of each patient were analyzed to determine whether there were any medication-related problems (MRP), and, when identified, an attempt was made to resolve and prevent potential MRPs.
The MRPs were classified according to Pharmacotherapy Workup methodology [13] in the following domains: indication (unnecessary medication or need for additional medication), effectiveness (different medication is required, need for low-dose synergic pharmacotherapy) safety (adverse reaction to high-low-dose medication) and adherence (patient prefers not to take medication).
Interventions were divided into MRP resolution, pharmaceutical advice and educational measures. To resolve MRPs medication times were changed, patients were encouraged to adhere to drug treatment and possible adverse reactions were resolved. In regard to problems involving the prescriber, the pharmacist sent a letter to the physician via the patient, who delivered it at the next meeting. A number of patients were referred to the Family Health Strategy (FHS to schedule an appointment with an endocrinologist through a community health agent or nurse. Next, a health care plan containing information on recommended practices and medication use was prepared for each patient. This plan was initially discussed and agreed upon with the patient, registered and documented on individual charts, and evaluated in successive meetings.
In educational measures, attempts to resolve health problems were directed towards changing lifestyle, stimulating healthy eating habits and encouraging physical activity. Pamphlets on diabetes, heart health, a food guide for diabetics, and the proper drug use were handed out.
Outcomes Assessed
As primary outcome the quality of life of patients was assessed and as secondary their satisfaction with pharmaceutical services.
Quality of life was measured by the Diabetes Quality of Life Measure(DQOL), a questionnaire validated in Brazil for Portuguese [8]. It is composed of 44 multiple-choice questions, divided into four domains: satisfaction (15 questions), impact (20), social/vocational concern (7), and diabetes-related concerns (4). A 5-point Likert scale was used to measure satisfaction (1 - excellent satisfaction, 2 – very satisfied, 3 – moderately satisfied, 4 – slightly satisfied, 5 – not satisfied), or frequency (1 - never, 2 – hardly ever, 3 - sometimes, 4 - frequently, 5 – always).
The DQOL-Brazil was applied at the onset and 6 months after follow-up in both groups, using a self-completion questionnaire or structured interview for patients with limited reading or writing skills. The pharmacists were trained to maintain a neutral stance during questionnaire completion, only encouraging patients to respond to every question.
With respect to satisfaction with the care provided, we used a structured instrument [14], translated and validated into Portuguese [15], composed of four dimensions: quality of advice, humanistic treatment on the part of the pharmacist, professional competence and pharmacotherapy management, in addition to overall satisfaction with the care received. It consists of 14 questions on a scale containing five alternatives (5 = always, 4 = almost always, 3 = sometimes, 2 = hardly ever, 1= never).
The questionnaire was completed at the end of follow-up without the presence of the research pharmacist. When patients found it difficult to respond, another pharmacist spoke with them to put them at ease and then left them to complete the questionnaire.
At this stage, appropriate participation by the interviewer will minimize interference in the study results. For ethical reasons, responses remained confidential and questionnaires were anonymous until the end of the study, at which time only data analysis was revealed.