ISSN 0976-2612, Online ISSN 2278–599X, Vol-7, Special Issue-Number4-June, 2016, pp854-864
http://www.bipublication.com
Case Report
Heart-Brain Coherence: the relationship between IHM Self-Regulation
Techniques and Heart Rate Variability (HRV) Biofeedback Training among
Iranian EFL Learners
Fatemeh Moussavi1 and Parviz Birjandi2* 1
Ph.D. Candidate in Applied Linguistics, Science and Research Branch, Islamic Azad University, Tehran, Iran
2Professor of Applied Linguistics, Science and Research Branch,
Islamic Azad University, Tehran, Iran
*Corresponding Author Email: [email protected]
ABSTRACT:
Drawing on psycho-physiological research emphasizing the importance of facilitating the emotion-cognition or heart-brain interaction through self-regulation techniques, the present study aimed at investigating the efficacy of heart rate variability (HRV) on heart-brain coherence through self-regulation techniques suggested by Institute of HeartMath. Sixty-three Iranian university students and high school students participated in this study. The TestEdge program was used to enable students to self-generate an optimal psycho-physiological state in order to increase HRV measures and heart-brain coherence. Running paired samples t-tests and Wilcoxon Signed Ranks tests, the results confirmed that the application of IHM self-regulation techniques significantly reduced the subjects’ low coherence ratio but increased the mid and high coherence ratio on the posttest than the pretest among subjects. Moreover, the subjects had a lower heart rate on the posttest than the pretest. These results indicated that utilizing IHM self-regulation techniques increased heart-brain coherence ratio.
Key words:Biofeedback; Heart-Brain Coherence; Heart-Rate Variability; Self-Regulation Techniques; TestEdge Program
1. INTRODUCTION
Historically, heart was referred to as the center of wisdom and emotionbydivine religions and some philosophers such as Aristotle and Avicenna. Furthermore, earlier studies (Cannon,1927; Lacey & Lacey, 1978) in addition to more recentMRI neuro-imagingfindings provide evidence that the heart transmits complex patterns of neurological, hormonal, and electromagnetic information to the brain(Ardell, 1994; Armour, 2007; Armour & Ardell, 2004; Armour & Kember, 2004; McCraty, 2003b) which form a major component of the physiological backdrop that ultimately determines our emotional experience (Appelhans, & Luecken,
2006; Armour, 2007; Bradley,
changes in our emotional states (McCraty,
Atkinson, Tiller, Rein,&
Watkins,1995).Therefore, the analysis of HRV is one of the most valuable tools in examining the interactions between heart and brain or heart-brain coherence.
2. Review of the related literature
2.1. Emotional factors in learning
Coleman (2008) defines Emotional Intelligenceas the ability to monitor and use emotional
information. Suggested byGould, Cameron,
Daniels, Woolley, and McEwen (1992), negative emotions cause reduction in cell proliferation in subgranular zone (SGZ) of the dentate gyrus in the hippocampus while antidepressant treatments increase it. In 2001 Shors and her collogues found some potential roles for the SGZ in cognitive development. Research in the new discipline of neurocardiology has confirmed that the heart acts as a sophisticated information encoding and processing center (Armour & Ardell, 2004) which is particularly sensitive to changes in emotional states (Tiller, McCraty, & Atkinson, 1996). Stressful situationsincrease HRV and decrease the function of corpus callosum and cerebral cortex (Wolpow, Johnson, Hertel, & Kincaid, 2011) which leads to heart-brain incoherence and deficiency in learning.
2.2. Theoretical basis of heart-brain interaction
From the social cognitive learning theory (Bandura, 1986), much of human learning occurs in a social environment; learners have an ability to influence their own self-beliefs which can affect their learning (Bandura, 2001). Learners are active participants in learning (Dornyei, 2005) and move from other regulation to self-regulationto control their learning (Lantolf, 2006). This is in accordance with research in psychophysiology and neurobiology which show that learning emotional regulation techniques significantly enhances attention, memory, comprehension, and reasoning (Bradley, et al., 2009; Schore, 1994). Many researchers (e.g. Erbe, 2007;Joseph, 2010;Stober, 2004; Laskey & Hetzel, 2010)
suggest different self-regulation strategies like positive thinking, relaxation, self-assessment,think aloud, and reciprocal teaching. Wolpow, et al. (2011) presents a six-category self-care plan (pp. 58-59)to prevent the negative consequences of bad feelings.Furthermore, it has been shown that heartplays a critical role in regulating the autonomic nervous system and affecting our emotional experience (Armour, 2007; Bradley, McCraty, Atkinson, Arguelles, & Rees, 2007; Bradley, et al. 2009; Bradley, et al., 2010; Childre, & Rozman, 2005; Kim, 2011). By biofeedback training, one learns to control heart rate or other physical or mental processes(McCraty, 2001). Based on research on psychophysiology of emotions and heart–brain coherence (Arguelles, McCraty, & Rees, 2003; McCraty, 2005; McCraty, Atkinson, Tomasino, & Bradley,2009; Tiller, et al., 1996), the Institute of HeartMath (IHM) has developed some tools and techniques focusing on heart intuition (perceive information outside our consciousness, Pearsall, 1999) and heart intelligence (respond to emotionally relevant information, McCraty & Rees, 2009) that teach students skills to self-regulate stress and other emotional learning impediments (Arguelles et al., 2003; Bradley et al., 2007; McCraty, 2005). Presenting electrophysiological evidence of heart intuition, McCraty et al. (2004) found we can intentionally experience certain positive feelings to advantageously affect our heart rhythm which is an important indicator of one’s capacity to adapt effectively to environmental demands. Dalton (2013) mentionsa variety of HRV applications such as regulating autonomic nervous system, synchronizing brain alpha rhythms with the heart, and cognitive development. Assessing HRV is a
useful measurement of psychophysiological
nervous system are out of sync with each other(Childre & Rozeman, 2005; McCraty, 2001, 2005, 2011; Reich, 2009).
2.3. Neurological basis of heart-brain interaction
Neurologists discovered that the “rhythmic beating patterns of the heart are transformed into neural impulses that directly affect the electrical activity of the higher brain centers” (Childre & Martin, 1999, p. 11). They discovered a neural pathway whereby input from the heart to the brain could either inhibit or facilitate the brain’s electrical activity.
This interrelationship is explained based on field theory and holographic principles by Laszlo (1995, p. 100) and also by Kafatos and Nadeau (1990, p. 185) applying systems theory. Based on
holographic principles, intuitive perception
accesses a field of energy into which information about future events is spectrally enfolded. One method of measuring the neurological heart-brain
interaction is analyzing HRV from
electrocardiograms. The normal HRV is due to the synergistic action of the two autonomic nervous system branches. Comprised of the TestEdge program and emWave technology, the IHM goal is training to monitor heart rhythmsin order to achieve low levels of stress and better performance. Focusing on positive emotions is the first intervention to increase heart-brain coherence by self-regulation techniques such as Cut-Thru (Childre & Rozman, 2002),Freeze-Frame, Heart Lock-In (McCraty & Childre, 2003), and Neutral Tool (Childre & Rozman, 2005). A software program, emWave Desktop,collects and translates HRV data into graphicsto show if physical, cognitive, and emotional systems are in sync or not.
3. The study
The primary goal of the present study was toinvestigate the relationship between IHM
self-regulation techniques and heart-brain
coherence.The following question was addressed:
1. Is there any significant relationship
between students’ HRV and their use of IHM self-regulation techniques?
4. METHODOLOGY
4.1. Participants
The participants were chosen from seven intact classes among 43 Iranian university students (male and female) and 20 female high school students.
4.2. Instruments
The following instruments were used:1) The Student Activity Guide (Novosel, 2012) to present the understanding of treatment, 2) an adapted form of the Self-Care Checklist (Wolpow, et al., 2011)to deal with anxiety, 3)IHM self-regulation techniques to facilitate managing emotions and pay attention to the area of the heart with an intentional positive emotion in order to change afferent cardiac input pattern sent to the brain,and4) an emWave Desktop device to record the participants’ HRV.
4.3. Procedure
Rozman, 2002). All was carried out via interactive modeling of the techniques.
To measure HRV, a pulse sensor plugged into USB of a computer was clipped to the earlobe of each student to collect and translate HRV patterns into graphics. The more coherence was achieved, the smoother and more wavelike heart rhythm patterns became. Furthermore, a tri-colored bar graph indicated the degree of attained coherence: low,medium, andhigh coherence.
To determine participants’ heart-brain coherence, coherence level ratio and average heart rate of participants were measured before and after treatment.
4.4. Materials
Reading materials were selected from passages of Mosaic1 (Wehmann & Knezevic, 2008). In order to have same grade reading difficulty of pre- and posttest passages, Fry Graph Readability Formula (1968) was used to provide the measure of the readability.
4.5. Data gathering
To depict electrophysiological coherence scores, the participants were seatedabout four to five feet apart from the researcher in order to minimize the possibility of HRV interference from one heart to another. The data were stored in a data-storage of emWave Desktop.
4.6. Design
The design of the present study was one comparisongroup pre/posttest design (Best & Kahn, 2006). The between-subject factors were coherence level ratio and average heart rate.
Self-regulation techniques were considered as
independent variables and HRVwas considered as dependent variable.
5. Data analysis and results
The data were analyzed using both parametric (paired-samples t-test) and non-parametric tests (Wilcoxon Signed Ranks Test).The first research question was decomposed into four minor questions because the heart rate variable was measured on a nominal scale while the coherence level ratios were percentages.
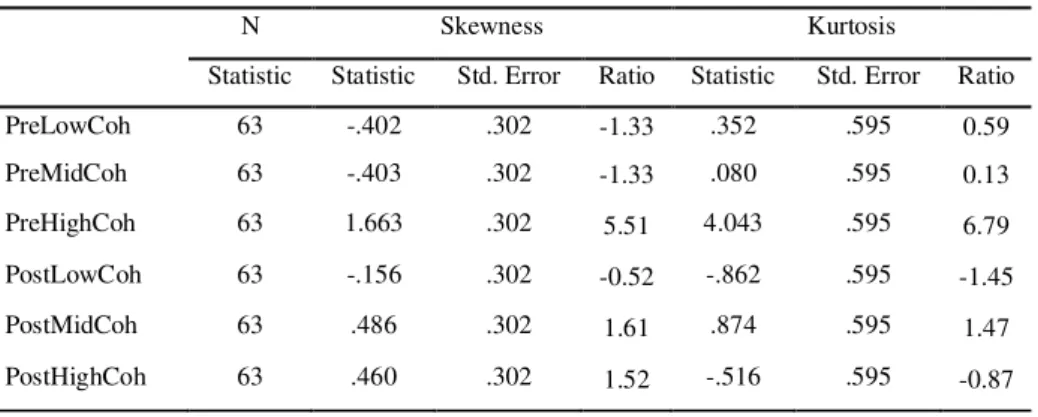
Moreover, the high, mid and low coherence level ratio could not be compared using a single analysis due to the fact that their total sum was 100.The normality of the data was checked. As displayed in Table 1, the ratios of skewness and kurtosis over their respective standard errors were all within the ranges of +/- 1.96 except for the pretest of high coherence ratio.
That is why the third minor null-hypothesis was analyzed using non-parametric Wilcoxon test.
Table 1. Testing Normality Assumption
N Skewness Kurtosis
Statistic Statistic Std. Error Ratio Statistic Std. Error Ratio
PreLowCoh 63 -.402 .302 -1.33 .352 .595 0.59
PreMidCoh 63 -.403 .302 -1.33 .080 .595 0.13
PreHighCoh 63 1.663 .302 5.51 4.043 .595 6.79
PostLowCoh 63 -.156 .302 -0.52 -.862 .595 -1.45
PostMidCoh 63 .486 .302 1.61 .874 .595 1.47
PostHighCoh 63 .460 .302 1.52 -.516 .595 -0.87
Note. Pre = pretest, Post = posttest and Coh = coherence ratio
5.1.1 Minor null-hypothesis 1-1
A paired samples t-test was run to compare the subjects’ low coherence ratio during the pretest and posttest. According to the results displayed in Table 2, the subjects had a lower low coherence ratio (M posttest =
Table 2. Paired Samples Statistics; Pretest and Posttest of Low Coherence Ratio
Mean N Std.
Deviation
Std. Error Mean Low Coherence
Level Ratio
Pretest 82.71 63 7.391 .931
Posttest 66.40 63 12.130 1.528
Figure 1: Means on Pretest and Posttest of Low Coherence Ratio
The results of paired-samples t-test (t (62) = 8.75, p = .000, r = .742 representing a large effect size) indicated that thelow coherence ratio level on the posttest was significantly lower. Thus the minor null-hypothesis 1-1 was rejected. The application of IHM self-regulation techniques reduced the subjects’ low coherence ratio significantly.
Table 3. Paired Samples Statistics; Pretest and Posttest of Low Coherence Ratio
Paired Differences
T Df Sig. (2-tailed) Mean Std. Deviation Std. Error Mean
95% Confidence Interval of the Difference
Lower Upper
16.317 14.795 1.864 12.591 20.044 8.754 62 .000
5.1.2 Minor null-hypothesis 1-2
To compare the subjects’ mid coherence ratio during the pretest and posttest, a paired samples t-test was run. Based on the results displayed in Table 4, after receiving IHM self-regulation techniques, they had a higher mid coherence ratio (M posttest = 16.48, SD = 5.66) compared with pretest (M pretest = 11.90, SD =
4.42).
Table 4. Paired Samples Statistics; Pretest and Posttest of Mid Coherence Ratio
Mean N Std.
Deviation
Std. Error Mean
Mid Coherence Level Ratio
Pretest 11.90 63 4.420 .557
Posttest 16.48 63 5.665 .714
Table 5. Paired Samples Statistics; Pretest and Posttest of Mid Coherence Ratio Paired Differences
T Df Sig. (2-tailed) Mean Std. Deviation Std. Error Mean
95% Confidence Interval of the Difference
Lower Upper
-4.571 7.321 .922 -6.415 -2.728 -4.956 62 .000
Figure 2: Means on Pretest and Posttest of Mid Coherence Ratio
5.1.3 Minor null-hypothesis 1-3
Based on the resultsof Wilcoxon Signed Ranks Test runon the subjests’ high coherence ratio (Table 6), the difference between pre and posttest had a higher positive mean rank (MR = 32.34). In other words, the subjects showed a higher high coherence ratio on the posttest than the pretest.
Table 6. Mean and Sum of Ranks; Pretest and Posttest of High Coherence Ratio
N Mean Rank Sum of Ranks
PostHighCoh – PreHighCoh
Negative Ranks 5a 16.00 80.00
Positive Ranks 56b 32.34 1811.00
Ties 2c
Total 63
a. PostHighCoh < PreHighCoh b. PostHighCoh > PreHighCoh c. PostHighCoh = PreHighCoh
Based on the results of the Wilcoxon test (Z= -6.21, p=.000, r= .858 indicating a large effect size), there was a significant difference between pre and posttest of high coherence ratio and subjects had a higher mean rank on posttest. Thus, the minor null-hypothesis 1-3 was rejected.
Table 7. Wilcoxon Signed Rank Test Statisticsa
PostHighCoh – PreHighCoh
Z -6.219b
Asymp. Sig. (2-tailed) .000
a. Wilcoxon Signed Ranks Test b. Based on negative ranks.
5.1.4 Minor null-hypothesis 1-4
A Wilcoxon Signed Ranks Test was run to compare the subjects’ average heart rate during the pretest and posttest. Based on the results displayed in Table 8 and Table 9, the subjects had a higher average heart rate on the pretest, i.e. the difference between pretest and posttest had a higher positive mean rank (MR = 35.79). It means there was a lower average heart rate of the subjects on the posttest than pretest.
Table 8. Mean and Sum of Ranks; Pretest and Posttest of Heart Ratio
N Mean Rank Sum of Ranks
PreAvHR – PostAvHR
Negative Ranks 13a 13.31 173.00
Positive Ranks 48b 35.79 1718.00
Ties 2c
Total 63
a. PreAvHR < PostAvHR b. PreAvHR > PostAvHR c. PreAvHR = PostAvHR
The results of the Wilcoxon test (Z = -5.55, p = .000, r = .766 representing a large effect size) and a lower mean rank on posttest indicated that there was a significant difference between the subjects’ heart rate on pretest and posttest. Thus the minor null-hypothesis 1-4 was rejected.
Table 9. Wilcoxon Signed Rank Test Statisticsa
PostHighCoh – PreHighCoh
Z -5.551b
Asymp. Sig. (2-tailed) .000
a. Wilcoxon Signed Ranks Test b. Based on negative ranks
Figure 4: Mean Ranks; Pretest and Posttest Average Heart Rate
6. DISCUSSION
Regarding the research question which
decomposed into four minor research questions, the results of paired-samples t-tests and Wilcoxon Signed Ranks Test indicated that the application of IHM self-regulation techniques reduced the subjects’ low coherence ratio significantly but it increased the mid and high coherence ratio
significantly among subjects on average.
Moreover, there was a significant difference between the subject’s heart rate on pretest and
posttest. They had a lower mean rank on posttest. As it mentioned before, heart rhythm coherence biofeedback has been used in various educational settings with excellent results. For instance, McCraty et al. (1999) found that at-risk middle school children who were taught emotional
self-management skills exhibited significant
HRV is a kind of parasympathetic control over the heart and “more parasympathetic input results in more variable intervals between heart beats, that is, higher HRV” (p. 275). They conclude that HRV measures could be a likely candidate to index self-regulatory capacity and activity because brain structures involved in self-regulation and those involved in autonomic nervous system regulation overlap considerably, particularly with regard to the prefrontal cortex. The results of their study confirmed the case; subjects making a higher level of self-regulatory effort had higher HRV measures than subjects with lower self-regulatory effort (Segerstrom & Nes, 2007). In a study involving 60 sixth through eighth grade students, Arguelles et al. (2003) found increased stress resiliency in the training group who had
practiced IHM regulation techniques in
comparison to the control group that did not learn the technique (p. 19). Findings have been shown to correlate directly with improvement in cognitive performance, increased attention and focus, improved emotional competence and classroom behaviors, and reduced perception of stress (McCraty et al., 2009; Tiller, McCraty, & Atkinson, 1996).
Moreover, according to Fabes and Eisenberg (1997, cited in Appelhans & Leucken, 2006), higher levels of resting respiratory sinus arrhythmia have been associated with greater self-reported emotion regulation and the use of constructive coping strategies in university students. They found that those with lower resting respiratory sinus arrhythmia experienced greater negative emotional arousal in response to stress, which interfered with their ability to implement adaptive regulative strategies. Other investigation, in a similar vein, revealed that HeartMath’s programs are effective in improving HRV and emotional stability (Arguelles et al., 2003; Bradley et al., 2007; Bradley et al., 2009; Bradley et al., 2010; Lloyd, Brett, & Wesnes, 2010; McCraty, 2003b, 2005, 2011; McCraty et al., 1999).The result of the present study is totally in line with the results of these studies.
7. CONCLUSION
The new understanding of the physiology of positive emotions and the key role played by the heart in the generation of emotional experience have exciting implications for higher-order thinking skills, learner readiness, decision making, and test-taking, as well as for social and emotional behavior. Accordingly, practical tools have been developed that enable students to self-regulate the physiological processes underlying effective learning and performance. The most obvious conclusion which can be drawn from the above mentioned studies and this study is that all have generally supported the premise that higher HRV measures reflect a greater capacity for regulated emotional responses.
REFERENCES
1. Appelhans, B. M., & Luecken, L. J. (2006). Heart rate variability as an index of regulated
emotional responding. Review of general
psychology, 10(3), 229-240.
2. Ardell, J. L. (1994). Anatomy and function of
mammalian intrinsic cardiac neurons. In JA.
3. Armour, & JL. Ardell (Eds.),
Neurocardiology (pp. 95–114). New York:
OUP.
4. Arguelles, L., McCraty, R., & Rees, R. A. (2003). The heart in holistic education.
Encounter: Education for meaning and social
justice, 16(3), 13-21.
5. Armour, J.A. (2007).The little brain on the
heart. Cleveland clinic Journal of
Medicine(74) 1, 848-851.
6. Armour, J. A. & Ardell J. L. (2004). Basic
and clinicalneurocardiology (Eds). New
York: OUP.
7. Armour, J. A. & Kember, G. C. (2004).
Cardiac sensory neurons. In JA. Armour, & J.
L. Ardell (Eds.), Basic and clinical
neurocardiology (pp.79–117). Oxford: OUP.
8. Bandura, A. (1986). Social foundations of
thought and action: A social cognitive theory.
9. Bandura, A. (2001). Social cognitive theory:
An agentic perspective. Annual Review of
Psychology, 52, 1–26.
10. Best, J. W., & kahn, J. V. (2006). Research in
education (10th ed.). Boston: Pearson Education,
Inc.
11. Bradley, R., McCraty, R., Atkinson, M.,
Arguelles, L., & Rees, R. (2007). Reducing test anxiety and improving test performance in America’s schools:Results from the test edge
national demonstration study. Boulder Creek,
CA: HeartMath ResearchCenter, Institute of HeartMath.
12. Bradley, R., Atkinson, M., Tomasino, D.,
Rees, R., & Galvin, P. (2009). Facilitating emotional self-regulation in preschool children: Efficacy of the early heart smarts program in promoting social, emotional and
cognitive development.
13. Boulder Creek, CA:HeartMath LLC.
14. Bradley, R., McCraty, R., Atkinson, M.,
Tomasino, D., Daugherty, A., & Arguelles, L.
(2010). Emotion self-regulation,
psychophysiological coherence, and test anxiety: Results from an experiment using
electrophysiological measures.
AppliedPsychophysiology &
Biofeedback,35(4), 261-283.
15. Cannon, W.B. (1927). The James-Lange theory
of emotions: A critical examination and an
alternative theory. The American Journal of
Psychology, 39, 106–124.
16. Childre, D. (1998). Freeze-Frame: A
scientifically proven technique for clear
decision making and improved health (2nd
ed.).
17. Boulder Creek, CA: PlanetaryPublications.
18. Childre, D., & Martin, H. (1999). The
HeartMath solution. San Francisco: Harper.
19. Childre, D., & Rozman, D. (2002).
Overcoming emotional chaos. San Diego, CA:
Jodere Group.
20. Childre, D., & Rozman, D. (2005).
Transforming stress: The heartmath solution
for relieving worry, fatigue, and tension.
Oakland, CA: New HarbingerPublications.
21. Coleman, A. (2008). A dictionary of
psychology (3rd ed.). Oxford: OUP.
22. Coleman, M., & Vaughn, S. (2000). Reading
interventions for students with
emotional/behavioral disorders. Behavioral
Disorders, 25, 93-105.
23. Dalton, M. S. (2013). Measures of heart rate variability and how they relate to age, gender,
emotional behavior, and academic
achievement in elementary school children in
Adventist and public schools. Unpublished
doctoral dissertation, La Sierra University, CA.
24. Dornyei, Z. (2005). The psychology of the
language learner: Individual differences in
second language acquisition. Mahwah, NJ:
Lawrence Erlbaum.
25. Erbe, B. (2007). Reducing test anxiety while increasing learning. College Teaching, 55 (3), 96-97.
26. Fry, E. B. (1968). A readability formula that
saves time. Journal of Reading, 11, 513–516.
27. Immordino-Yang, M. H., & Damasio, A.
(2007). We feel, therefore we learn: The relevance of affective and social
neuroscience to education. Mind, Brain,and
Education, 1(1), 3-10.
28. Joseph, N. (2010). Metacognition needed:
Teaching middle and high school students to develop strategic learning skills. Preventing
School Failure, 54(2), 99-103.
29. Kafatos, M., & Nadeau, R. (1990). The
conscious universe part and whole in modern
physical theory. New York: Sprinter-Verlag.
30. Kim, S. (2011). Heart rate variability
biofeedback and executive functioning in individuals with chronic traumatic brain
injury. Unpublished doctoraldissertation,
Yeshiva University, NY.
31. Lacey, J. I., & Lacey, B. C. (1978). Two-way
communication between the heart and the brain:Significance of time within the cardiac
32. Lantolf, J. (2006). Sociocultural theory and
L2. Studies in Second Language Acquisition,
28, 67-109.
33. Laskey, M. L., & Hetzel, C. S. (2010). Self regualted learning, metacognition and soft
skills: The 21st century learner. Online
submission to ERIC. (ERICDocument
Reproduction Service
34. No. ED511589.)
35. Laszlo, E. (1995). The interconnected
universe: Conceptual foundations of
transdisciplinary unified theory. Singapore:
World Scientific.
36. Lloyd, A., Brett, D., & Wesnes, K. (2010). Coherence training in children with attention deficit hyperactivity disorder: Cognitive
functions and behavioral changes. Alternative
Therapies in Health and Medicine, 16 (4),
34-42.
37. McCraty, R. (2001). Science of the heart.
Boulder Creek, CA: Institute of HeartMath.
38. McCraty, R. (2003a). Heart-brain
neurodynamics: The making of emotions. In D.
39. Childre , R. McCraty, & B. C. Wilson (Eds.),
Emotional sovereignty. Amsterdam: Harwood
Academic Publishers.
40. McCraty, R. (2003b).The scientific role of the
heart in learning and performance. Retrieved
from www.macquarieinstitute.com/scientific-
role-heart.
41. McCraty, R. (2004). The energetic heart:
Bioelectromagnetic communication within and between people. In P. J. Rosch & M. S.
Markov (Eds.), Clinicalapplications of
bioelectromagneticmedicine (pp. 541-562).
New York: Marcel Dekker.
42. McCraty, R. (2005). Enhancing emotional,
social, and academic learning with heart
rhythm coherence feedback. Biofeedback,
33(4), 130-134.
43. McCraty, R. (2011). Coherence: Bridging
personal, social and global health. Act Nerv
Super Rediviva, 53(3), 85–102.
44. McCraty, R., Atkinson, M., Tiller, W. A.,
Rein, G., & Watkins, A. D. (1995).The effects of emotions on short term heart rate variability
using power spectrum analysis. American
Journal of Cardiology, 76(14), 1089-1093.
45. McCraty, R., Atkinson, M., Tomasino, D.,
Goelitz, J., & Mayrovitz, H. N. (1999). The impact of an emotional self-management skills course on psychosocial functioning and autonomic recovery to stress in middle school
children. IntegrativePhysiological and
Behavioral Science, 34(4), 246-268.
46. McCraty, R., Atkinson, M., Tomasino, D., & Bradley, R. T. (2009). The coherent heart: Heart-brain interactions, psychophysiological coherence, and the emergence of system-wide order. IntegralReview, 5(2), 10-115.
47. McCraty, R., & Childre, D. (2003). The
appreciative heart: The psychophysiology of
positive emotions and optimal functioning.
Boulder Creek, CA: Institute ofHeartMath. 48. McCraty, R., & Rees, R. A. (2009). The
central role of the heart in generating and sustaining positive emotions. In C. R. Snyder
& S. J. Lopez (Eds.), The Oxfordhandbook of
positive psychology (pp. 527-534). Oxford,
UK: OUP.
49. Nelson, R. J., Benner, G. J., & Rogers-Adkinson, D. L. (2003). An investigation of the characteristics of k-12 students with co-morbid emotional disturbance and significant language deficits served in public school settings. Behavioral Disorders, 9 (1), 25-33.
50. Novosel, L. C. (2012). Emotions
self-regulation: A mixed-methods intervention study of socioemotional and reading outcomes of high school students with reading
difficulties. Unpublished doctoral dissertation,
University of Texas atAustin, Austin.
51. Pearsall, P. (1999). The heart's code: Tapping
the wisdom and power of our heart energy.
New York, NY: Random House: Broadway Books.
and mental and emotional self-management.
Unpublished doctoral dissertation, Institute of Integral Studies, San Francisco,California. 53. Segerstrom, S. C., & Nes, L. S. (2007). Heart
rate variability reflects self-regulatory
strength, effort, and fatigue. Psychological
Science, 18(3), 275-281.
54. Schore, A. N. (1994). Affect regulation and the origin of the self: The neurobiology of
emotional development. Hillsdale, New
Jersey: LawrenceErlbaum Associates.
55. Stober, J. (2004). Dimensions of test anxiety: Relations to ways of coping with pre-exam anxiety and uncertainty. Anxiety, Stress and
Coping, 17(3), 213-226.
56. Thayer, J. F., & Lane, R. D. (2009). Claude Bernard and the heart-brain connection:
Further elaboration of a model of
neurovisceral integration. Neuroscience &
BiobehavioralReviews, 33(2), 81-88.
57. Tiller, W. A., McCraty, R., & Atkinson, M.
(1996). Cardiac coherence: A new,
noninvasive measure of autonomic nervous
system order. AlternativeTherapies in Health
and Medicine, 2(1), 52-65.
58. Wehmann, B. & Knezevic, M. (2008).
Mosaic1. Berkshire: McGrawHill Education.
59. Wolpow, R., Johnson, M., Hertel, R., &
Kincaid, S. (2011). The heart of learning and
teaching: Compassion, resiliency, and
academic success (2nd ed.).Washington: