RADIATION PROTECTION – AN ISSUE OF KNOWLEDGE AND
TECHNIQUE IN DENTAL OFFICES
Mariana CONSTANTINIUC1, Daniela POPA2, Ana ISPAS2,
Alexandru BURDE2, Mihaela HEDEŞIU1
1Senior Lecturer, „Iuliu Haţieganu” University of Medicine and Pharmacy, Cluj-Napoca
2Univ. Assistant, PhD Student, „Iuliu Haţieganu” University of Medicine and Pharmacy, Cluj-Napoca Corresponding author: [email protected]
Abstract
Radiological examination is indispensable in current dental practice. Lately, dentists have become not only the beneiciaries of radiographic investigations required for diagnosis, but also their authors, as many dental ofices have been authorized to have X-ray machines and carry out radiological activity. This is why dentists who perform dental X-rays have the legal and moral obligation to possess thorough theoretical and practical knowledge about the radiological technique and also about their own and patients’ radiation protection. This study investigates to what extent medical practitioners providing dental radiology services know and apply the technical norms for work and patient protection.
Keywords: radiology, dentistry, protection measures.
1. INTRODUCTION
The importance of radiation protection measures derives from the harmful effects of radiation, which cause somatic changes and genetic mutations. These can be avoided by correctly performing radiographs and by reducing the number of radiographic examinations and, implicitly, unnecessary radiation exposure.
In developed countries, the number of dental radiological investigations represents 25.25% of all radio-diagnostic examinations performed worldwide [1,2].
In Romania, periodic reporting, to public
patient radiation doses among dental practitioners in Cluj county who attended postgraduate radiation protection courses.
2. MATERIALS AND METHOD
The theoretical knowledge of dentists providing dental radiology services was evaluated based on a questionnaire distributed to 78 dental practitioners.
The questionnaire included 28 questions referring to:
- recommendation of radiological examination (type of indicated X-rays and criterion of the recommendation, technique recommended for periapical X-rays, frequency of radiographic examinations in various disorders),
- radiation protection measures in the dental ofice (knowledge on the role of radiation protection, radiosensitive anatomical regions, radiation protection measures, type of ilms and collimator used).
The obtained data were centralized in an Excel 2010 table and were interpreted based on descriptive analysis.
Out of all persons who participated in the study, 21 dentists (58.33%) had a dental X-ray machine, 10 dentists (27.7%) had a panoramic X-ray machine, and 14 (38.8%) had no radiological equipment available, but had attended a radiation protection course. A ratio of 72.72% of the respondents had less than 10 years of dental practice experience.
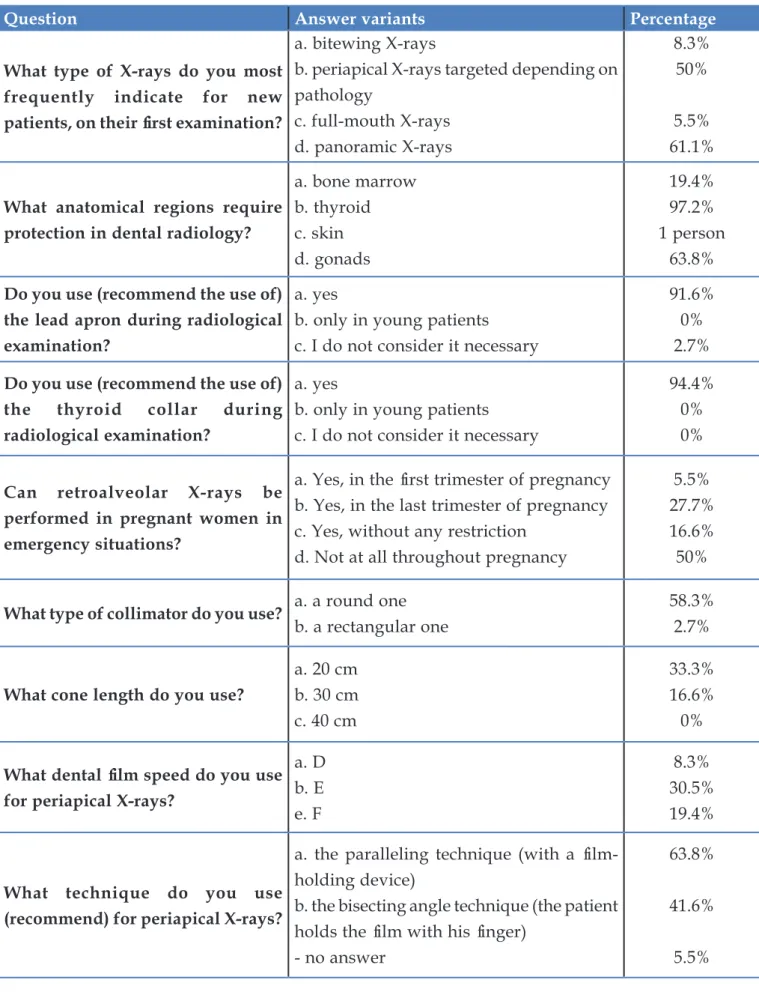
The X-rays most frequently indicated for new patients, on the first examination, were: panoramic X-rays (61.1%), followed by periapical X-rays (50%), bitewing X-rays (8.3%), and full mouth X-rays (5.5%).
Most of the dentists considered radiographic examination necessary irst for clinical diagnosis (66.6%), but other criteria were also taken into consideration, such as: the technical performance of the radiology laboratory (11.1%), patient’s inancial resources (8.3%), and the dificulties of technical execution (2.7%).
With respect to the anatomical regions requiring protection in dental radiology, the respondents considered the thyroid as the most important one (97.2%), followed by gonads (63.8%) and bone marrow (19.4%). For one respondent, skin was the most important element.
Out of the 36 persons who answered the questionnaire, two persons had no opinion about the use of the lead apron or thyroid collar. The ratio of those who answered afirmatively was
91.6% for the lead apron and 94.4% for the thyroid collar. One person considered the use of the lead apron as unnecessary when performing dental radiographs.
Regarding the performance of X-rays in pregnant women, 5.5% of the dentists considered this as possible in the irst trimester of pregnancy, and 27.7% - in the last trimester. On the other hand, 16.6% of them stated that radiographs could be performed without any restriction and 50% believed that they could not be performed at all during pregnancy.
According to this study, the ilms used in dental radiology services were mostly high-speed ilms, such as E-high-speed (30.5%) and F-high-speed ilms (19.4%), while slow-speed ilms, such as D-speed ilms, were used only in 8.3% of the cases.
The results of our study showed that 58.3% of the respondents used a round collimator and only 2.7% a rectangular one (Table 1).
16.6% of the respondents used a medium cone, most of them - 33.3% - used a short cone, and none used a long cone.
Table 1. Answers (as percentages) to the main questions
Question Answer variants Percentage
What type of X-rays do you most frequently indicate for new patients, on their irst examination?
a. bitewing X-rays
b. periapical X-rays targeted depending on pathology
c. full-mouth X-rays d. panoramic X-rays
8.3% 50%
5.5% 61.1%
What anatomical regions require protection in dental radiology?
a. bone marrow b. thyroid c. skin d. gonads
19.4% 97.2% 1 person
63.8%
Do you use (recommend the use of) the lead apron during radiological examination?
a. yes
b. only in young patients c. I do not consider it necessary
91.6% 0% 2.7%
Do you use (recommend the use of) the thyroid collar during radiological examination?
a. yes
b. only in young patients c. I do not consider it necessary
94.4% 0% 0%
Can retroalveolar X-rays be performed in pregnant women in emergency situations?
a. Yes, in the irst trimester of pregnancy b. Yes, in the last trimester of pregnancy c. Yes, without any restriction
d. Not at all throughout pregnancy
5.5% 27.7% 16.6% 50%
What type of collimator do you use? a. a round oneb. a rectangular one 58.3%2.7%
What cone length do you use?
a. 20 cm b. 30 cm c. 40 cm
33.3% 16.6% 0%
What dental ilm speed do you use for periapical X-rays?
a. D b. E e. F
4. DISCUSSION
The concept of patient radiation protection in dental medicine is based on three physical principles: the use of shields (usually of lead) for areas not to be exposed to radiation (particularly for radiosensitive organs), increased distance between the source of radiation and the target area, as well as reduction of the exposure time [1-3]. However, the most important radioprotection criterion includes justiied X-ray indication and reduction of unnecessary recommendations.
The advantages of digital radiology compared to conventional ilm-based radiology include the image acquisition speed, reduction of radiation exposure for both patients and medical staff, as well as elimination of ilm processing with chemical substances [4,5].
According to literature data, the increased use of digital systems compared to conventional radiology has resulted in a considerable reduction of the radiation doses (a 37% decrease in 2007) and has eliminated errors associated with manual ilm processing. In the future, further reduction of the radiation doses can be predicted by a gradual replacement of X-ray machines that still use manual processing with digital systems [6-8]. Replacement of D-speed ilms with E-speed ilms may reduce the radiation dose up to 50%. Utilization of F-speed ilms leads to a 20% decrease of the radiation dose compared to E-speed ilms. Studies on image quality have demonstrated that it does not affect the use of high speed ilms. However, dentists do not always choose the fastest receptor. Research carried out in various countries (Belgium, Turkey, Spain, Denmark, Finland) has shown a wider use of E-speed ilms. According to the authors of these studies, this is probably due to a wider commercial availability of these ilms [9]. Studies performed in Spain, which compared the radiation doses administered using digital systems in 2007 with those administered in 2002 (when conventional ilm-based X-ray machines were used), evidenced small differences. This demonstrates that replacement of the conventional system with the digital one involved, in many cases, only substitution of the ilm processor and
of the X-ray ilm cassette, while almost the same radiation dose was maintained. Dentists still use the same exposure time with the new digital systems as with the previous X-ray ilms, despite the possibilities offered by the new technology [10,11].
According to literature, the amount of radiation to which a person is exposed is 1.7 mGy in the case of a D-speed ilm and 1.3 mGy for an E-speed ilm, which means a 23% reduction of radiation exposure by the replacement of the D-speed with an E-speed ilm. Substitution of D-speed with E-speed ilms in dental radiology resulted in a 30-40% reduction of radiation exposure. The change from E-speed to F-speed ilms was associated with a 20-25% reduction of radiation exposure, and the cumulated effect of the change from D-speed to F-speed ilms was a 60% reduction of radiation exposure [12]. According to the results of our study, there is still an increased tendency to use E-speed ilms, despite the fact that using F-speed ilms would further reduce radiation exposure.
The limited use of rectangular collimation evidenced in our study represents about half of the percentages recorded in other countries (Belgium - 6%, Turkey - 5.5%, Canada - 8%), being 10 times less compared to the rates reported in Sweden (36%) [3,14,15]. This situation can be most probably attributed to the lack of knowledge on the effect of collimation and to the differences between the two types of collimators, an explanation deriving from the fact that almost half of the respondents did not wish or did not know how to answer this question. Using a rectangular collimator restricts the X-ray beam to the receptor area and can prevent unnecessary patient exposure. Replacement of a round collimator with a rectangular one results in an almost 60% reduction of the radiation dose [4,6,8,16].
To reduce patient exposure, the use of a long cone is recommended for increasing the distance between the radiation source and the target area. With the long cone, the X-ray beam will be less divergent and the amount of radiation and, implicitly, patient exposure will be diminished [4,16,17].
contradiction with the recommendations of specialists.
Some authors mention a higher number of leukemia cases in children whose mothers were exposed to radiological examinations during pregnancy, such as radiographic pelvimetry, by which the entire body of the fetus was exposed to high radiation doses. At the same time, an increased frequency of thyroid cancer is recorded in patients exposed to thymic irradiation during childhood, as well as a risk for intracranial meningioma following several dental X-rays [18,19].
Pregnant women should be particularly protected, with the complete avoidance or minimization of fetal radiation [20].
The relationship between dental radiation exposure during pregnancy and a low birth weight, even in the absence of fetal exposure, has been reported in the literature, but there is no mention of the organ whose radiation exposure is particularly responsible for this [21]. Experimental and epidemiological studies indicate that exposure of the thyroid gland might be responsible for this situation.
In our study, the responses regarding the performance of retroalveolar X-rays in pregnant women in emergency situations evidence the confusion of dentists with respect to this aspect. The incorrect opinions expressed could be due to the incomplete questions intentionally formulated in this way (in order to better check the knowledge of respondents), but also to the deicient knowledge in this area.
This shows the need for specialists performing dental X-rays to review their general knowledge of radiology, for adopting an adequate attitude on radiation protection.
The genetic effects of radiation consist of mutations whose number is directly proportional to the gonadal dose, regardless of the intensity of or the time period between exposures.
In most dental radiographic examinations, the thyroid gland is usually within the area exposed to radiation. There is an increased risk of thyroid cancer in the follicular epithelium after radiation exposure, women and children being predominantly predisposed. Because orthodontic treatment is more frequently requested in childhood, and cephalometric radiography is one of the most widely used radiological investigations before orthodontic treatment, it is vital to protect the thyroid gland during cephalometric exposure. The thyroid collar is the easiest and most effective modality to protect the thyroid from radiation [24,25].
The doses absorbed by the thyroid gland during a lateral cephalogram vary, according to different authors, between 5 and 57 μGy for one exposure. It was demonstrated that the use of a thyroid collar allowed a reduction ranging between 50% and 80% of the radiation dose absorbed by the thyroid after a cephalogram [5,24].
A comparison of the answers to the question regarding the radiological X-rays technique with those referring to the length of the cone used shows an obvious contradiction, leading to the conclusion that the respondents have no knowledge on the equipment, the projection technique, or both.
Possible answers to the questions did not include the option “I don’t know”. Therefore, the absence of an answer could be assimilated to the absence of knowledge on the respective issue. It should be noted that the absence of an answer was mostly related to questions referring to the type of collimator, cone length, and speed of the ilm used.
5. CONCLUSIONS
radiological examination they perform or request, for a correct evaluation of the risk-beneit ratio.
It can be concluded that neither the knowledge nor the behavior of dentists regarding safety standards in oral radiology is satisfactory.
By evidencing the current level of theoretical knowledge and the attitude towards radiation protection in oral medicine, the study suggests that more attention should be paid to this aspect, for reducing the exposure of patients to ionizing radiations.
References
1. Shahab S, Kavosi A, Nazarinia H, Mehralizadeh S, Mohammadpour M, Emami M. Compliance of
Iranian dentists with safety standards of
oral radiology. Dentomaxillofac
Radiol. 2012;41(2):159-64.
2. Syriopoulos K, Velders XL, vanderStelt PF, van Ginkel FC, Tsiklakis K. Mail survey of dental radiographic techniques and radiation doses in Greece. Dentomaxillofac Radiol. 1998;27(6):321–8. 3. Alcaraz M, Armero D, Martínez-Beneyto Y, Castillo
J, Benavente-García O, Fernandez H, Alcaraz-Saura M, CanterasAlternative X-ray ilters for an intra-oral digital radiographic system M. Chemical genoprotection: reducing biological damage to as low as reasonably achievable levels. Dentomaxillofac Radiol. 2011;40(5):310–4.
4. White SC, Pharoah MJ. Oral radiology:principles and interpretation (6th edn). St Louis, MO: Mosby; 2009. 5. Horner K. Review article: Radiation protection in
dental radiology. Br J Radiol. 1994;67(803):1041–9. 6. Geist JR, Katz JO. The use of radiation dose-reduction
techniques in the practices of dental faculty members. J Dent Education. 2002;66(6):697–702. 7. Alcaraz M, Navarro C, Vicente V, Canteras M. Dose
reduction of intraoral dental radiography in Spain. Dentomaxillofac Radiol. 2006;35(4):295–8. 8. Alcaraz M, Parra C, Martínez Beneyto Y, Velasco E,
Canteras M. Is it true that the radiation dose to which patients are exposed has decreased with modern radiographic films? Dentomaxillofac Radiol. 2009;38(2):92–7.
9. Alcaraz M, Velasco E, Martinez-Beneyto Y, Velasco F, Armero D, Parra C, Canteras M. The status of Spain’s dental practice following the European Union directive concerning radiological installations: 11 years on (1996-2007). Dentomaxillofac Radiol. 2010;39(8):468-74.
10. Gordon JC. Why switch to digital radiography? J Am Dent Assoc. 2004;135(10):1437–9.
11. Bohay RN, Kogon SL, Stephens RG. A survey of radiographic techniques and equipment used by a
sample of general dental practitioners. Oral Surg Oral Med Oral Pathol. 1994;78(6):806–10.
12. Syriopoulos K, Velders XL, Sanderink GCH, van Der Stelt PF. Sensitometric and clinical evaluation of a new F-speed dental X-ray ilm. Dentomaxillofac
Radiol. 2001;30(1):40–4.
13. Farman TT, Farman AG. Evaluation of a new F speed dental X-ray ilm. The effect of processing solutions and a comparison with D and E speed
ilms.Dentomaxillofac Radiol. 2000;29(1):41–5
14. Ilgüy D, Ilgüy M, Dinçer S, Bayirli G. Survey of dental radiological practice in Turkey. Dentomaxillofac Radiol. 2005;34(4):222–7.
15. Svenson B, Petersson A. Questionnaire survey on the use of dental X-ray film and equipment among general practitioners in the Swedish Public Dental
Health Service. Acta Odontol
Scand.1995;53(4):230–5.
16. Tugnait A, Clerehugh V, Hirschmann PN. Radiographic equipment and techniques used in general dental practice. A survey of general dental practitioners in England and Wales. J Dent. 2003;31(3):197–203.
17. Hintze H. Radiographic screening examination: frequency, equipment, and ilm in general dental practice in Denmark. Scand J Res. 1993;101(1):52–6.
18. Martínez-Beneyto Y, Alcaráz-Baños M, Pérez-Lajarín L, Rushton VE. Clinical justiication of dental radiology in adult patients: A review of the literature. Med Oral Patol Oral Cir Bucal. 2007;12(3):E244-51. 19. Philippe Hujoel, Lars G. Hollender. More than 5
full-mouth radiographic series increases intracranial meningioma risk. J Evid Based Dent Pract. 2005;5(3):162-3.
20. Glinoer D, Soto MF, Bourdoux P, Lejeune B, Delange F, Lemone M, Kinthaert J, Robijn C, Grun JP, de Nayer P. Pregnancy in patients with mild thyroid abnormalities: maternal and neonatal repercussions. J Clin Endocrinol Metab. 1991;73(2):421–7.
21. Hujoel PP, Bollen AM, Noonan CJ, del Anguila MA. Antepartum dental radiography and infant low birth weight. JAMA. 2004;291(16):1987–93 22. Horner K. Review article: radiation protection in
den tal radiology. Br J Radiol. 1994;67(803):1041-9. 23. Stecke J, Cruz AD, Almeida SM, Bóscolo FN.
Alternative X-ray ilters for an intra-oral digital
radiographic system. Dentomaxillofac
Radiol. 2012;41(5):361–6.
24. Sansare KP, Khanna V, Karjodkar F. Utility of thyroid collars in cephalometric radiography.
Dentomaxillofac Radiol. 2011;40(8):471–5.
25. Hujoel P, Hollender L, Bollen A-M, Young JD,
Cunha-Cruz J, McGee M, Grosso A. Thyroid shields