Department of Electronics and Instrumentation Engineering SASTRA University, Thanjavur. 613402, India.
S. Sundaram
Department of Electronics and Instrumentation Engineering SASTRA University, Thanjavur. 613402, India.
Abstract:
Sufferings associated with broken limbs have been on an exponential increase in India, mainly due to road accidents. Conventional healing and uniting methods takes any where between 1 ½ to 6 months depending on the nature of the fracture and the speed of reporting for medical care .In an effort to speed up the healing process low voltage electric stimulation has been tried and has been found to cut down the healing time by nearly 30% depending on the fracture-history. Also the course of fracture healing has been traced and definite trends during the process identified. Two case studies of fractures of the leg bone through electric stimulation indicate identical trends in the healing process.
Key words:
Fracture healing, Monitoring, Electric Stimulation, Low voltage,Process,Legbone
1.Introduction
The drastic increase in the road accidents due to vast expansion of the automobile industry has resulted in large scale fractures incidence posing a great challenge to an orthopaedic surgeon. The conventional methods of tracing the history of fracture healing like xrays, ultrasound, Quantitative CT, Triphase Radio Isotope bone scan does not in anyway accelerate the healing process (1-4). Several workers have indicated that electric field speeds up fracture healing especially in the long bone fractures (5-13). An earlier work has made a preliminary study on the effect of electric stimulation on fracture patients (14). The present work makes a detailed analysis of the course of fracture and demarcates various stages in the process of fracture healing.
2.Experimental-setup-for electric stimulation and recording
Figure 1 Steel, Carbon Fixator, and Patient with Carbon ring
3. Methodology
In this experimental study 2 male patients with tibia fracture were stabilized using carbon Ilizaro external fixator. They were mobilized with partial to full weight bearing in the immediate postoperative period as allowed by the patient’s pain tolerance. The upper wire of the fracture was given a direct current up to 1 V and the output was recorded across the fracture in the lower wire. The stay wires that passes only through the tibia was taken into consideration. and those wires that have purchase in fibula were avoided Figure 2 shows real time experimental recording and schematic diagram
Figure 2 Experimental set up of the assembly.
4 Results and discussion 4.1.1 Patient-1
This patient presented 3 months after a debridement and a rod type fixator application for an open an oblique irregular fracture of the middle third of leg as seen in Figure 3. His fixator pin sites got infected and it was removed and the carbon fixator was applied . Figure 3 shows response for 0.1 to 1.0 V D.C input. The maximum current flow was recorded in the 2nd week coinciding with the start of the osteoblastic action (the cells that produce new bone in the fracture site) from that time. Here the stabilization of current flow occurred on the 45th day indicating a delay in new bone formation and healing due to infection, and high energy injury. The dynamization to induce for new bone formation caused a reduction in conduction from the 75th day onwards as seen in Figure 3. The curve touched the lowest level on 98 day, correlating with the clinical and radiological union and the rings were removed after 130 days.
RING
FIXATOR
AMMETER
POWER
SUPPLY
0 200 400 600 800 1000 1200
0 20 40 60 80 100 120
No of Days
Cu
rr
e
n
t in
m
A
0.1 V 0.2V 0.3V 0.4 V 0.5 V 0.6 V 07 V 0.8 V
Figure 3 Fracture, Carbon fixator and Output response for Tibia fracture for patient 1
4.1.2 Patient 2
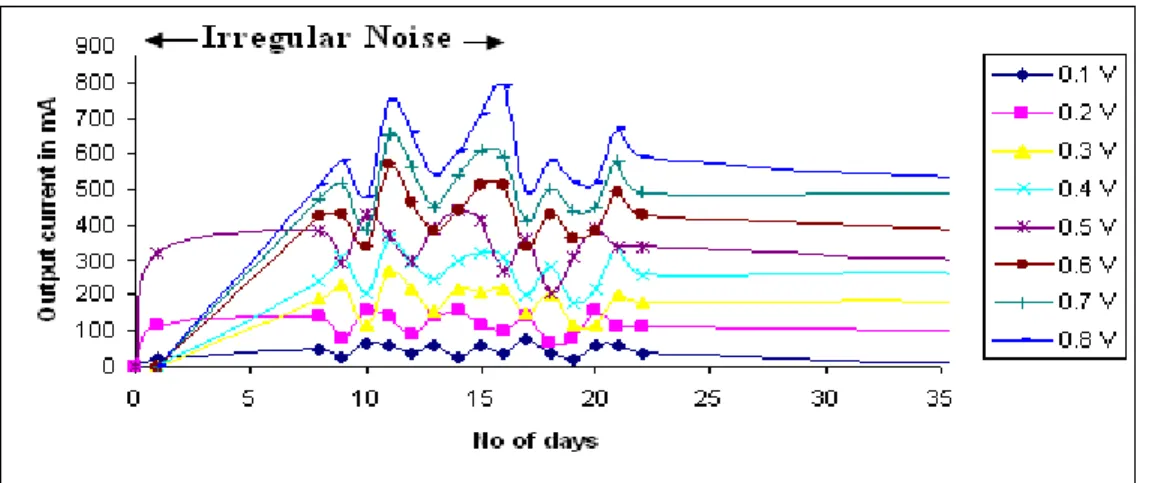
Figure 4 Fracture, Carbon fixator and Output response for Tibia fracture for patient 2
The process of fracture healing as indicated by the amount of current flow in mA for various DC voltages ranging from 0.1 to 0.8V are shown in the figures 3 and 4 as a function of time for patients 1 and 2 respectively. The following observations are seen for both the cases. Patient 1 reported after 3 months while patient 2 was admitted on the day of fracture. It is observed in the case of patient 2 that up to 15days there was irregular peaks as also reported by Bauke W.Kooistra et al (16). Comparing patients 1 and 2 after the cessation of noise signal in patient 2, the following observations are made. First peak is on the 9th to 10th day indicating osteogenesis. Second peak on the 28-32 day showing the period of formation of immature callus (Soft bone formation ).A downward trend thereafter upto about 40 days indicating ossification. After 40 days a horizontal line showing no further variation in current is an indication of complete healing. The various stages indicated by peaks were confirmed by X-rays . A few more cases are being studied to establish a healing pattern graph which can in future help in avoiding x-rays for analysis.
Conclusions
Monitoring of fracture healing using electric stimulation was done for two open fractures. The DC voltage 0.1 to 1V was given for both the patients. The output was recorded and compared with xrays taken concurrently. Based on the response the following conclusions were arrived. It was observed from the x-rays the fractures were radio logically healed and in the same time the current also was seen stabilized in the response curve. There is a definite inference that the current stabilizes after the initiation of the healing process .This stabilization depends on the delay in the start of the treatment and also the comminution of the fracture and presence of infection.
References:
[1] Text book of Orthopaedics and Trauma by G.S.Kulkarni Page 1506-7, First edition 1999.
[2] Dr.T.S.Keshwar ,DRP,PhD,DSc, and Dr Sushmita Goshal MD,Short and long term effects of radiation exposure. pages 118-138 –from the proceedings of International conference on radiological protection of patients in medical application of ionizing radiation. March 22-23-2002,department of nuclear medicine ,SGPGIMS,Lucknow.
[3] Chris J Harvey -Principles of radiology- -© 2008 Elsevier Ltd. pp 235 -238
[4] De Deyne PG ,Kirsch-Volders M -.In vitro effects of therapeutic ultrasound on the nucleus of human fibroblasts - J. Phys ther ,Vol. 75, No. 7, July 1995, pp. 629-634
[5] Chakkalakal D.A., Lippiello L., Shindell R.L., and Connolly J.F. (1990) Electrophysiology of direct current stimulation of fracture healing in canine radius. IEEE Trans. Biomed. Eng 37, 1048-1058.
[6] Cho M.R., Thatte H.S., Lee R.C., and Golan D.E. (2000) Integrin-dependent human macrophage migration induced by oscillatory electrical stimulation. Ann. Biomed. Eng 28, 234-243.
[7] Clinical effects of electromagnetic and electric fields on fracture healing-James T Ryaby.-Clinical Orthopaedics and Related Research – number 355S(supplement),PP S205-S 215(1998).
[8] Cheng K., Tarjan P.P., and Mertz P.M. (1993) Theoretical study of rectangular pulse electrical stimulation (RPES) onskin cells (in vivo) under conforming electrodes. Biomed. Sci. Instrum. 29, 349-354
[9] Chang W.H., Hwang I.M., and Liu H.C. (1991) Enhancement of fracture healing by specific pulsed capacitively-coupled electric field stimulation. Front Med. Biol. Eng 3, 57-64 .
[10] Chakkalakal D.A., Lippiello L, Wilson R.F., Shindell R., and Connolly J.F. (1990) Mineral and matrix contributions to rigidity in fracture healing. J. Biomech. 23, 425-434.