Qualidade de vida em pacientes com vertigem posicional paroxística benigna e/ou doença de Ménière
Texto
Imagem
Documentos relacionados
The probability of attending school four our group of interest in this region increased by 6.5 percentage points after the expansion of the Bolsa Família program in 2007 and
I could propose that all of these, perhaps with the exception of the last one, relate to preserving or enhancing the quality of life, or at least that aspect of it that relates
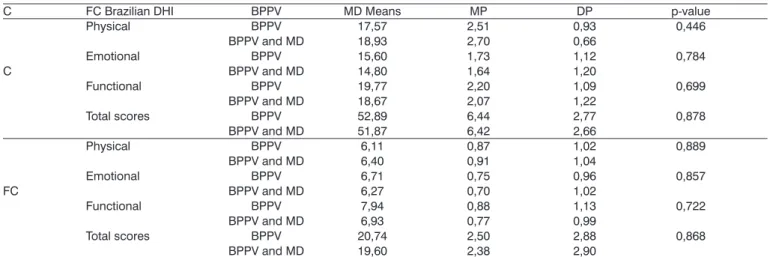
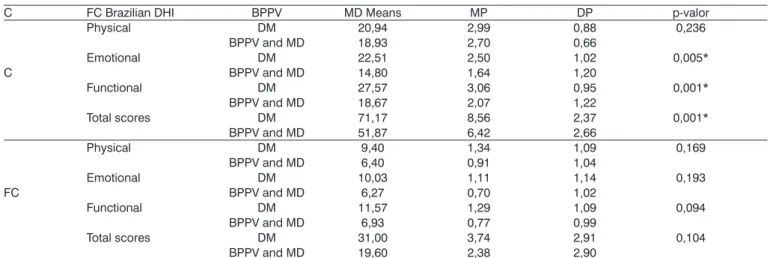
Based on the application of the identification and quality of life questionnaires during the interviews, the study showed that the quality of life of both patients with head and
Na hepatite B, as enzimas hepáticas têm valores menores tanto para quem toma quanto para os que não tomam café comparados ao vírus C, porém os dados foram estatisticamente
In the present study, institutionalized elderly persons with dizziness complaints had a low self-perception of quality of life, and the duration of dizziness, age, falls. and fear
This cross-sectional study assessed patients with TMD with or without coexisting tinnitus and aimed at on the quality of life as well on the intensity and duration of pain of
In light of the above, this study aimed at evaluating quality of life and adherence to treatment of ibromyalgia patients and at observing limitation or fear of movement as well as
The present study aimed at: 1) assessing the association be- tween distances walked in the 6MWT and the quality of life of premenopausal patients with low activity SLE; 2) comparing
