www.jped.com.br
REVIEW
ARTICLE
Excessive
crying
in
infants
夽
Ricardo
Halpern
∗,
Renato
Coelho
ChildDevelopmentOutpatientClinic,HospitaldaCrianc¸aSantoAntônio(HCSA),SantaCasadePortoAlegre,PortoAlegre,RS, Brazil
Received21December2015;accepted14January2016 Availableonline17March2016
KEYWORDS Excessivecrying; Infant;
Circadianrhythm; Infantilecolic
Abstract
Objective: Reviewtheliteratureonexcessivecryinginyounginfants,alsoknownasinfantile colic,anditseffectsonfamilydynamics,itspathophysiology,andnewtreatmentinterventions.
Datasource: TheliteraturereviewwascarriedoutintheMedline,PsycINFO,LILACS,SciELO, andCochraneLibrarydatabases,usingtheterms‘‘excessivecrying,’’and‘‘infantilecolic,’’as welltechnicalbooksandtechnicalreportsonchilddevelopment,selectingthemostrelevant articlesonthesubject,withemphasisonrecentliteraturepublishedinthelastfiveyears.
Summaryofthefindings: Excessivecryingisacommonsymptominthefirst3monthsoflife andleadstoapproximately20%ofpediatricconsultations.Differentprevalenceratesof exces-sive crying havebeen reported, ranging from14% to approximately30% ininfants up to3 months ofage. Thereis evidencelinking excessivecrying earlyinlife withadaptive prob-lemsinthepreschoolperiod,aswellaswithearlyweaning,maternalanxietyanddepression, attentiondeficithyperactivitydisorder,andotherbehavioralproblems.Several pathophysio-logicalmechanismscanexplainthesesymptoms,suchascircadianrhythmalterations,central nervous system immaturity, andalterationsin theintestinal microbiota. Severaltreatment alternatives havebeen described,includingbehavioral measures,manipulation techniques, useofmedication,andacupuncture,withcontroversialresultsandeffectiveness.
Conclusion: Excessivecrying intheearlymonths isaprevalentsymptom; thepediatrician’s attentionisnecessarytounderstandandadequatelymanagetheproblemandoffersupport toexhaustedparents.Theprescriptionofdrugsofquestionableactionandwithpotentialside effectsisnotarecommendedtreatment,exceptinextremesituations.Theeffectivenessof dietarytreatmentsanduseofprobioticsstillrequireconfirmation.Thereisincompleteevidence regardingalternativetreatmentssuchasmanipulationtechniques,acupuncture,anduseofthe herbalsupplementsandbehavioralinterventions.
© 2016 Sociedade Brasileira de Pediatria. Published by Elsevier Editora Ltda. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/ by-nc-nd/4.0/).
夽
Pleasecitethisarticleas:HalpernR,CoelhoR.Excessivecryingininfants.JPediatr(RioJ).2016;92(3Suppl1):S40---5. ∗Correspondingauthor.
E-mail:[email protected](R.Halpern). http://dx.doi.org/10.1016/j.jped.2016.01.004
PALAVRAS-CHAVE Choroexcessivo; Lactente; Ritmocircadiano; Cólicasdolactente
Choroexcessivodolactente
Resumo
Objetivo: Revisaraliteraturasobrechoroexcessivoembebêspequenos,cólicasinfantis,esuas repercussõesnafamíliaeafisiopatologiaeestratégiasdetratamentos.
Fontedosdados: Revisadasasprincipaisbasesdedados,Medline,PsycINFO,LILACSeSciELO eCochraneLibraryutilizando‘‘choroexcessivodolactente’’e‘‘cólicasdolactente’’.Foram selecionadasaspublicac¸õesmaisrelevantescomênfasenosúltimoscincoanos.
Síntesedosdados: Éumsintomacomumnosprimeirosmesesdevidaeémotivodecercade 20%dasconsultaspediátricas.Asprevalênciasdechoroexcessivovariamde14a30%nestes lactentes.Existemevidênciasligandoochoroexcessivonosprimeirosmesesdevidacom prob-lemasfuturosbemcomoaodesmameprecoce,ansiedade,depressãomaterna,TDAHeoutros problemascomportamentais.Distintosmecanismosfisiopatológicospodemexplicaressequadro clínico,comoalterac¸õesnoritmocircadiano,imaturidadedoSNC,ealterac¸õesnamicrobiota intestinal.Sãodescritosdiversasalternativasdetratamentodesdemedidascomportamentais, técnicasmanipulativas,usodemedicac¸ãoeacupunturacomresultadoseeficáciacontroversos.
Conclusão: Paraochoroexcessivonosprimeirosmesesénecessárioaatenc¸ãodopediatrapara oentendimento,manejodoproblemaeoferecersuporteparapaisemexaustão.Aprescric¸ão dedrogasdeefeitosduvidososepotenciaisefeitoscolateraisnãoéterapêuticapreconizada anãoseremsituac¸õesextremas.Aeficáciadostratamentosdietéticoseousodeprobióticos ainda necessitade confirmac¸ão. Existem evidencias incompletasa respeito de tratamentos alternativoscomotécnicasmanipulativas,acupunturaeusodesuplementoabasedeervase intervenc¸õescomportamentais.
© 2016 Sociedade Brasileira de Pediatria. Publicado por Elsevier Editora Ltda. Este é um artigo Open Access sob a licença de CC BY-NC-ND (http://creativecommons.org/licenses/ by-nc-nd/4.0/).
Introduction
Crying is a common symptom in the first 3 months of life and is responsible for approximately20% of pediatric consultations.Althoughinmostcasesthissymptomis self-limitedandof benignetiology,itisa sourceofstress and often leads parents and caregivers to exhaustion.1 Crying
is part of the normal development of a baby and
con-stitutes a form of communication with their caregivers,
althoughnonspecific,andcanbecausedbydifferentstimuli,
such as hunger, manifestation of discomfort or pain, or
simplythebaby’sneedtoapproachthecaregiverfor
emo-tional comfort and safety. Different prevalence rates of
excessive crying have been reported in several studies,
ranging from 14% to approximately 30% in infants up to
3 months of age.1,2 A meta-analysis performed with 22
longitudinalstudiesshowedevidencethatassociates
exces-sive crying and other regulatory difficulties (sleeping and
eating) in the first months of life with adaptive
prob-lems at school age, mainly related to attention deficit
hyperactivity disorder (ADHD) symptoms and associated
behaviors.3,4
In a cohort study in the city of Pelotas, infants
that had excessive crying in the first three months had
approximately 30% more behavioral problems than those
that did not have excessive crying, even after
con-trolling for all confounding factors.5 Additionally, it is
associated withearly weaning,and maternal anxiety and
depression.6---9
Definitions
and
classification
Inaclassicstudyaboutcryingininfants,Brazeltondefines excessivecryingasany amount ofcrying thatworries the parents,10 but the consensusdefinitionby severalauthors
arethe criteria defined by Wessel,11 known asthe ‘‘rule
of three’’ (crying spellsat least threehoursa day, three
timesaweekforthreeconsecutiveweeksandlastingthree
months).Evenwithaconsensus,thereisnosingledefinition
ofwhatshouldbeconsideredexcessivecrying.12Anattempt
atclassificationwascarriedoutusingthreecriteria: from
newbornupto4monthsofage, infantswithcrying spells
andirritabilityforthreeormorehoursaday, threedaysa
weekandatleastforoneweek,andnofailuretothrive,i.e.,
withoutanyconsequencesforthechild’sdevelopment.13An
examplewouldbeahealthy infant,agedupto3months,
whofeedswellandhasaprolonged,strident cryingspell,
whichcanlastuptoafewhours,writhingandbendingthe
kneesandthighsovertheabdomeneliminatinggases;the
childseemshungry,butdoesnotcalmdownafterbeingfed.
It is a crying spell without apparent cause and maybe a
manifestationofothermedicalconditions,self-limitedand
benign.
Although it has a benign etiology, it causes parental
stress,oftenleadingparentstoexhaustionwithoutsolving
theproblem,which,asa result,canleadparents totake
dangerousmeasuresinanattempttocalmtheinfant.14 In
additiontotheindiscriminateuse ofpainkillers and
excessivecrying withoutquick resolutionin infants isone
ofthecausesofshakenbabysyndrome.15,16
InstudybyBrazelton10 oftypicalinfants,excessive
cry-ingismeasuredinhours/day.Inthisstudy,themeancrying
timeofaninfantaged2weeksisonehourand45minutes,
andat 12weeksofage,themeantimeisuptotwohours
and45minutes;at 12weeks,themeantimedecreases to
onehour.Thesecryingspellsaremorefrequentinthelate
afternoon,withapeakoccurrenceat3---6weeksofage.
Over time, attentive caregivers begin to differentiate
whatmotivatestheinfant’scrying,buttheperceptionof
dis-comfortandsufferingoftenconfoundstheirinterpretation,
leadingtoanovervaluationandhinderingamorethorough
assessment. As a didactic characterization and
classifica-tion,thecryingcouldbedividedintothreecategories:(1)
normal/physiological; (2) excessive,secondary to
discom-fortor disease;and(3)without anapparentcause,where
colicisincluded.17
Colic
Colicisaclinicalmanifestation,forwhichseveralattempts at explanation have been made and of whose etiology stillremains unclear.18 The current understanding is that
infantilecolicisavariationofnormalityratherthana
patho-logical entity,12,18 and it is a phenomenon that stilllacks
furtherunderstanding,butitisanimportantmanifestation,
throughcrying,thataffects20---30%ofinfantsupto3months
of age.12 Aprospective study with ten yearsof follow-up
showed that excessive crying caused by colic may be an
earlymanifestationofsusceptibilitytorecurrentabdominal
pain,psychologicalproblems,andallergiesthatwillaffect
childhood.19
Amongthestudiesontheetiologyand
pathophysiologi-calmechanisms,thecurrentandmostacceptedhypothesis
isthatexcessivecryingiscausedduetoanimbalanceinthe
centralnervoussystemof theseinfants,supported bythe
factthatchildrenbornwithcentralnervoussystem
impair-menthave moreintensecrying spells,18 aswellasinfants
whose mothers or fathers have depression or those born
prematureor small for gestational age,20,21 who show an
increasedrisk of excessive crying during the firstmonths
of life. This hypothesis is based on the fact that these
groups,whonaturallyhavegreaterbiologicalrisk,arealso
at increased risk of developmental delays,which maybe
related to the immaturity of the central nervous system
(CNS)aswellasthedigestivesystem.
The circadian system plays an important role in the
CNS, and some studies associate this function with colic
andexcessivecrying.22 Thecircadiansystem,regulatedby
the hypothalamus, affects physiological activities such as
sleeptime,bodytemperature,feeding,andproductionof
hormonessuchasmelatonin;it maturesduring thefirst3
monthsoflife.Althoughnochangein totalhoursof sleep
hasbeendemonstrated,infantswithexcessivecryingshow
adifferentiatedpatterninrandomeyemovementsleepand
a fragmented sleep pattern.23 Additionally, cortisol does
notincreasesignificantlyonlyin casesofstress, asit also
shows a circadian rhythm, with an important role in the
process of waking in the morning;22 in a study with
con-trol group, including infants with and without colic, the
differencebetween them wastheabsence ofthe cortisol
circadianrhythminthegroupwithcolic.24
Theevidencethatsupportsthishypothesisisthatinfants
withexclusivebreastfeedinghavefewercolicspells;ithas
been observed that the nocturnal breast milk has higher
amountsof melatonin25 andthat theinfants tend tohave
longerandless-fragmentedsleep.Likewise,thereisa
vari-ationintheamountofmelatonininbreastmilk,whichmay
change according tothe mother’s mood26 and is possibly
relatedtostress.
Regarding nutritional intolerances, mainly the
intoler-ance to lactose or allergy to milk, and, indirectly, the
irritativesubstancestransmittedthroughbreastmilk,
sev-eralstudies suggest an insignificantparticipationof these
elementsinexcessivecryinginhealthyinfants,dividingthe
opinion of pediatric gastroenterologists.18 When an infant
haslactoseintoleranceorallergytocow’smilk,inaddition
tothecrying theinfantwillalsoshowotherclinical
mani-festations,andthusthecriteriaforcolicwillnolongerbe
valid, asthese infants are not healthy. Similarly, there is
no consensusin cases of gastroesophageal reflux and the
use of proton-pump inhibitors to reduce gastric juice, as
a procedure to relieve crying spells in infants with this
type of problem.27 In recent years, some studies focused
ontheassociationofintestinalmicrobiota,altered
intesti-nalmotility,andtheincreasedproductionofgases,causing
abdominalpainandresultingincrying.28---31Afterbirth,there
isagradualincreaseinthediversityoftheinfants’intestinal
flora, but in those withexcessive crying spells,
consider-ing the colic criteria, the diversity was lower and they
hadareducedamount ofbifidobacteriaandlactobacilli.28
Thecolonizationofgas-producingcoliformbacteriawas
sig-nificantly higher in children with colic spells in a study
of exclusively breastfed infants, with a predominance of
Escherichia coli.29 There is indication that there may be
an intestinal inflammatory reaction, in addition to lower
microbiotadiversityininfantswithcolicspells.31
Some newborns, while still in the nursery, can be
perceived as likely candidates to have excessive crying
spells,withincreased chancesof meeting thecriteriafor
colic.Theseinfantsaresensitive,withincreasedirritability,
prone to intense reactions and less adaptable, who take
longertocalmdownwiththeusualmeasuresofbeingheld
and cuddled.This situationcharacterizesthe influence of
the infant’s temperament, which is defined as a set of
characteristics relatedtothe typeof responsetostimuli,
their adaptive capacity(ability to calm down in stressful
situations),andactivitylevel.32,33Whenthisinfant,
charac-terizedby havingadifficult temper,finds anon-favorable
environment,withtenseandinsecurecaregivers whodeal
inadequately withtheinfant,the excessivecrying willbe
themostcommonmanifestationofdiscomfort.34,35 Studies
have been performed toverifywhether thedifficult
tem-per seenin adults,demonstratedbystructuralchanges in
their brains, may be predictive when observed in infants
withhyper-reactivetemperament.36
Even in infants without this a difficult temper, the
environmental factors that cause family disruption, such
as psychosocial problems and domestic violence, may be
relatedtoexcessivecrying.Theinfantactsasasignalerof
whatishappeningwiththeircaregivers,mainlythemother,
betterobservedinthecasesofpostnataldepression.20,37Ina
prospectivestudy,itwasshownthatstressduringpregnancy
was strongly related to excessive crying spells in infants
duringthefirst6monthsoflife.38
Diagnosis
Asinanyclinicalresearch,theassessmentbeginswitha his-toryofsymptomsdescribedbythefamily,providingdetails suchasfrequency,intensity,timeofoccurrence,and dura-tionofcrying.The complaintofexcessivecryingdemands fromthepediatrician a carefulassessmentof theinfant’s behaviorandreactions,andtheinteractionofparentsand caregivers. Italsodemands searching, wheneverpossible, for a triggering event or situationin the infant’s routine, evenifnotdirectlyconnectedtoit,suchasafamilystress situation(psychosocialfactorssuchasunemployment, mar-italcrises,mourning).Thewayparentsarriveanddescribe thecomplaint,associatedwiththedescriptionofhowthey holdandreceivetheirbabies,aswellasthestrategiesused tocalmthem,arean importantsourceofobservationand canbeusedtherapeuticallyduringtheconsultation.39 The
history and the motivation of the pregnancy and parents
facilitate the understanding,representation, andthe role
oftheinfantinthefamily.
During thephysical examination ofa small infantwith
excessivecryingthatmeetsthecriteriafor colic,itis not
common to find semiological alterations, but it is
indis-pensabletoperformacompleteexaminationaspartofthe
assessmentandasamanagementstrategy,inordertoensure
to parents that the infant does not have any associated
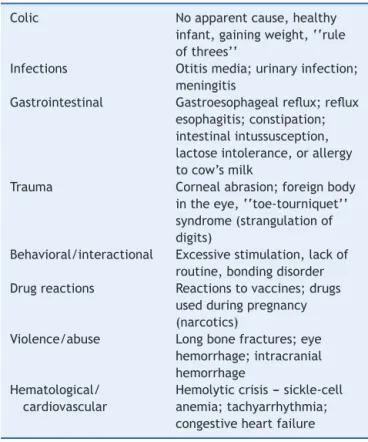
pathology. This procedure ensures the possibility of using
clinical reasoning tosearch, wheneverevident, for a
dif-ferentialdiagnosisamongthoselistedinTable1.Additional
testsarenotpartoftheresearchprotocolunlessthehistory
andphysicalexaminationsuggestssomepossiblecause.40
Clinicalmanagement
For clinical management, it is crucial to understand the complexity of symptoms and the possible causes, which in mostcases arenotexplicit. As inother behavioral and developmentmanifestations,theconceptofcumulativerisk effectcanbeappliedtoexcessiveinfantcrying.41 Mostof
the time, there is a set of factors with little individual
weight, but which together cause the clinical
manifesta-tion.Atfirst,itisnecessarytorecognizetheproblem,giving
supportandreassurance to thefamily, providing
informa-tionabout thebenign condition anditsnatural history,in
which95%ofcasesareself-limitedandonly5%haveprimary
causes.Informationaboutthenormalpatternofcryingand
theinfant’sself-regulatorymechanismshelptounderstand
the problem, as well as the necessary preventive
meas-ures against shaken baby syndrome and maltreatment.18
Often parents already show signs of fatigue and a few
areexhausted.Inextreme situations,theuseofnocturnal
emergencies services is frequent and, often, unnecessary
therapeuticmeasuresaretaken.
The necessary support to the family begins at the
consultationandwiththepediatrician’savailabilitytohelp
them.Thepediatricianmustbeattentiveandinterestedin
Table1 The mostcommon causesofexcessivecrying in younginfants.
Colic Noapparentcause,healthy infant,gainingweight,‘‘rule ofthrees’’
Infections Otitismedia;urinaryinfection; meningitis
Gastrointestinal Gastroesophagealreflux;reflux esophagitis;constipation; intestinalintussusception, lactoseintolerance,orallergy tocow’smilk
Trauma Cornealabrasion;foreignbody intheeye,‘‘toe-tourniquet’’ syndrome(strangulationof digits)
Behavioral/interactional Excessivestimulation,lackof routine,bondingdisorder Drugreactions Reactionstovaccines;drugs
usedduringpregnancy (narcotics)
Violence/abuse Longbonefractures;eye hemorrhage;intracranial hemorrhage
Hematological/ cardiovascular
Hemolyticcrisis--- sickle-cell anemia;tachyarrhythmia; congestiveheartfailure
Source:ModifiedandadaptedfromGrover.17
helping, and perform an adequate clinical assessment in
order to establish a secure baseline to confirm that the
infantishealthy.Thepositivereinforcementstrategyismost
effective when parents arehelped by the pediatrician to
findthesolutionstogether,ratherthanonlythetransferof
informationtothem.18
AccordingtotheWesselcriteriaforthediagnosis,theuse
oftheruleofthreesinthemanagementisalsouseful:(1)
infantilecolicisnotadisease;(2)nothingwillhappentothe
infantbecauseof thepain(dispelmyths);(3)colic passes
onitsownand‘‘itisaproblemthatthebabywilllearnto
solve’’(presentingthenaturalhistoryofthiskindof
prob-lem),relieving parentsfromtheresponsibility to‘‘solve’’
thecrying.42 Itisaneducationalprocessfortheparentsto
learntosolvecrises,clarifyingthemeaningsoftheinfant’s
crying,dispellingmyths,relievingfeelingsofguiltandthe
needtosharetheburden,whiletheotherrests.
It is essential to avoid the simplification of the
phe-nomenonandtheconsequentprescription ofcontroversial
drugs that have adverse effects, as well as exposing the
infanttounnecessarytestsandprocedures.Itisalso
impor-tanttodiscouragechangesintheinfant’sfeedingschemes,
suchasfrombreastmilktoinfantformula,aswellasfrom
theusual formula to differentbrands or sources,such as
soymilkorhydrolyzedformulas,withoutajustifiedclinical
basis.18Calmingthechildinoneoftheparent’sarms,orin
theproneposition,withawarmclothorusinghotwater
bot-tlestouchingthechild’sabdomenandabdominalmassage,
areproceduresthatshowsomeevidenceofcrying
improve-ment.Symptomimprovementwiththesetechniquesmaybe
mother---infantbonding,sleeppatterns,andstresshormone
levels;43 nevertheless,placingtheinfantintheprone
posi-tioninthecribshouldbediscouraged,evenifthisposition
improves thecrying spells.18 The useof a pacifier canbe
occasionally allowed if it calms the infant; the relevant
guidelinesforusingthisresourcecanbeleftforlater.42
Some approaches have shown some evidence of
bene-fit,suchaswrappingthe infant,which hasbeenshown to
bemoreefficientthe youngerthe babyis, upto8weeks
ofage,whencomparedtothegroupthatwasnotwrapped.
Historicalreportsshowtheuseofthisprocedureinthepast;
themaineffectisincreasedsleepdurationanddecreased
motoractivity.44Similarly,theuseofsleephygieneandthe
establishmentofaroutine,organizingtheinfant’sandthe
parents’day, provedtobeeffective inreducingcrying by
42%.45Theuseofteas,suchasfennel,licorice,chamomile,
and peppermint, were part of a systematic review, and
some encouragingresults were shown using fennel versus
placebo46;sincetheydonothave sideeffects,theycould
beusedasatherapeuticaid.18
The prescriptionof drugsis controversial andtheiruse
shouldbediscouragedduetothelackofevidenceof
ben-efits,butinrarecases,suchasinafamilycrisis,withvery
highanxietylevels,sleepdeprivation,withoutafamily
sup-portnetwork, and withtheinfant at risk ofsuffering the
consequencesof familydysfunction, drugs canbe
tempo-rarilyused.Themostoftenrecommendedarephenobarbital
at a dose of 10mg three times/day or diphenhydramine,
6mg,twotothreetimes/day,bothfor oneweek, sothat
the initial approach steps can be resumed.12 The use of
simethiconeisnowwell-acceptedinclinicalpractice,more
frequently through self-medication, but it shows no
evi-denceofbenefit,47 and itseffectcouldbea consequence
ofthecalmingeffectofitssweettaste.46
It is noteworthy that the isolated use of drugs greatly
reducestheeffectof amorecomprehensiveandsystemic
approachtosolvingtheproblem.12
The use of probiotics is part of several studies and is
increasing as a promise of improvement in colic
symp-toms,buttheevidenceofitseffectivenessandtheresults
arecontroversial.48 Inarecentmeta-analysistherewasan
improvement in crying and treatment effectiveness, but
onlyaftertwotothreeweeks andtogetherwiththe
nat-uralhistory ofcolicimprovement.49 Inanothersystematic
reviewandmeta-analysisstudy,theimprovementoccurred
onlyinthegroupofinfantsthatwasbreastfedandthestudy
concludedthat thereis littleevidencetorecommendthe
useofprobioticsinthetreatmentofinfantswithcolic.30
Somealternative therapieshavebeen proposedforthe
treatment of colic and excessive crying, including
chiro-practic and cranial manipulation. A systematic review in
theCochrane database,although showing insome studies
areductionincolicsymptomsandcryingusingthese
tech-niques,doesnotallowtheclinicaluseoftheoutcomesdue
topotentialbiasesinthestudies.50
Another proposed treatment is acupuncture, but its
resultsarealsocontroversial,andfurtherclinicaltrialsare
recommendedtoelucidatetheeffectsofthisformof
ther-apyforexcessivecryingandinfantilecolic.51
Crying as a prevalent symptom is usually a form of
communicationinyoungandhealthyinfants.The
pediatri-cian’scarefulassessment inseparatingsymptomsthatcan
have another meaning besides crying is essential for the
emotionalhealth oftheinfant.Itisincreasinglymore
evi-dentthatthefirstyears,whetherhealthyornot,willdefine
thechild’sdevelopmentandoftentheirbehaviorin
adult-hood.Therefore,buildingatherapeuticcooperationthrough
empathywillallowthepediatriciantobeanactiveobserver
and effectively elucidate the issues related to excessive
infantcrying.41,52
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.KimJS.Excessivecrying:behavioralandemotionalregulation disorderininfancy.KoreanJPediatr.2011;54:229---33. 2.ReijneveldSA,BrugmanE,HirasingRA.Excessiveinfantcrying:
theimpactofvaryingdefinitions.Pediatrics.2001;108:893---7. 3.HemmiMH,WolkeD,SchneiderS.Associationsbetween
prob-lems with crying, sleeping and/or feeding in infancy and long-termbehaviouraloutcomesinchildhood:ameta-analysis. ArchDisChild.2011;96:622---9.
4.Schmid G, Wolke D. Preschool regulatory problems and attention-deficit/hyperactivityandcognitivedeficitsatschool ageinchildrenbornatrisk:differentphenotypesof dysregula-tion?EarlyHumDev.2014;90:399---405.
5.SantosIS,MatijasevichA,CapilheiraMF,AnselmiL,BarrosFC. Excessivecryingat3monthsofageandbehaviouralproblemsat 4yearsage:aprospectivecohortstudy.JEpidemiolCommunity Health.2015;69:654---9.
6.Barros FC, Halpern R, Victora CG, Teixeira AMB, Béria JU. Promoc¸ão da amamentac¸ão em localidade urbana da região suldoBrasil:estudodeintervenc¸ãorandomizado.RevSaude Publica.1994;28:277---83.
7.HiscockH,CookF,BayerJ,LeHN,MensahF,CannW,et al. Preventingearlyinfantsleepandcryingproblemsandpostnatal depression:arandomizedtrial.Pediatrics.2014;133:e346---54. 8.VikT,GroteV,EscribanoJ,SochaJ,VerduciE,FritschM,etal.
Infantilecolic,prolongedcryingandmaternalpostnatal depres-sion.ActaPaediatr.2009;98:1344---8.
9.RadeskyJS,ZuckermanB,SilversteinM,RivaraFP,BarrM,Taylor JA,etal.Inconsolableinfantcryingandmaternalpostpartum depressivesymptoms.Pediatrics.2013;131:e1857---64. 10.BrazeltonTB.Cryingininfancy.Pediatrics.1962;29:579---88. 11.WesselMA,CobbJC,JacksonEB,HarrisGS,DetwilerAC.
Parox-ysmal fussing in infancy, sometimes called colic. Pediatrics. 1954;14:421---35.
12.CareyWB.ColicProlongedorexcessivecryinginyounginfants. In:CareyWB,editor.Developmental-behavioralpediatrics.4th ed.Philadelphia:SaundersElsevier;2009.p.557---62.
13.Hyman PE, Milla PJ,BenningaMA, Davidson GP,Fleisher DF, Taminiau J. Childhood functional gastrointestinal disorders: neonate/toddler.Gastroenterology.2006;130:1519---26. 14.Reijneveld SA, van der Wal MF, Brugman E, Sing RAH,
Verloove-Vanhorick SP. Infant crying and abuse. Lancet. 2004;364:1340---2.
15.DuhaimeAC,ChristianCW,RorkeLB,ZimmermanRA. Nonac-cidentalheadinjuryininfants---theshaken-babysyndrome.N EnglJMed.1998;338:1822---9.
18.AkhnikhS,EngelbertsAC,vanSleuwenBE,L’HoirMP,Benninga MA.Theexcessivelycryinginfant:etiologyandtreatment. Pedi-atrAnn.2014;43:e69---75.
19.SavinoF,CastagnoE,BrettoR,BrondelloC,PalumeriE,Oggero R.Aprospective10-yearstudyonchildrenwhohadsevere infan-tilecolic.ActaPaediatrSuppl.2005;94:129---32.
20.vandenBergMP,vanderEndeJ,CrijnenAA,JaddoeVW,Moll HA,MackenbachJP,etal.Paternaldepressivesymptoms dur-ingpregnancyarerelatedtoexcessiveinfantcrying.Pediatrics. 2009;124:e96---103.
21.MilidouI,Søndergaard C,JensenMS,Olsen J,HenriksenTB. Gestationalage,smallforgestationalage,andinfantilecolic. PaediatrPerinatEpidemiol.2014;28:138---45.
22.ShamirR,James-Roberts IS, DiLorenzo C,Burns AJ,Thapar N, Indrio F, et al. Infant crying, colic, and gastrointestinal discomfort in early childhood. J Pediatr Gastroenterol Nutr. 2013;57:S1---45.
23.BrandS,FurlanoR, SidlerM,Schulz J,Holsboer-TrachslerE. ‘‘Oh,baby,pleasedon’tcry!’’:ininfantssufferingfrom infan-tilecolichypothalamic---pituitary---adrenocorticalaxisactivityis relatedtopoorsleepandincreasedcryingintensity. Neuropsy-chobiology.2011;64:15---23.
24.WhiteBP,GunnarMR,LarsonMC,DonzellaB,BarrRG. Behav-ioralandphysiologicalresponsivity,sleep,andpatternsofdaily cortisolproductionininfantswithandwithoutcolic.ChildDev. 2000;71:862---77.
25.Cohen Engler A, Hadash A, Shehadeh N, Pillar G. Breast-feeding may improve nocturnal sleep and reduce infantile colic:potentialrole ofbreastmilkmelatonin. EurJPediatr. 2012;171:729---32.
26.KimataH. Laughter elevatesthe levelsofbreast-milk mela-tonin.JPsychosomRes.2007;62:699---702.
27.vanderPolRJ,SmitsMJ,vanWijkMP,OmariTI,TabbersMM, BenningaMA. Efficacy of proton-pumpinhibitors in children withgastroesophagealrefluxdisease:asystematicreview. Pedi-atrics.2011;127:925---35.
28.deWeerthC,FuentesS,PuylaertP,deVosWM.Intestinal micro-biotaofinfantswithcolic:developmentandspecificsignatures. Pediatrics.2013;131:e550---8.
29.SavinoF,CordiscoL,TarascoV,CalabreseR,PalumeriE, Mat-teuzziD. Molecular identification of coliform bacteria from colickybreastfedinfants.ActaPaediatr.2009;98:1582---8. 30.SungV,CollettS,deGooyerT,HiscockH,TangM,WakeM.
Pro-bioticstopreventortreatexcessiveinfantcrying.JAMAPediatr. 2013;167:1150---7.
31.RhoadsJM,FathereeNY,NororiJ, LiuY,LuckeJF, TysonJE, etal.Alteredfecalmicrofloraandincreasedfecalcalprotectin ininfantswithcolic.JPediatr.2009;155:823---8.e1.
32.BussAH, PlominR.Temperament:earlydeveloping personal-itytraits.1sted.Hillsdale(NJ):LawrenceErlbaumAssociates; 1984.
33.GoldsmithHH,AlanskyJA.Maternalandinfanttemperamental predictorsofattachment:ameta-analyticreview.JConsultClin Psychol.1987;55:805---16.
34.DouglasP,HillP.Managinginfantswhocryexcessivelyinthe firstfewmonthsoflife.BMJ.2011;343:d7772.
35.Yalc¸ınSS,ÖrünE,MutluB,Madenda˘gY,Sinici ˙I,DursunA,etal. Whyaretheyhavinginfantcolic?Anestedcase---controlstudy. PaediatrPerinatEpidemiol.2010;24:584---96.
36.Schwartz CE, Kunwar PS, Greve DN, Moran LR, Viner JC, CovinoJM,et al. Structural differences inadult orbitaland
ventromedialprefrontal cortex predictedbyinfant tempera-mentat4monthsofage.ArchGenPsychiatry.2010;67:78---84. 37.TalgeNM,NealC,GloverV.Earlystress,translationalresearch and preventionscience network: fetal and neonatal experi-enceonchildandadolescentmentalhealth.Antenatalmaternal stressandlong-termeffectsonchildneurodevelopment:how andwhy?JChildPsycholPsychiatry.2007;48:245---61.
38.Wurmser H, Rieger M, Domogalla C, Kahnt A, Buchwald J, KowatschM,etal.Associationbetweenlifestressduring preg-nancyandinfantcryinginthefirstsixmonthspostpartum:a prospectivelongitudinalstudy.EarlyHumDev.2006;82:341---9. 39.CéliaSAH,HalpernR.Aconsultaterapêutica:aimportânciada intervenc¸ãoprecocenaprimeirainfância.In:HalpernR, edi-tor.Manualdepediatriadodesenvolvimentoecomportamento. Barueri(SP):Manole;2015.p.73---82.
40.FreedmanSB,Al-HarthyN,Thull-FreedmanJ.Thecryinginfant: diagnostictestingandfrequencyofseriousunderlyingdisease. Pediatrics.2009;123:841---8.
41.HalpernR.Acrianc¸avulnerável:opapeldosfatoresderiscoe protec¸ãonadeterminac¸ãododesenvolvimentodacrianc¸a.In: HalpernR,editor.Manualdepediatriadodesenvolvimento e comportamento.Barueri(SP):Manole;2015.p.59---71. 42.CoelhoR.Choroexcessivodeumlactentepequeno-cólicas.
In:HalpernR,editor.ManualdePediatriadoDesenvolvimento eComportamento.Barueri(SP):Manole;2015.p.245---53. 43.Underdown A, Barlow J, Chung V, Stewart Brown S.
Mas-sageinterventionforpromotingmentalandphysicalhealthin infantsaged under six months. CochraneDatabase Syst Rev. 2006;18:CD005038.
44.VanSleuwenBE,L’hoirMP,EngelbertsAC,BusschersWB, West-ersP,BlomMA,etal.Comparisonofbehaviormodificationwith andwithoutswaddlingasinterventionsforexcessivecrying.J Pediatr.2006;149:512---22.
45.BlomMA,vanSleuwen BE,de VriesH,Engelberts AC,L’Hoir MP.Health careinterventionsfor excessivecrying ininfants: regularity withand without swaddling. JChild Health Care. 2009;13:161---76.
46.PerryR,HuntK,ErnstE.Nutritionalsupplementsandother com-plementarymedicinesforinfantilecolic:asystematicreview. Pediatrics.2011;127:720---33.
47.Danielsson B, Hwang CP. Treatment of infantile colic with surface active substance (simethicone). Acta Paediatr. 1985;74:446---50.
48.Cruchet S, Furnes R, Maruy A, Hebel E, Palacios J, Medina F,et al.The useofprobiotics inpediatric gastroenterology: a review of the literature and recommendations by latin-Americanexperts.PediatrDrugs.2015;17:199---216.
49.XuM,WangJ, WangN,SunF,Wang L,LiuX-H.Theefficacy andsafetyoftheprobioticbacteriumlactobacillusreuteriDSM 17938for infantilecolic:ameta-analysis ofrandomized con-trolledtrials. LionettiV,editor.PLOSONE. PublicLibraryof Science;2015;10(10):e0141445.
50.DobsonD,LucassenPL,MillerJJ,VliegerAM,PrescottP,Lewith G.Manipulativetherapiesforinfantilecolic.CochraneDatabase SystRev.2012;12:CD004796.
51.Savino F,Ceratto S,De MarcoA,Cordero diMontezemolo L. Lookingfor new treatments ofinfantile colic.ItalJPediatr. 2014;40:53.