Research article
Whole blood donor deferral analysis at General hospital blood bank – A retrospective study.Hinal Gajjar*, F R Shah**, N R Shah***, C K Shah****
*Assistant Professor, **Associate Professor,*** Professor & Head.**** Professor Dept. of Pathology, Smt. NHL Municipal Medical College, V S Gen Hospital, Ahmedabad.
Abstract Background:
A blood transfusion is a life saving procedure in many instances and it requires an adequate supply of safe blood. The most important is the selection of blood donors by donor selection criteria. A large number of blood donors are deferred from donating blood for several reasons either temporarily or permanently. A shortage of safe blood donor is frequent and it is important to understand the causes of deferral of potential donors.
Aims:
1. Primary objective of this study was to record and document the current rate and reasons for donor deferred in our blood bank.
2. Apply relevant findings to modify recruitment strategy for blood donors. Materials and methods:
Data for WBD presenting for blood donation in a blood bank V S General Hospital and outdoor camps over two and half years from January 2011 to June 2013 were analysed retrospectively. National Guidelines were used for selection & deferral of WBD.
Results:
3836 (11.16%) WBD were deferred out of 34373 registered donors during the study period. Donor deferrals were tabulated into temporary and permanent reasons. Temporary deferrals were 3113 (81.15%) and permanent deferrals were 723 (18.85%). The most common reasons were low haemoglobin (48.33%), high blood pressure (11.94%), underweight donors (7.95%) and history of medication use (6.13%) among total deferral donors. Majority of donors (47.16%) deferred were between 18 -30 years. Females were found to have higher deferral rate (25.48%) than males (10.76%). Discussion and conclusion:
A deferral study in blood donors may shed light on the health status of general population which may affect the present and future blood supply. It is important to provide donors with a clear message on their deferral status so that most of temporary deferral donors will return for donation in future.
Key words: Blood donor deferral, deferral reasons, blood bank.
Abbreviations: BP : Blood Pressure BT : Blood transfusion
BTS : Blood Transfusion Services CuSO4 : Copper sulphate
WBD : Whole Blood Donors
Introduction
Blood Transfusion Services (BTS) is the vital part of modern health care system without which efficient medical care is impossible. The aim of Blood Transfusion Services should be to provide effective blood and blood products, which are as safe as possible and adequate to meet patients’ need1. Many measures have been taken to make the blood transfusion safe by blood transfusion committee. The most important is the selection of blood donors by donor selection criteria2. A large number of blood donors are not able to donate blood successfully for several reasons, either temporarily or permanently. Individuals disqualified from donating blood are known as deferred donors. Blood donor deferral is a painful and sad experience for the blood donor as well as the blood centre screening the donor. Deferral leads to loss of precious whole blood donors (WBD) and blood units available for transfusion purposes. Additionally these donors are less likely to return for blood donation in future3. Knowledge of rate and causes of donor deferral can guide the recruitment strategy for WBD3,4. The few studies done in India in the past have provided different common reasons for deferral of whole blood donors highlighting differing demographic profile in different parts of the country5. The present study was undertaken to analyse the deferral incidence and pattern among blood donors in blood bank, Ahmedabad with an objective to review the centre’s policy for recruitment and retention of blood donors.
Material and methods
This retrospective record based study was carried out for whole blood donors at Blood bank over a period of two and half years from January 2011 to June 2013. Donors who have donated blood at our outdoor voluntary blood donation camps as well as at our blood bank (indoor) were included in the study. Standard operating Procedures based on the Directorate General of Health Services guidelines, Ministry of Health & Family Welfare (2003) used for donor selection and deferral. Pre-donation screening tests like donor questionnaire followed by physical examination & Hb estimation by CuSO4 (finger prick) method with cut off value of
as independent attempts for blood donation. Deferred donor data was analysed with respect to age, sex and causes of deferral (temporary and permanent). Five leading causes of deferrals in male and female blood donors were also analysed. Suitable statistical tests were applied to find significant differences among different variables.
Results
A retrospective study was done over a period of two and halfyears from 1st January 2011 to 30th June 2013. Total 34373 potential donors were screened at our blood bank (as well as outdoor voluntary blood donation camps). Of the total 34373 donors, 30537 were selected for blood donation (88.84%) and 3836 (11.16%) found unfit to donate for various reasons. Amongst 30537 donors, voluntary donors were 26323 (86.21%) and relative donors were 4214 (13.79%) (Table I). As shown in Table II, out of 33431 registered male donors, 29835 (89.24%) were selected & 3596 (10.76%) were deferred for blood donation. While out of 942 registered female donors 702 (74.52%) were selected & 240 (25.48%) were deferred.
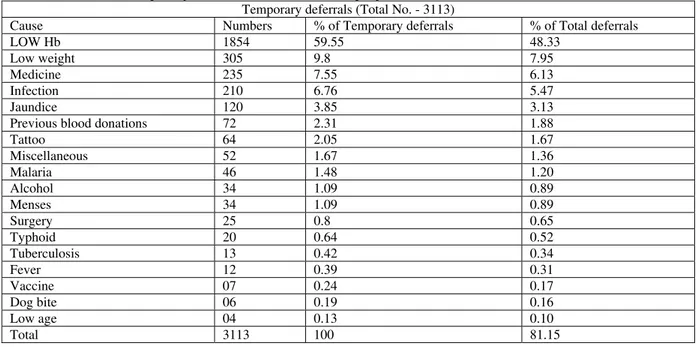
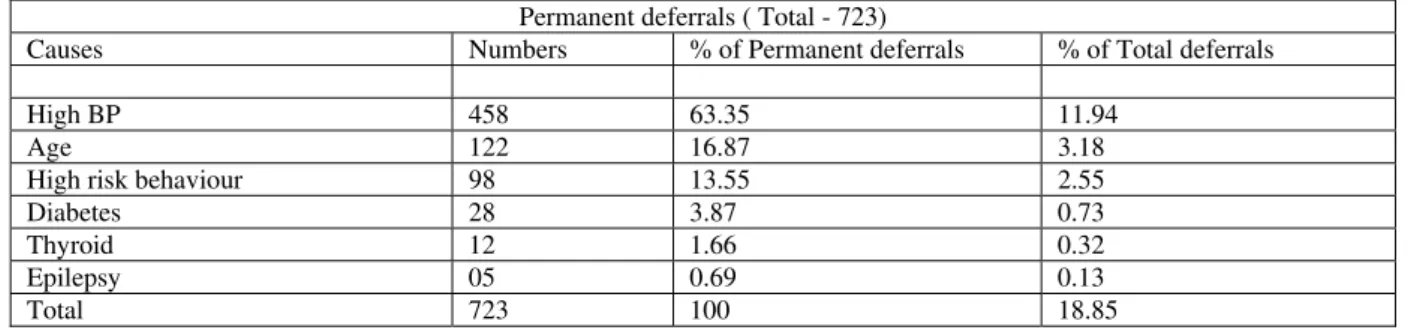
Deferral rate was significantly higher among females (Z=5.17; p<0.05). The majority i.e. 3113 (81.15%) donors were deferred for temporary reasons and smaller subset i.e. 723 (18.85%) donors were permanently deferred. The causes of deferrals in the temporary and permanent subsets are shown in Table III & IV. Anaemia (Hb<12.5) was the leading cause of donor rejection (59.55%) followed by underweight (9.8%) amongst temporary causes. In permanently deferred category, Hypertension was the most common cause constituting 63.35% of all the permanently rejected potential donors. As shown in Table V, amongst the five leading causes of deferrals in males, anaemia (47.97%) and uncontrolled Hypertension (12.51%) were most common while in female anaemia (53.75%) and menstruation (14.17%) were major causes. As prevalence of anaemia was evidently high in both males and females, the difference was not statistically significant (Z= 1.75; p>0.05).
As shown in Table VI, highest number of deferral (47.16%) both in male & female, were between the age group of 18-30 years.
Table I: Demographic profile of all blood donors:
Category of donor No. of blood donation % of total donation
Voluntary 26323 86.21%
Replacement 4214 13.79%
Total 30537 100%
Table II: Gender distribution of registered, selected and deferred donors:
Donors Male Female Total
Registered 33431 942 34373
Selected 29835 (89.24%) 702 (74.52%) 30537 (88.84%) Deferred 3596 (10.76%) 240 (25.48%) 3836 (11.16%)
Table III: Causes of temporary deferrals with their relative proportions.
Temporary deferrals (Total No. - 3113)
Cause Numbers % of Temporary deferrals % of Total deferrals
LOW Hb 1854 59.55 48.33
Low weight 305 9.8 7.95
Medicine 235 7.55 6.13
Infection 210 6.76 5.47
Jaundice 120 3.85 3.13
Previous blood donations 72 2.31 1.88
Tattoo 64 2.05 1.67
Miscellaneous 52 1.67 1.36
Malaria 46 1.48 1.20
Alcohol 34 1.09 0.89
Menses 34 1.09 0.89
Surgery 25 0.8 0.65
Typhoid 20 0.64 0.52
Tuberculosis 13 0.42 0.34
Fever 12 0.39 0.31
Vaccine 07 0.24 0.17
Dog bite 06 0.19 0.16
Low age 04 0.13 0.10
Total 3113 100 81.15
Table IV: Causes of permanent deferrals with their relative proportions
Permanent deferrals ( Total - 723)
Causes Numbers % of Permanent deferrals % of Total deferrals
High BP 458 63.35 11.94
Age 122 16.87 3.18
High risk behaviour 98 13.55 2.55
Diabetes 28 3.87 0.73
Thyroid 12 1.66 0.32
Epilepsy 05 0.69 0.13
Total 723 100 18.85
Table V: Five leading causes of deferrals in male and female blood donors
Male (3596) Female (240)
Causes Number % of deferrals Causes Number % of deferrals
Low Hb 1725 47.97 Low Hb 129 53.75
High BP 450 12.51 Menses 34 14.17
Low weight 278 7.73 Low weight 27 11.25
Medicine 226 6.28 Infection 12 5.00
Infection 198 5.50 Medicine 09 3.75
Table VI: Demographic profile of various age groups of deferred blood donors.
Male (3596) Female (240)
Age in years Number of donors % of deferrals Age in years Number of donors % of deferrals
<18 04 0.11 <18 - -
18-30 1710 47.55 18-30 99 41.26
31-40 912 25.36 31-40 63 26.25
41-50 549 15.26 41-50 47 19.58
51-60 299 8.10 51-60 18 7.50
>60 134 3.72 >60 13 5.41
Total 3596 100 Total 240 100
Discussion
Adequate supply of blood is most important and it is also essential that the blood collection process doesn’t harm either the donor or the recipient. Safe donor is the first step towards Safe Transfusion Services. This is achieved by donor selection criteria4.
While losses resulting from consequences of rigorous screening for transfusion transmitted infections have been the focus of our attention for more than a decade, reasons for donor deferrals has not received as much as attention6. In order to quantify the losses due to deferred donors and to understand the health problems of the donor population, a retrospective study was conducted. The rate and reasons of deferral differs from region to region and from one centre to another. Donor deferral rates in blood centres vary from 5%- 24%, leading to huge losses in terms of available units for transfusion in the nation every year 7.
In our study we segregated donor deferrals on the basis of medical history and physical examination. Our objective was to formulate definite strategy based on point of exit of prospective blood donors in order to increase the efficiency of the donor screening process.
In our study 3836 (11.16%) out of total 34373 registered perspective blood donors were found
unfit to donate for various reasons. Deferral incidence in our study was 11.16% which was similar to that observed by Zou et al 8 (12.8%), Chaudhary et al9 (16.4%), Bahadur and Colleagues6 (9%), Custer et al10 (13.6%), Lawsen Ayayi et al11 (10.8%) and Lim et al3 (14.4%). However studies by other authors have cited Low12,13 (5.6 -7.1%) to very high 7,14,15 (20 – 35.6%) deferral incidence in their populations, which probably reflects the regional diversity and marked variations in whole blood donor eligibility criteria internationally16,17. The most common cause of temporary deferral in our study was low Hemoglobin (59.55% of temporary deferral) similar to that reported by Custer et al10 (60% of temporary deferral) and Halperin et al18 (46%). The second most common cause of deferral was low weight accounted for 9.80% of temporary deferrals while Bahadur et al6 studied 26.6% deferral rate of low weight
Haemoglobin and low weight combined accounted for 56.28% of total deferral which is similar to the findings of Shalini–Bahadur 6(59.5%).
and motivation of donors to seek medical attention for anaemia, will improve the eligibility of prospective donors in the long run.
The most common reason for permanent deferral found in our study was high blood pressure which was also the most common cause in male similar to Sunder P study5 and Bahadur S study6. This signifies hypertension as the major under diagnosed epidemic in Indian population.
In our study 81.15% of donors were deferred for temporary reasons and 18.85% were deferred for permanent reasons. Other studies like Custer et al10 (10.6%) and Arslan19 (10%) reported rate of permanent deferral similar to our study. Temporary deferral, no matter how short in duration, represents an indefinite deferral for a sizable percentage (81.15%) with leading causes of anaemia and low weight. All these can be actively and aggressively managed by calling them back after correction of their cause which can help to retain future donor pool.
Conclusion
Findings of our study are summarised as follows: 1. Incidence of WBD deferral was 11.16%,
majority of them (81.15%) was being deferred for temporary reasons and a smaller subset (18.85%) for permanent reasons.
2. Most common reasons for deferral were low haemoglobin (48.33%), high blood pressure(11.95%), underweight(7.95%) and history of antibiotic/medication use(6.13%).
3. Anemia was the most common reason (59.55%) in temporary deferrals, while Hypertension (63.35%) is the most common reason in permanent deferral. 4. Most of these deferral donors (47.16%)
were of age 18 – 30 years old.
5. Females were found to have higher deferral rate (25.48%) than males (10.76%).
6. Analysis of rejection pattern (deferral rate) is of vital significance in formulating and modulating the policies towards modern blood transfusion services. Hence studying the profile of blood donors will help to identify the sections of the populations which could be targeted to increase the pool of voluntary donors and also to guide and provide the necessary data base for the policy design and program implementation. As deferral leads to loss of present & future precious blood units, it is high time to take effective measures & modify recruitment strategy on issue of lost donors.
References:
1. Organization of Blood
Transfusion Services in : Transfusion Medicine Technical Manual, Second Edition 2003; Edited by Dr. R.K. Saran, WHO DGHS guidelines, Ministry of Health and Family Welfare : 1-6. 2. Unnikrishnan B , Rao P Kumar
N, Ganti S, Prasad R et al. Profile of blood donors and reasons for deferral in coastal South India. Australasian Medical Journal. 2011; 4 (7) :379 – 385
3. Lim JC, Tien SL, Ong YW. Main causes of pre–donation deferral of prospective blood donors in the Singapore blood transfusion service. Ann Acad Med Singapore. 1993; 22: 326 – 31 [Pub Med].
4. Naveen Agnihotri. Whole blood donor deferral analysis at a centre in Western India. Asian J Transfus Sci. 2010; 4(2) : 116 – 122.
5. Sunder P, Sangeetha SK, Seema DM, Marimuthu P, Shivana N. Pre – donation deferral of blood donors in South Indian set–up: An analysis. Asian J Transfus Sci. 2010 July; 4 (2) : 112 – 115. 6. Bahadur S, Jain S,Goel RK,
Pahuja S, Jain M. Analysis of blood donor deferral characteristics in Delhi, India. South east Asian J Trop Med Public Health. 2009; 40 (5) : 1087 – 91.
7. Tomasul. PA, Anderson AI, Paluso MB, Gutschenritter MA, Aster RH. A study of criteria for blood donor deferral. Transfusion 2003; 20(5) : 511 -18.
8. Zou S, Musavi F, Notari EP, Rios JA, Trouern - Trend, J Fang CT. Donor deferral and resulting donor loss at the American Red Cross Blood Services, 2001 through 2006. Transfusion 2008; 48(12) : 2484 – 6.
9. Chaudhary RK, Gupta D, Gupta RK. Analysis of donor – deferral pattern in a voluntary blood donor population. Transfusion Med. 1995; 5 (3) : 209 -12.
the donated blood supply due to donor deferral and miscollection. Transfusion, 2004; 44(10) : 1417 – 26.
11. Lawson – Ayayi S, Salmi LR. Epidemiology of blood collection in France. Eur J Epidemiol 1999; 15 : 285 – 92.
12. Rabeya Y, Rapiaah M, Rosline H, Ahmed SA, Zaidah WA, Roshan TM. Blood pre–donation deferrals–a teaching hospital experience. Southeast Asian J. Trop Med Public Health. 2008; 39 (3): 571 – 4.
13. Kwa SB, Ong YW, Gaw YN. Blood donor rejects – a study of the causes and rejection rates. Singapore Medical Journal 1966; 7 (1) : 61 – 8.
14. Charles KS, Hughes P, Gadd R, Bodkyn CJ, Rodriquez M. Evaluation of blood donor deferral causes in the Trinidad and Tobago National blood Transfusion Service. Transfusion Med. 2010; 20(1) : 11 -14. 15. Madan N, Qadiri J, Akhtar F.
Study of Blood Donor Profile at a Tertiary Care Teaching Hospital. Journal of the Academy of Hospital Administration. 2005; 17 (2) : 31 – 4.
16. Di Lovenzo Oliveiva C, Loureiro F, de Bastos MR, Proietti FA, Carneiro – Proietti AB. Blood donor deferral in Minas Gerais State, Brazil : blood centres as sentinels of urban population health. Transfusion. 2009; 49(5) : 851 - 7.
17. Karp JK, King KE. International variation in volunteer whole blood donor eligibility criteria. Transfusion. 2010; 50(2) : 507 – 13.
18. Halperin D, Baetens J, Newman B. The effect of short term temporary deferral on future blood donation. Transfusion 1998; 38 : 181 – 3.