The
Brazilian
Journal
of
INFECTIOUS
DISEASES
w w w. e l s e v ie r . c o m / l o c a t e / b j i d
Original
article
Body
composition
and
lipodystrophy
in
prepubertal
HIV-infected
children
Cecilia
Zanin
Palchetti,
Rose
Vega
Patin,
Aída
de
Fátima
Thomé
Barbosa
Gouvêa,
Vera
Lúcia
Szejnfeld,
Regina
Célia
de
Menezes
Succi,
Fernanda
Luisa
Ceragioli
Oliveira
∗UniversidadeFederaldeSãoPaulo,EscolaPaulistadeMedicina,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received31August2011 Accepted28October2012 Availableonline11January2013
Keywords: HIV Child Lipodystrophy Bodycomposition Anthropometry
a
b
s
t
r
a
c
t
Objective:ToidentifylipodystrophyinprepubertalHIV-infectedchildrenusing anthropo-metricparametersandbodycompositionassessment.
Methods:Cross-sectionalstudyincluding40prepubertalHIV-infectedchildrenofboth gen-dersseenattheCareCenteroftheDivisionofPediatricInfectiousDiseases–Universidade Federal deSãoPaulo, SãoPaulocity, Brazil,wascarriedout fromAugusttoDecember 2008.Age,clinicalandimmunologicalstatus,prophylaxis,transmissionandhighlyactive antiretroviraltherapywererecorded.Bodymassindexz-scoreandheight-for-agez-score werecalculatedtocharacterizethenutritionalstatus.Circumferencesweremeasuredwith flexibletapeandskinfoldswereassessedbyanadipometry.Fatmassandleanmasswere determinedbydual-energyX-rayabsorptiometry.Presenceofclinicalsignsoflipodystrophy wasassessedbyatrainedclinician.DatawereanalyzedusingSPSS12.0software. Results:Themeanageandstandarddeviationwere9.8(1.2)years,50%weregirlsand82.5% childrenfromBandCcategories.Clinicallipodystrophyanddislypidemiawerepresentin 27.5%and70%,respectively.Thetrunktoarmratioandthelimbtotrunkratiohad posi-tiveassociationwithlipodystrophy.Patientswithlipodystrophyhadshortstature,higher triglyceridesvaluesandlowerHDL-cholesterol.
Conclusion: Theratiosobtainedbyskinfoldsanddual-energyX-rayabsorptiometry measure-mentscanbeconsideredasindicatorsofpreclinicallipodystrophy.Thecutoffpointshave notbeendeterminedyet;however,continuousassessmentmaybeusefultoidentifyearly bodycompositionchanges.
©2013ElsevierEditoraLtda.Allrightsreserved.
Introduction
The highly active antiretroviral therapy (HAART) has sig-nificantly reduced morbidity and mortality in HIV-infected children.AU.S.multicenterstudyshowedthat,between1994
∗ Correspondingauthorat:UNIFESP/EPM,DepartamentodePediatria,RuaLoefgreen,1647,04040-032,SãoPaulo,SP,Brazil.
E-mailaddress:[email protected](F.L.C.Oliveira).
and2000,thedeathratedecreasedfrom7.2to0.8per100 chil-dren/year,remainingstableuntil2006.1InBrazil,probabilityof
survivalto60monthshasincreasedfrom52.8%among chil-drendiagnosedduringtheperiodbetween1983and1998to 86.3%amongchildrenbornfrom1999to2007.2Assuredly,in
additiontopreserveorrestoretheimmunesystem,theuse
ofHAARTalsocontributestomaintainorimproveweightfor heightgrowth.3
Nonetheless,HIVinfectionitselfandtheuseof antiretro-viraltherapy cause clinical andmetabolic changesinitially describedinadultsinthelate90s4andsubsequentlyobserved
inchildrenandadolescents.5Duetoprecocityandlarge
expo-suretothedrug,especiallyininfectionsacquiredbyvertical transmission,thispopulationshowshigherrisksof develop-ingadverseeffectsofantiretroviraltherapy.5
Among other metabolic side effects of antiretroviral therapy, we mention the lipodystrophy syndrome, which compriseslipodystrophy,dyslipidemia,insulinresistanceand cardiovascularrisk.6Lipodystrophyisidentifiedand
charac-terizedbytheuseofclinicalparameters,whichcausesseveral difficulties.7,8 Anthropometric measurements and
assess-mentofbodycompositionareusefulinstrumentstomonitor theevolutionofgrowth,alsobeingusefultoidentifythe pres-enceofclinicalandmetabolicchanges.9Therefore,thisstudy
aims to identify lipodystrophy in prepubertal HIV-infected children through anthropometric measurements and body compositionassessments.
Methods
Wecarriedoutacrosssectionalstudywith52prepubertal chil-dren(7–12yearsold),bothgenders,seenattheCareCenter oftheDivisionofPediatricInfectious Diseases(CEADIPe)of theDepartmentofPediatricsofUNIFESP/EPMfromAugustto November2008.Childrenwithgeneticsyndromeor neurop-athywerenotincluded.Onehospitalizedpatientdied,fivehad neuropathyandsixwerenotallowedbythecaregiverto partic-ipateinthestudy.Thus,thefinalsampletotaled40patients. Thestudy wasapprovedbytheResearchEthicsCommittee oftheUniversidadeFederaldeSãoPauloandinitiatedupon consentinwritingofparentsorguardians.
Pubertalstagewasassessedbythepediatrician,whoused, asacriterion,thedevelopmentofthesecondarysexual char-acteristicsproposedbyMarshallandTanner,10includingthe
studychildrenandadolescentswhoshowedstaging.1Inorder
toclassifythedisease,weusedtheclinicalparametersand immunologicalcategoriesproposedbytheMinistryofHealth,3
whichadoptedtheguidelines fromthe CentersforDisease Controland Prevention(CDC),11 inaddition toinclusion of
pulmonarytuberculosisasacriterioninclinicalcategoryB. Data on identification, age, type of transmission, pro-phylaxis, patient’s legal caregiver and/or guardian and antiretroviralregimenwerecollectedfromthemedicalrecords ofthesepatients.Clinicallipodystrophywasclinically iden-tified by the pediatrician, showing threecharacterizations: lipoatrophy,lipohypertrophyandmixedlipodystrophy.12
Weightandheightmeasurementswereusedtocalculate thebodymassindexz-score(zBMI)andheight-for-agez-score (HAz), pursuantto the reference standard and recommen-dation ofthe World Health Organization.13 Skinfolds were
measured byusingan adipometerunderthe brand Lange® (Beta TechnologyInc.,Santa Cruz, CA,USA)with precision of1mm, and circumferences were measured with a flexi-ble,non-extendabletapegraduatedin0.1-cm.Trunktoarm ratiowascalculatedthroughthesumofthesubscapularand
suprailiac skinfold divided bythe value resulting from the sumofbicepsandtricepsskinfolds.12Bodycompositionwas
assessed through dual-energy X-ray absorptiometry (DXA) byonlyonetrainedtechnician(equipmentLUNARTMDPX-L,
pediatricsoftware,version1.5).Theratiolimbtotrunkwas obtainedbyaddingthefat(g)inarmsandlegsanddividingit bythefatvalue(g)intrunk.
HIVviralloadwasdeterminedthroughtheRT-PCR tech-nique (Cobas Amplicor HIV-1 MonitorTM Test, version 1.5)
and TCD4 andT CD8lymphocyteswere assessedthrough flow cytometry (BD FACSCaliburTM System). The lipid
pro-filewasdetermined throughreflectancespectrophotometry – colorimetry– 540nm(Vitros Systems Chemistry750 XRC –Ortho-ClinicalDiagnostics,Inc.–Johnson&Johnson Com-pany, New York, NY, USA), using the cutoffs proposed by Kwiterovich.14Bloodglucosewasmeasuredthroughthe
enzy-matic method using hexokinase and glucose-6-phosphate dehydrogenase enzyme (Advia Chemistry System 1650 – Bayer) and insulin through an immunoenzymatic method (Tosoh–TosohCorporation,Tokyo,Japan).Fastinginsulinand bloodglucosewereusedtocalculatethehomeostaticmodel assessment-insulin resistance(HOMA-IR), which character-izesinsulinresistancewhenHOMA-IR>3.15Skeletalmuscle
masswascalculatedpursuanttoHeymsfieldetal.16
For statistical analysis, we used the Statistical Package fortheSocialSciences(SPSS)programversion12.0.To com-pare qualitative variables, we used the Chi-square test or Fisher’sExacttest.Tocomparequantitativevariables,weused Student’st-distributiontest. Shapiro–Wilktest wasusedto assess the normality of continuous quantitative variables. Thoseshowingnoregulardistributionweretransformedinto logarithm (log10)forthe statisticaltests. Wecomputed the
Pearson’scorrelationcoefficientinordertoshowthedegree oflinearcorrelationbetweenthe variables.Alinear regres-sionmodelwaspreparedtoinvestigatethedeterminantsof lipodystrophy.Thetrunktoarmratiowasusedasa depend-ent variable. Acorrelation matrix was developed,provided that the entry inthe model followed the ascending order withvaluep<0.20.Thevariablesthatadjustedthemodeland remainedsignificantweremaintainedinthefinalmodel. Val-uesofp<0.05weredeemedsignificant.
Results
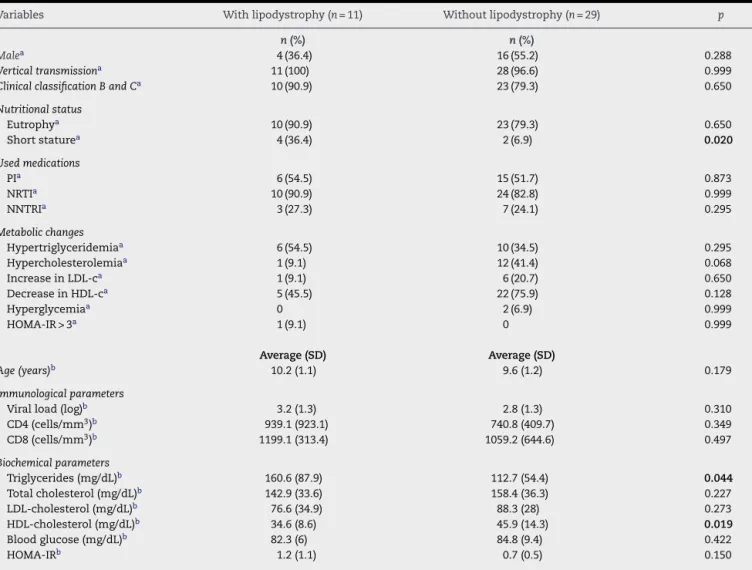
Table1–Characterization,nutritionalstatus,antiretroviraldrug,metabolicchangesandimmunologicalandbiochemical parametersofHIV-infectedprepubertalchildrenwithandwithoutlipodystrophy.
Variables Withlipodystrophy(n=11) Withoutlipodystrophy(n=29) p
n(%) n(%)
Malea 4(36.4) 16(55.2) 0.288
Verticaltransmissiona 11(100) 28(96.6) 0.999
ClinicalclassificationBandCa 10(90.9) 23(79.3) 0.650
Nutritionalstatus
Eutrophya 10(90.9) 23(79.3) 0.650
Shortstaturea 4(36.4) 2(6.9) 0.020
Usedmedications
PIa 6 (54.5) 15 (51.7) 0.873
NRTIa 10(90.9) 24(82.8) 0.999
NNTRIa 3(27.3) 7(24.1) 0.295
Metabolicchanges
Hypertriglyceridemiaa 6(54.5) 10(34.5) 0.295
Hypercholesterolemiaa 1 (9.1) 12 (41.4) 0.068
IncreaseinLDL-ca 1 (9.1) 6 (20.7) 0.650
DecreaseinHDL-ca 5(45.5) 22(75.9) 0.128
Hyperglycemiaa 0 2(6.9) 0.999
HOMA-IR>3a 1(9.1) 0 0.999
Average(SD) Average(SD)
Age(years)b 10.2(1.1) 9.6(1.2) 0.179
Immunologicalparameters
Viralload(log)b 3.2(1.3) 2.8(1.3) 0.310
CD4(cells/mm3)b 939.1(923.1) 740.8(409.7) 0.349
CD8(cells/mm3)b 1199.1(313.4) 1059.2(644.6) 0.497
Biochemicalparameters
Triglycerides(mg/dL)b 160.6(87.9) 112.7(54.4) 0.044
Totalcholesterol(mg/dL)b 142.9(33.6) 158.4(36.3) 0.227
LDL-cholesterol(mg/dL)b 76.6(34.9) 88.3(28) 0.273
HDL-cholesterol(mg/dL)b 34.6(8.6) 45.9(14.3) 0.019
Bloodglucose(mg/dL)b 82.3(6) 84.8(9.4) 0.422
HOMA-IRb 1.2(1.1) 0.7(0.5) 0.150
HOMA-IR,homeostaticmodelassessment-insulinresistance;NRTI,nucleosidereversetranscriptaseinhibitors;NNRTI,non-nucleosidereverse transcriptaseinhibitors;PI,proteaseinhibitors.Boldvaluesmeanthevaluesthatpresentedstatisticaldifference.
a Chi-squaretestorFisher’sExacttest.
b Student’st-test.
(PI).Timeofexposuretoantiretroviraltherapyinthis popula-tionwas7.8±2.4years.Asforthe nutritionalcondition,33 (82.5%)wereeutrophic,6(15%)overweight/obeseand34(85%) showedproperheight.Theprevalenceofdyslipidemiainthe studypopulationwas70%(28children).Regardingmetabolic changes,16 patients(40%)showedhypertriglyceridemia,13 (32.5%)hypercholesterolemia,13 (32.5%)adecrease inHDL cholesterolserumlevelsand7(17.5)anincreaseinLDL choles-terolserum levels.Insulin resistancewas foundin1(2.5%) patient.
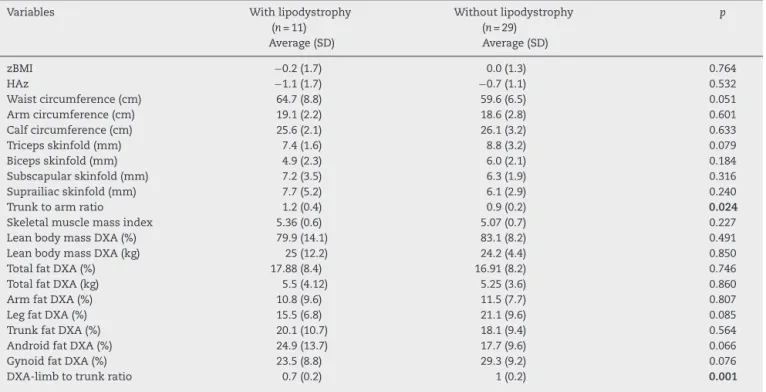
InTable1, wecomparedclinicalvariables and immuno-logicalandlaboratoryparametersofpatientsinthepresence orabsenceoflipodystrophy.Thetrunktoarmratio,obtained throughskinfolds,showedastrongassociationwiththe pres-ence of lipodystrophy, as well as the ratio limb to trunk determined throughDXA (Table2).When correlated,these variablesshowedamoderatenegativecorrelation(r=−0.69; p=0.000)(Fig.1).
Withrespecttowaistcircumferenceandothervariables, we noted a positive correlation with trunk to arm ratio
(r=0.42; p<0.007) and with zBMI (r=0.68; p=0.003) and a negative correlationwith the limbtotrunkratio (r=−0.68; p=0.000).Thetrunktoarmratioalsoshowedapositive corre-lationwithinsulin(r=0.48;p=0.001)and HOMA-IR(r=0.45; p=0.004), showing metabolic changes resulting from cen-tral adiposity.Asforbiochemicaltests, TCD4lymphocytes and viral load showed a positive and negative correlation withtotalcholesterol(r=0.41;p<0.008;r=−0.50;p=0.001)and LDLcholesterol(r=0.49;p=0.001;r=−0.65;p=0.000), respec-tively.ViralloadalsoshowedanegativecorrelationwithHAz
(r=−0.47;p=0.002).
The linear regression used the trunk to arm ratio as a controlvariableandshowedassociationwiththearm circum-ference (ˇ=0.71;p=0.045;IC95%:0.017–1.41)and HOMA-IR (ˇ=0.14;p=0.026;IC95%:0.018–0.271).
Discussion
Table2–Averageandstandarddeviationofanthropometricmeasures/indexesandfatpercentage(%)assessedthrough DXAofprepubertalHIV-infectedchildrenwithandwithoutlipodystrophy.
Variables Withlipodystrophy (n=11) Average(SD)
Withoutlipodystrophy (n=29)
Average(SD)
p
zBMI −0.2(1.7) 0.0(1.3) 0.764 HAz −1.1(1.7) −0.7(1.1) 0.532 Waistcircumference(cm) 64.7(8.8) 59.6(6.5) 0.051 Armcircumference(cm) 19.1 (2.2) 18.6 (2.8) 0.601 Calfcircumference(cm) 25.6 (2.1) 26.1 (3.2) 0.633 Tricepsskinfold(mm) 7.4 (1.6) 8.8 (3.2) 0.079 Bicepsskinfold(mm) 4.9(2.3) 6.0(2.1) 0.184 Subscapularskinfold(mm) 7.2(3.5) 6.3(1.9) 0.316 Suprailiacskinfold(mm) 7.7(5.2) 6.1(2.9) 0.240 Trunktoarmratio 1.2(0.4) 0.9(0.2) 0.024
Skeletalmusclemassindex 5.36(0.6) 5.07(0.7) 0.227 LeanbodymassDXA(%) 79.9(14.1) 83.1(8.2) 0.491 LeanbodymassDXA(kg) 25(12.2) 24.2(4.4) 0.850 TotalfatDXA(%) 17.88(8.4) 16.91(8.2) 0.746 TotalfatDXA(kg) 5.5(4.12) 5.25(3.6) 0.860 ArmfatDXA(%) 10.8(9.6) 11.5(7.7) 0.807 LegfatDXA(%) 15.5(6.8) 21.1(9.6) 0.085 TrunkfatDXA(%) 20.1(10.7) 18.1(9.4) 0.564 AndroidfatDXA(%) 24.9(13.7) 17.7(9.6) 0.066 GynoidfatDXA(%) 23.5 (8.8) 29.3 (9.2) 0.076 DXA-limbtotrunkratio 0.7 (0.2) 1 (0.2) 0.001
zBMI,bodymassindexz-score;HAz,height-for-agez-score;BIA,bioimpedance;DXA,dual-energyX-rayabsorptiometry.Boldvaluesmeanthe valuesthatpresentedstatisticaldifference.
USpopulation(29%).17 AnotherBrazilianassessmentfound
lipodystrophyin14%ofHIV-infectedchildren.18
Scientific evidences suggest that lipohypertrophy and lipodystrophyitselfaremorefrequentinpubescentchildren, as sexual maturity and hormonal factors may contribute tothis outcome.12,19 Thediagnosis of lipohypertrophyand
mixedlipodystrophyinprepubertalchildreninthisstudymay beexplained by the advanced classificationof the disease andhighprevalenceofdyslipidemia.Lipodystrophy,insulin resistanceanddyslipidemia,withsubsequentincreasein car-diovascular risk, characterize the lipodystrophy syndrome, inwhichetiology seemstoberelatedwithsomeclassesof antiretroviraldrugs,suchasPIandnucleosidereverse trans-criptaseinhibitors (NRTI); duration of drugadministration;
05
1
1
.5
2
-5 0 .5 1
DXA-Limbs-trunk ratio
Skinfold trunk to arm ratio (log)
95% CI Fitted values
DXA-limb to trunk ratio
r=-0.69 (p=0.000)
Fig.1–Pearson’scorrelationbetweentheratiolimbto
trunkobtainedthroughDXAandtrunktoarmratio
obtainedthroughskinfolds(r=−0.69;p=0.000).DXA,
dual-energyX-rayabsorptiometry.
increaseinviralload;lowlevelsofCD4andpriorincreasein serumlevelsoftriglyceridesandcholesterol.4,6
In this study population, there is a higher serum level oftriglycerides and lower HDL cholesterolinpatientswith bodyfatredistribution.TheEuropeancohortrelatedthe pres-enceoflipodystrophywithlevelsoftriglycerides,insulinand blood glucose.20 ASpanishstudy withheterogeneous
pedi-atricpopulation(21monthsto18yearsold)verifiedahigher prevalenceoflipodystrophywithinthehigheragegroupandin thepresenceofhypertriglyceridemia,withnopositive associ-ationwithviralload,TCD4lymphocyte,totalcholesteroland glucose.Withrespecttoclassesofantiretroviraldrugs,wedid notnoteassociationwithlipodystrophy.Thecurrentliterature evidencesconflictingdataastothepresenceoflipodystrophy associatedwiththeuseofPI.AUSstudywithapopulation averaging 11.9 years showed no association21 between the
drug use and this clinical change, while another Brazilian work,withapopulationaveraging9.1years,verifiedapositive associationbetweenthesetwovariables.22
The use of antiretroviral therapy plays a positive role as to maintenance or improvement of nutritional condi-tion, however, in children with lipodystrophy, we noted a higherprevalenceofshortstature.Hormonalfactors, nutri-tional condition, gastrointestinal and endocrine disorders, insufficientfoodintakeandrecurrentinfectionmayalso com-promiseheightdevelopment.23,24Themechanismbywhich
thisimpairmentoccursisnotverywelldescribedinthe litera-ture,anditispossibletofinddivergencesbetweenresearchers andreviewswithrespecttothistopic.23,25
to be a resistance to GH, with increase in its levels and decreaseinIGF-1.26Anotherhypothesiswouldbeachangein
IGF-1levels,resultingfromtheimpropersynthesisof insulin-like growthfactor binding protein-1(IGFBP-1)and increase in insulin-like growth factor binding protein-3 (IGFBP-3).25
Ininfected children,resistance toGH and changes in pro-ductionofcortisoldirectlyaffectthebodymassandgrowth interruption.27Interactionbetweenhormonaldisordersand
lipodystrophyseemstoberelatedtoanincreasein somato-statintone, whichwillinhibit secretionofGH, decrease in ghrelinanddecreaseofGHcausedbytheincreaseinfreefatty acids.28
GH and IGF-I act directly in muscle fibers, increasing protein synthesis and body mass. Nonetheless, in chronic diseasessuchasAIDS,thestressgeneratedbyapermanent inflammatorycondition contributesthrough hepatic gluco-neogenesistothedepletionofessentialaminoacids ofthe skeletalmuscle.23Thefastlossofmusclemassresultsfrom
accelerationinproteinbreakdownanddegradationof myofib-rillarproteinsthroughactivationoftheubiquitinproteasome system.29 Inthis alternativemetabolicpathway,thereisan
activation of transcription factors (FoxO3) in cell nucleus, causinganincreaseinlysosomalandproteasomalproteolysis, whichwillberesponsibleformitochondrialandmyofibrillar loss.29Inphysiologicalterms,whentheIGF1/insulin–
P13k-Aktsignalingpathwayisactivated,FoxO3isdeactivatedand cytosolisreleased.30
Lipodystrophy is classified on a clinical and subjective basis.3,7,8 Accordingly, the assessment of anthropometric
measurementsand bodycompositioncouldbeinstruments thathelpdetectingclinicalandmetabolicchanges.Although the average value of waist circumference did not show a significantstatisticaldifference(p=0.051),aresultthatmay belimitedduetothesamplesize,thisvariable washigher inthegroupwithlipodystrophy.Additionally,valuesof cor-relationcoefficientand linearregressionshowedthatwaist circumference is related to anthropometric indexes deter-mininglipodystrophy. Somestudiessuggest thatmetabolic changesalsoresultfromcentraladiposity,aswellasinsulin resistance,whichseemstobemorepronouncedinthe pres-enceoflipohypertrophy.31
Atrunktoarmratiomay beagoodparameterforbody fatredistribution,whichshowsupperlimbtaperingand accu-mulationoffatintheabdominalareaanddorsalhump.12In
thisstudy,wedemonstrated thepositiveassociationofthis ratiowithlipodystrophy.Thehighertheindexobtainedbythe ratio,thegreatertheamountoffatinthetrunkand reduc-tionthereofintheupperlimbs.Thisindexiseasytoapply, obtainedthroughskinfolds,beingfeasibleinclinicalpractice. Inthestudy population,nochangeswereverifiedinthe percentageoffatinlowerandupperlimbswhencompared tothe groupswithandwithoutlipodystrophy,howeverthe ratiolimbtotrunkobtainedthroughDXA showedastrong correlationwiththisclinicalchange.Inanotherstudycarried outwithchildrenusingHAARTcomparedtoacontrolgroup, changesinbodycompositionobtainedthroughDXAwerealso noted,evenintheabsenceofclinicalsignsoflipodystrophy.7
Therefore, the clinical diagnosis oflipodystrophy seems to beunderestimated. Vigano et al., demonstrated that 31/37 ofpatientsnon-identifiedaslipodystrophicpatientsshowed
changesinbodycomposition,suchasfatreductioninlower limbsandincreaseinvisceraladipositythroughDXA.Only 8/37ofthesepatientswereprovidedwiththesame clinical andimagediagnosisoflipodystrophy.8
Theresultsofthisstudyshowlimitationsasitisacross sectionalstudy,whichonlyconsidersvariablesatthemoment ofdatacollection,inadditiontothelimitedsampleregarding populationseenatthisclinic.Thus,itwouldbeidealtohave acohortstudytobetterassessthemetabolicsideeffects com-paredtochanges inbody composition. Onthe otherhand, thestudyshowsahomogeneoussampleastoage,pubertal stage,severityofthediseaseanduseofantiretroviraldrugs, supportingtheresultsobtained.
AssessmentofbodycompositionthroughDXAhasthe dis-advantageofrequiringcostlytechnology,therefore,theuseof anthropometric measurements,obtainedthroughskinfolds, presentsafeasibleandlow-costalternative.
Thetrunktoarmandlimbtotrunkratios maybeused as indicators of preclinical lipodystrophy. No cutoffswere establishedtosuchvaluesyet,requiringsubsequentstudies; however,continuousmonitoringoftheseratiosmayidentify changesinbodycompositionofthesepatientsearly.
Conflict
of
interest
Allauthorsdeclaretohavenoconflictofinterest.
r
e
f
e
r
e
n
c
e
s
1.BradyMT,OleskeJM,WilliamsPL,etal.,PediatricAIDS ClinicalTrialsGroup219/219CTeam.Declinesinmortality ratesandchangesincausesofdeathinHIV-1-infected childrenduringtheHAARTera.JAcquirImmuneDeficSyndr. 2010;53(1):86–94.
2.MatildaLH,RamosJrAN,HeukelbachJ,HearstN,Brazilian StudyGrouponSurvivalofChildrenwithAIDS.Continuing improvementinsurvivalforchildrenwithacquired immunodeficiencysyndromeinBrazil.PediatrInfectDisJ. 2009;28(10):920–2.
3.Brasil.MinistériodaSaúde.SecretariadeVigilânciaem Saúde.ProgramaNacionaldeDSTeAids.Recomendac¸ões paraTerapiaAntiretroviralemCrianc¸aseAdolescentes InfectadospeloHIV:manualdebolso/MinistériodaSaúde, SecretariadeVigilânciaemSaúde,ProgramaNacionaldeDST eAIDS.–Brasília:MinistériodaSaúde;2009.
4.CarrA,SamarasK,ChrisholmDJ,CooperDA.Pathogenesisof HIV-1proteaseinhibitor-associatedperipherallipodistrophy, hyperlipidemia,andinsulinresistance.Lancet.
1998;351:1881–3.
5.MillerTL.NutritionalaspectsofHIV-infectedchildren receivinghighlyactiveantiretroviraltherapy.AIDS.2003;17 Suppl.1:S130–40.
6.ValenteAM,ReisAF,MachadoDM,SucciRC,ChacraAR. MetabolicalterationsinHIV-associatedlipodytrophy syndrome.ArqBrasEndocrinolMetabol.2005;49(6):871–81. 7.BrambillaP,BricalliD,SalaN,etal.Highlyactive
antiretroviral-treatedHIV-infectedchildrenshowfat distributionchangeseveninabsenceoflipodystrophy.AIDS. 2001;15(18):2415–22.
antiretroviraltherapyinHIV-infectedchildren.JAIDS. 2003;32:482–9.
9. SociedadeBrasileiradePediatria.Avaliac¸ãonutricionalda crianc¸aedoadolescente–ManualdeOrientac¸ão/Sociedade BrasileiradePediatria.DepartamentodeNutrologia.–São Paulo:SociedadeBrasileiradePediatria,Departamentode Nutrologia;2009.p.112.
10.MarshallEA,TannerJM.Growthandphysiological developmentduringadolescence.AnnuRevMed. 1975;19:283–300.
11. CentersforDiseaseControl.Revisedclassificationsystemfor humanimmunodeficiencyvirus(HIV)infectioninchildren lessthan13yearsofage.MMWR.1994;43:1–10.
12.JaquetD,LèvineM,Ortega-RodriguezE,etal.Clinicaland metabolicpresentationofthelipodystrophicsyndrome HIV-infectedchildren.AIDS.2000;14:2123–8.
13.WorldHealthOrganization.TheWHOchildgrowth standards.Growthreference,5–19y.Geneva,Switzerland: WorldHealthOrganization;2007.
14.KwiterovichJrPO.Recognitionandmanagementof dyslipidemiainchildrenandadolescents.JClinEndocrinol Metab.2008;93:4200–9.
15.TresacoB,BuenoG,PinedaI,MorenoLA,GaragorriJM,Bueno M.Homeostaticmodelassessment(HOMA-IR)indexcut-off valuestoidentifythemetabolicsyndromeinchildren.J PhysiolBoichem.2005;61:381–8.
16. HeymsfieldSB,SmithR,AuletM,etal.Appendicularskeletal musclemass:measurementbydual-photonabsorptiometry. AmJClinNutr.1990;52:214–8.
17.ArpadiSM,CuffPA,HorlickM,WangJ,KotlerDP. LipodystrophyinHIV-infectedchildrenisassociatedwith highviralloadandlowCD4+-lymphocytecountand CD4+-lymphocytepercentageatbaselineanduseofprotease inhibitorsandstavudine.JAcquirImmuneDeficSyndr. 2001;27(1):30–4.
18.WernerML,PoneMV,FonsecaVM,ChavesCR.Lipodystrophy syndromeandcardiovascularriskfactorsinchildrenand adolescentsinfectedwithHIV/AIDSreceivinghighlyactive antiretroviraltherapy.JPediatr(RioJ).2010;86:27–32. 19.SánchezTorresAM,MunozMunizR,MaderoR,BorqueC,
García-MiguelMJ,DeJoséGómezMI.Prevalenceoffat redistributionandmetabolicdisordersinhuman immunodeficiencyvirus-infectedchildren.EurJPediatr. 2005;164(5):271–6.
20.RossoR,ParodiA,dAnnunzioG,etal.Evaluationofinsulin resistanceinacohortofHIV-infectedyouth.EurJEndocrinol. 2007;157(5):655–9.
21.Ergun-LongmireB,Lin-SuK,DunnAM,etal.Effectsof proteaseinhibitorsonglucosetolerance,lipidmetabolism, andbodycompositioninchildrenandadolescentsinfected withhumanimmunodeficiencyvirus.EndocrPract. 2006;12(5):514–21.
22.SarniRO,deSouzaFI,BattistiniTR,etal.Lipodystrophyin childrenandadolescentswithacquiredimmunodeficiency syndromeanditsrelationwiththeantiretroviraltherapy employed.JPediatr(RioJ).2009;85(4):329–34.
23. Spinola-CastroAM,Siviero-MiachonAA,daSilvaMT, Guerra-JuniorG.Theuseofgrowthhormonetotreat endocrine-metabolicdisturbancesinacquired immunodeficiencysyndrome(AIDS)patients.ArqBras EndocrinolMetabol.2008;52(5):818–32.
24.PatinRV,PalchettiCZ,OliveiraFLC.Crianc¸aeadolescente comSIDA.In:PalmaD,EscrivãoMAMS,OliveiraFLC,editors. Guiadenutric¸ãoclínicanainfânciaenaadolescência. Barueri:Manole;2009.p.571–82.
25.MoyleGJ,DaarES,GertnerJM,etal.,Serono9037StudyTeam. Growthhormoneimprovesleanbodymass,physical performance,andqualityoflifeinsubjectswith HIV-associatedweightlossorwastingonhighlyactive antiretroviraltherapy.JAcquirImmuneDeficSyndr. 2004;35:367–75.
26. GelatoM,McNurlanM,FreedlandE.Roleofrecombinant humangrowthhormoneinHIV-associatedwastingand cachexia:pathopysiologyandrationalefortreatment.Clin Ther.2007;29:2269–88.
27.ChantryC,ByrdR,EnglundJ,BakerCJ,McKinneyJrRE, PediatricAidsClinicalTrialsGroupProtocol152StudyTeam. Growth,survivalandviralloadinchildhoodHIVinfection. PediatrInfectDisJ.2003;22:1033–9.
28.StanleyTL,GrinspoonSK.GH/GHRHaxisinHIV lipodystrophy.Pituitary.2009;12(2):143–52.
29.ZhaoJ,BraultJJ,SchildA,GoldbergAL.Coordinateactivation ofautophagyandtheproteasomepathwaybyFoxO transcriptionfactor.Autophagy.2008;4(3):378–80.
30.SandriM,SandriC,GilbertA,etal.FoxOtranscriptionfactors inducetheatrophy-relatedubiquitinligaseatrogin-1and causeskeletalmuscleatrophy.Cell.2004;117:
399–412.
31.BeregszàsziM,JaquetD,LévineM,etal.Severeinsulin resistancecontrastingwithmildanthropometricchangesin theadiposetissueofHIV-infectedchildrenwith