1
Pr evalence of Periodontal Disease in the Fresno Hmong Community
By
Mai Zong Her , Student Resear cher
Asian Amer ican Pacific Islander Health Resear ch Gr oup (AAPIHRG) Univer sity of Califor nia, Berkeley
Hmong Studies Jour nal, 15(1): 1-13.
ABSTRACT
Ther e has been no r esear ch conducted in the past or pr esent to examine the dental health of the Hmong population in Califor nia. Having lived and emigr ated fr om the hills of devel-oping countries, such as Laos, Vietnam, and Thailand, w her e ther e ar e a lack of r esour ces and community outr each on basic or al car e, the Hmong population r eceived ver y minimal attention in r egar ds to dental health. The pur pose of this r esear ch paper is to analyze the statistical data collected at a pr ivat e dental clinic r un by a Hmong dentist, Dr . Kao N. Vang, to illustr ate the pr evalence of the per iodontal diseases, gingivitis and per iodontitis. The in-tention of this quantitative r esear ch is to obtain a gener al over view of dental health in the Fr esno Hmong community, as w ell as to explor e how the inter section of vulner abilities, such as Wester n accultur ation, socioeconomic status, and the lack of a for mal education among Hmong people, have contr ibuted to the depr ivation of basic or al car e and affected the over all dental health of the population.
RESEARCH QUESTION
What is the pr evalence of the gum diseases, gingivitis and per iodontitis, among Fr esno Hmong patients betw een the ages of 16–50 at a pr ivate dental pr actice?
INTRODUCTION
Per iodontal Disease: Gingivitis and Per iodontitis
2
not alw ays lead to the advanced for m of per iodontitis. In the cases w her e gingivitis is left untr eated, it has gr eat potential for advancement to the irr ever sible st ages of per iodontitis. The bones that suppor t the teeth become physiologically compromised and the r ecession of the gums cr eates pockets ar ound the teeth, w hich makes them mor e susceptible to futur e infections. As descr ibed on the patient char ts fr om the dental clinic w her e the data w as col-lected, ther e ar e thr ee stages of per iodontitis. “Slight Per iodontitis” is having minor to mod-er ate bone loss and sockets w ith a depth of 3-4mm. “Modmod-er ate Pmod-er iodontitis” is having moder ate to deep pockets, moder ate to sever e bone loss, and socket s w ith a depth of 5-7mm. “Advanced Per iodontitis” is descr ibed as having deep pockets, sever e bone loss, and a depth of 8mm or gr eater . The last stage of per iodontitis is one of the most common causes of tooth loss. This occur s as a r esponse t o the infection of the gum w her e the body’s immune system br eaks dow n the components suppor ting the teeth, w hich ar e the bone and connective tissues. It is impor tant to note that the depth of a pocket does not alw ays pr e-dict the amount of bone loss.
Who ar e the Hmong people and how ar e they a vulner able gr oup?
Hmong r efer s to a w idely and globally disper sed tr ibal minor ity group of Southeast Asian r efugees w ho immigr ated to the United States pr imar ily fr om the hills of Laos. In 1961, the United States gover nment saw the Hmong as effective guer r illas and advanta-geous in defeating the communist r egime in Southeast Asi a; ther efor e, they began r ecr uit-ing Hmong men and boys in Laos to secr etly fight in the Vietnam War (UCLA Inter national Institute). This collabor ation became the debut of a haunting exper ience for the small, mar-ginalized Hmong population in Laos. After the w ar ended in 1975 and the United States tr oops pulled out, the Hmong became the tar get for a massive genocide implemented by the communist r egime in Southeast Asia. “The w ar took a heavy toll with a thir d of the esti-mated 300,000 Hmong dead or injur ed fr om being r ecr uited to fight for the w ar r ing fac-tions, and half of the total Hmong population for cibly displaced in var ious ar eas” (Lee 3). Many Hmong families escaped per secution by seeking r efuge in r emote, mountainous for-ests and fleeing acr oss the Mekong River to Thailand. In exchange for their sur vival, they encounter ed family separ ation and loss, as w ell as having to accept their displacement into r efugee camps as a lifest yle.
3
Refugees and other populations w ith similar exper iences and backgr ounds ar e con-sider ed to be some of the most vulner able gr oups in the United States (Finney, Lamb, Smith 161). A vulner able population is defined as a “gr oup at incr eased r isk for poor physical, psychological, and social health outcomes and inadequate health car e,” w hich is shaped by “political and social mar ginalization and the lack of socioeconomic and societal r esour ces” (Der ose, Escar ce, Lur ie 1258). For instance, dental health is an emphasized concept of health car e in the United States, but the emphasis and pr actice of daily br ushing and flossing may not exist in immigr ant and r efugee communities such as the Hmong. Scholar s ar -gue that immigr ants and r efugees fr om thir d wor ld countr ies, w her e ther e ar e no available dental ser vices, ar e the least likely to utilize the available dent al ser vices (Mar r cus, Maida, Guzman-Becer r a, Belloso, Fidell). Many of the developing countr ies that the Hmong emi-gr ate fr om do not have a stable health car e syst em w her e the public is infor med about dis-ease contr ol and pr eventative measur es, especi ally tow ar ds dental health (Her 3). Fur ther-mor e, the villages in Laos w her e the Hmong people lived ar e in the r ur al ar eas and some-times difficult to r each by car . This cr eates geogr aphical bar r ier s w her e r esidents did not, or ver y minimally, have access to health car e facilities and dentists. The geogr aphical isola-tion suggests that the idea of visiting dentists for check ups is pr obably a for eign idea and an uncommon routine for them. Her states that, “ver y often, this lack of aw ar eness and know ledge is funneled thr ough the pr ocess of migr ation and per sists in the lives of immi-gr ants and r efugees in the United States” today (Her 3).
The immediacy of the migr ation and r esettlement pr ocess for the Hmong often de-posits them into poor communities and into the mar gins of gover nmental public assistance, w hich may have r esulted in low er employment r ates and public assistance pr ogr ams being the cor e of financial suppor t for many Hmong families. This notion categor izes them as de-pendents and often limits their ability to establish financial, social, and health stability. Re-cent r esear cher s Baker , Dang, Ly, and Diaz (2010) theor ize that the Hmong population in the United State face cer tain health car e bar r ier s, such as immunization, due to nativity, so-cio-economic position and the use of tr aditional Hmong healing pr actices. Likew ise, the Of-fice of Global Health Affair s (2004) identified the major r isk factor s affecting the Hmong community as the follow ing: the tr aditional pr actice of health car e, lack of a for mal educa-tion, and low r ates of English liter acy. Only 61% of Hmong r esidents in the United States have r eceived a high school education and higher , 14% have obtained a Bachelor ’s degr ee or higher , and 43% of the Hmong ar e not pr oficient in the English language (Asian Amer i-can Center for Advancing Justice). These per centages ar e among some of the low est w ithin the Asian Amer ican and Pacific Islander population. Among Asian Amer ican ethnic gr oups, the Hmong also cur r ently hold the highest r ank in the categor y of “pover ty r ate” at 26% and they have one of the low est aver age annual incomes at $10,949 (Asian Amer ican Cen-ter for Advancing Justice).
METHODOLOGY
4
fir st-time patients fr om August 2010 to August 2011 w er e selected for the study. The var ia-bles that w er e collected and used for analysis include: age, sex, occupation, insur ance pr o-vider , date of fir st visit, and dental diagnosis. The insur ance pr oo-vider s ar e indicator s for the socioeconomic statuses of the patients, and they ar e used to make compar isons betw een gr oups w ith differ ent socioeconomic statuses. The pur pose of selecting fir st-time patients w as to tr ack them on a one-year time fr ame to see how often they make visits to the dental office and how many of them fall into the categor y of being a “common patient.” The “com-mon patient” var iable is used to deter mine Wester n accultur ation and to see how the r ates of per iodontal disease differ betw een patient s w ho ar e making r egular visits (accultur ated) and those w ho do not (unaccultur ated); this follow s the assumption that someone who is mor e accultur ated pr actices the Wester n nor m of making r egular dental visits. Dr . Vang defines a common patient as one w ho visits ever y six to seven months or tw ice a year for r egular check ups. Patients w ho ar e r equested t o r etur n to the clinic for additional dental w or k do not count tow ar ds common patient status. This allow s us to see and under stand w hether or not accultur ation factor s into the dental health of the Hmong community. The available diagnoses found on the patient char ts include: gingivitis, slight per iodontitis, moder ate per iodontitis, and advanced per iodontitis. In the data and r esults section of this paper , gingivitis is labeled as 1, per iodontitis is labeled as 2, and the 3 stages of per iodonti-tis ar e labeled as A, B, and C; w ith A being slight, B being moder ate, and C as advanced.
DATA AND RESULTS
5
Data Demogr aphicsFigur e 1. Pie Char t of Patient Age Demogr aphics: The pie char t illust r at es t he age de-mogr aphics of t he 100 pat ient s. A major it y of t he pat ient s wer e 20 year s of age and younger .
Figur e 2. Pie Char t of Patient Statuses: The pie char t indicat es t hat most of t he pat ient s wer e st udent s; 42% wer e st udent s; 28% had some sor t of car eer / job; 29% did not list t heir st at us;
1% wer e unemployed.
100
%
Patient Status
100
%
6
Figur e 3. Pie Char t of Patient Insur ance: Out of t he 100 pat ient s, mor e t han half of t hem wer e st r ict ly under Dent i-Cal. 11% of t hem had low-income healt h insur ance, such as Healt hy
Family. 9% wer e uninsur ed.
Figur e 4. Pie Char t of Common Patients: 34% fell int o t he cat egor y of being “common pa-t ienpa-t s.” The dapa-t a illuspa-t r apa-t es how pa-t he major ipa-t y of pa-t hese papa-t ienpa-t s do nopa-t make r egular denpa-t al
vis-it s.
100
%
Patient
Insurance
100%
Common Patient
vs. Uncommon
7
Per centages of Gingivitis and Per iodontitis
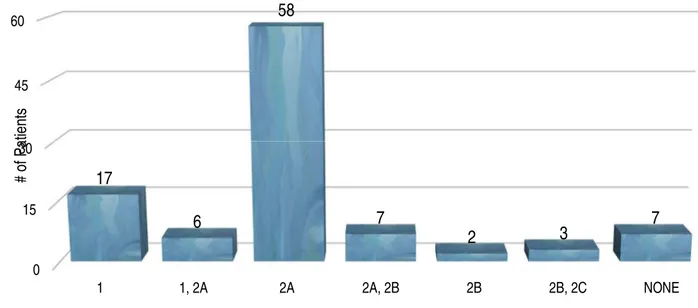
Figur e 5. Bar Gr aph compar ing Over all Per centages of Gingivitis and Per iodontitis: 1=Gin-givit is; 2=Per iodont it is, A=Slight , B=Moder at e, C=Advanced. Out of the 100 patients, 93 of them w er e diagnosed w ith some form of per iodontal disease. 76 of them have per
iodonti-tis.
0 15 30 45 60
1 1, 2A 2A 2A, 2B 2B 2B, 2C NONE
17
6
58
7
2
3
7
#
of
P
at
ient
s
8
Figur e 6. Bar Gr aph of Gingivitis/ Per iodontitis Rates, Males vs. Females: 1=Gingivit is; 2=Per iodont it is, A=Slight , B=Moder at e, C=Advanced. Alt hough mor e females appear ed t o have
higher r at es of gingivit is, t he advanced st ages of per iodont al disease wer e mor e pr evalent in men.
Figur e 7. Bar Gr aph of Gingivitis/ Per iodontitis Rate, Common Patients vs. Uncommon Pa-tients: 1=Gingivit is; 2=Per iodont it is, A=Slight , B=Moder at e, C=Advanced. The moder at e t o se-ver e per iodont it is diagnoses on t he gr aph wer e all among uncommon pat ient s.
0 8 15 23 30
1 1, 2A 2A 2A, 2B 2B 2B, 2C NONE
#
o
f
Pa
ti
e
n
ts
Gingivitis/Periodontitis Rates:
Males vs. Females
Female Male
0 10 20 30 40
1 1, 2A 2A 2A, 2B 2B 2B, 2C NONE
#
o
f
Pa
ti
e
n
ts
Gingivitis/Periodontitis Rates:
Common Patients vs. Uncommon Patients
9
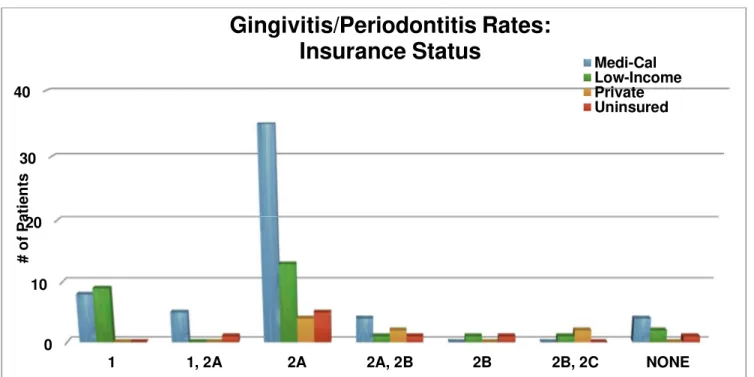
Figur e 8. Bar Gr aph of Gingivitis/ Per iodontitis Rates, Insur ance Statuses: 1=Gingivit is; 2=Per iodont it is, A=Slight , B=Moder at e, C=Advanced. Of t he 93 pat ient s who eit her have
gingi-vit is or per iodont it is, 52 of t hem ar e Dent i-Cal pat ient s.
DISCUSSION
It is cr ucial to under stand the r elationship of dental health to an individual’s over all health. Because the or al cavity is the main entr y for digestion and r espir ation, it is mor e pr one to bacter ial infections. Manifestations of or al diseases can be indicator s to other clin-ical diseases. For example, “r ecent r esear ch suggests that inflammation associated w ith per iodontitis may incr ease the r isk of hear t disease and str oke, pr ematur e bir ths in some w omen, difficulty in contr olling blood sugar in people w ith diabetes, and r espir ator y infec-tion in susceptible individuals” (Wisconsin – Depar tment of Health Ser vices). The Depar t-ment of Health Ser vices in Wisconsin finds that adults w ho have lost their teeth due to per i-odontal diseases have higher r ates of diabetes and angina/ coronar y hear t disease; 65% of those adults have diabetes and 72% have angina/ cor onar y hear t disease. This r esear ch ser ves as evidence that per iodontal disease i s not just a condition and pr oblem w ithin the or al cavity but can be associated w ith other ailing par ts of the human body. This study show s the impor tance in establishing aw ar eness and impr oving the dental health and den-tal hygiene of under -r esour ced ethnic minor ity communities including Hmong Amer icans.
The Center for Disease Contr ol and Pr evention (2013) r eleased a compr ehensive sur vey estimating the r ate of per iodontitis in the United States to be 47.2%. The data show that almost half the U.S. population have per iodontal disease, but the r ates incr ease w ith the condition of having a low er socioeconomic status and a low er level of education attain-ment. The pr evalence of per iodontitis in communities living under the pover ty level is a significant per centage of 65.4% and w ith groups that have obtained less than a high school
0 10 20 30 40
1 1, 2A 2A 2A, 2B 2B 2B, 2C NONE
#
o
f
Pa
ti
e
n
ts
Gingivitis/Periodontitis Rates:
Insurance Status
Medi-Cal10
education, it is 66.9% (Amer ican Academy of Per iodontology). Given that almost half of the people in the United States have per iodontitis and a major ity of the patients fr om the clinic in Fr esno ar e Denti-Cal r ecipients, it is pr esumable that ther e is a high pr evalence of per io-dontal disease in the Hmong community. The data fr om this study illustr ate that 93% of the patients have some for m of per iodontal disease and 76% of them have per iodontitis. When compar ing this data to those of the CDC, it clear ly show s that not only is per iodontal dis-ease ver y pr evalent in the Hmong community, per iodontitis is appr oximately 10% higher w hen compar ed to the data fr om other pover ty-str icken communities and communities w ith low er educational attainment. It is also cr itical to note that out of the 93 patients in the study w ho had per iodontitis, 52 of them w er e Denti-Cal r ecipients, 25 of them had low-income health insur ance, 8 of them w er e uninsur ed, and 8 of them had pr ivate insur ance. It is inter esting that the pr evalence of per iodontal disease is high even among the patients w ho have a higher socioeconomic standing and ar e able to pur chase pr ivate health insur -ance. How ever , pr ivately insur ed patients made up 25% of the patient pool, but they bar ely made up 8% of the patients w ho w er e diagnosed w ith per iodontal disease.
Mor e specific to the r efugee community, a study in 2004 w ith r efugee childr en show s that dental health is often neglected in r efugee childr en; 51.3% of r efugee childr en have dental car ies and 48.7% of them have untreated dental decay (Cote, Geltman, Numm, Litur i, Henshaw , Gar cia 734). Although the data is not dir ectly r elated to per iodontal dis-ease, it pr ovides us w ith an idea of the dental health condition of younger member s of r efu-gee communities like the Hmong. As mentioned in the data and r esults section of this pa-per , 72% of the patients in the study w er e betw een the ages of 16 and 20. This implies that ther e may be a distinct segr egation betw een gener ations, in ter ms of utilizing dental health car e. Never theless, since the younger gener ation do make up a lar ger por tion of the patient pool w hich has a high pr evalence of per iodontal disease, this fur ther suggests that the r ates of per iodontal disease is still ver y high even among Hmong teenager s and young adults. This r aises the question, w hy is the r ate of per iodontal disease still ver y high even among younger patients and w hat kind of bar r ier s ar e contr ibuting to this situation? These ar e questions that r equir e mor e r esear ch and explor ation. The patient demogr aphics show that only 34% of the patients w er e consider ed “common patients” and 66% of them did not make r egular dental check ups at the clinic. This ser ves as an indicator that many Hmong people have not adopted the Wester nized pr actice of making r egular dental visits to check up on their dental health. In addition, the pr evalence of gingivitis and per iodontitis is much higher in uncommon patients than common patients, suggesting that West er n accultur a-tion is a possible factor in the dental health of the Fr esno Hmong community. Similar to the questions that w er e r aised pr eviously, this also r equir es additional r esear ch that involves qualitative analysis.
Conclusion/ Fur ther Resear ch
11
12
Refer ences Cited
Pfeifer , Mar k E. and Br uce Thao, Editor s. “2010 U.S. Census Hmong Population.” Hmong National Development, Inc. 2010. PDF.
“A Community of Contr asts - Asian Amer icans i n the United States: 2011.” Asian Amer ican Center for Advancing Justice. 2011. PDF.
Baker , Dian L., Michelle T. Dang, May Ying Ly, and Rafael Diaz. “Per ception of
Bar r ier s to Immunization Among Par ents of Hmong Or igin in Califor nia.” Amer ican Jour nal of Public Health. 2010. PDF.
Cote, Susan et al. “Dental Car ies of Refugee Chil dr en Compar ed With US Childr en.” Pediat-r ics 114.6 (2004): e733–e740. pediatPediat-r ics.aappublications.oPediat-r g. Web. 29 June 2014.
Der ose, Kathr yn P., Jose J. Escar ce, and Nicole Lur ie. “Immigr ants and Health Car e: Sour ces of Vulner ability.” Healt h Affair s 26, no. 5. September 2007: 1258-1268. PDF.
Finney Lamb, Cathr yn, and Mitchell Smith. “Pr oblems Refugees Face When Accessing Health Ser vices.” New Sout h Wales Public Healt h Bullet in 13. Januar y 2002. PDF.
Her , Mai Zong. “Health Car e Dispar ities in the Immigr ant and Refugee Populations in Cali-for nia: A Closer Look at Popular Health Car e Bar r ier s and the AfCali-for dable Car e Act and Their Effects on Health Car e Accessibility.” Univer sity of Califor nia, Ber keley, June 2014.
Hor ne, Steven B. “Gum Disease: Lear n Causes and Tr eatments for Gingivitis.” MedicineNet. Web. 29 June 2014.
"Hmong: An Endanger ed People." Hmong: An Endanger ed People. UCLA Inter national Institute, 7 July 2004. Web. 28 June 2014.
Lee, Gar y Yia. “Diaspor a and the Pr edicament of Or igins: Inter r ogating Hmong Postcolonial Histor y and Identity.” Hmong Studies Jour nal. PDF.
Mar cus, Maida, Guzman-Becer r a, Belloso and Fidell. “Policy Implications of Access to Dental Car e for Immigr ant Communities.” Califor nia Policy Resear ch Center . 2001. PDF.
Office of Global Health Affair s Humanitar ian and Refugee Health Affair s. “Backgr ound on Potential Health issues for Hmong Refugees fr om Wat Tham Kr abok.” U.S. Depar t-ment of Health and Human Ser vices. 2004. PDF.
13
“Per iodontitis Among Adults Aged
≥
30 Year s — United States, 2009–2010.” Center for Dis-ease Contr ol and Pr evention, November 22, 2013. Web. 29 June 2014.Pinzon-Per ez, Helda. “Health Issues for the Hmong Population in the U.S: Implications for Health Educator s.” Inter national Jour nal of Health Education. 2006. PDF.
Vang, Kao. Per sonal Inter view . August 7, 2012.
About the Author :