REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Morphine
as
first
medication
for
treatment
of
cancer
pain
Beatriz
C.
Nunes,
João
Batista
dos
Santos
Garcia,
Rioko
Kimiko
Sakata
∗UniversidadeFederaldeSãoPaulo,SãoPaulo,SP,Brazil
Received19March2013;accepted10June2013 Availableonline11February2014
KEYWORDS
Cancerpain; Analgesia; Morphine
Abstract
Backgroundandobjectives: the medications used according to the recommendation of the WorldHealth Organizationdo notpromote pain reliefinanumber ofpatients with cancer pain.Theaimofthisstudy wastoevaluatetheuseofmorphineasfirstmedicationforthe treatmentofmoderatecancerpaininpatientswithadvancedand/ormetastaticdisease,asan optiontotherecommendationsoftheWorldHealthOrganizationanalgesicladder.
Method: sixtypatientswithoutopioidtherapy,with≥18yearsofage,wererandomizedintotwo groups.G1patientsreceivedmedicationaccordingtotheanalgesicladderandstarted treat-mentwithnon-opioidsinthefirst,weakopioidsinthesecond,andstrongopioidsinthethird step;G2patientsreceivedmorphineasfirstanalgesicmedication.Theefficacyandtolerability ofinitialuseofmorphinewereevaluatedeverytwoweeksforthreemonths.
Results:thegroupsweresimilarwithrespecttodemographicdata.Therewasnosignificant differencebetweenthegroupsregardingpainintensity,qualityoflife,physicalcapacity, sat-isfactionwithtreatment,needforcomplementationanddoseofmorphine.InG1therewasa higherincidenceofnausea(p=0.0088),drowsiness(p=0.0005),constipation(p=0.0071)and dizziness(p=0.0376)inthesecondvisitanddrowsiness(p=0.05)inthethird.
Conclusions:theuseofmorphineasfirstmedicationforpaintreatmentdidnotpromote bet-teranalgesiceffectthantheladderrecommendedbyWorldHealthOrganization,withhigher incidenceofadverseeffects.
©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
PALAVRAS-CHAVE
Doroncológica; Analgesia; Morfina
Morfinacomoprimeiromedicamentoparatratamentodadordecâncer
Resumo
Justificativaeobjetivos: Osmedicamentosusados segundoarecomendac¸ãodaOrganizac¸ão MundialdeSaúde(OMS)nãopromovemalíviodadordeumaparceladospacientescomdor oncológica.Oobjetivodesteestudofoiavaliarousodemorfinacomoprimeiromedicamento para o tratamentoda doroncológica moderada, em pacientes comdoenc¸a avanc¸ada e/ou metástases,comoopc¸ãoàsrecomendac¸õesdaescadaanalgésicapreconizadapelaOMS.
∗Correspondingauthor.
E-mail:[email protected](R.K.Sakata).
Método: Sessentapacientessemterapiacomopioide,comidade maiorouiguala18 anos, foramdistribuídosaleatoriamenteemdoisgrupos.OspacientesdoG1receberammedicamentos segundo aescadaanalgésicaeiniciaramotratamentocomnão opioidenoprimeiro degrau, opioide fraconosegundo eopioidepotentenoterceiro;osdoG2 receberammorfina como primeiromedicamentoanalgésico.Foramavaliadasaeficáciaeatolerabilidadedousoinicial demorfina,acadaduassemanasdurantetrêsmeses.
Resultados: Osgruposforamsemelhantesquantoaosdadosdemográficos.Nãohouvediferenc¸a significanteentreosgruposquantoàintensidadedador,qualidadedevida,capacidadefísica, satisfac¸ãocomotratamento,necessidadedecomplementac¸ãoedosedemorfinausada.NoG1 houvemaiorincidênciadenáusea(p=0,0088),sonolência(p=0,0005),constipac¸ão(p=0,0071) etontura(p=0,0376)nasegundaconsultaeparasonolência(p=0,05)naterceira.
Conclusões: Ousodemorfinacomoprimeiromedicamento paratratamentodadornão pro-moveumelhorefeitoanalgésicodoqueaescadapreconizadapelaOMSehouvemaiorincidência deefeitosadversos.
©2013SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Theprevalenceofcancerhasincreased,withanestimated projectionfor2020of17millionnewcases.1Thismeansthat
therewillbeanincreaseinindividualswithpaincausedby thediseaseandbytreatment.2
The World Health Organization (WHO) developed the analgesic ladder as a guideline for the treatment of cancerpainandrecommendedtheuseofnonsteroid anti-inflammatorydrugs(NSAIDs)formildpainonthefirst,weak opioidsformoderatepaininthesecond,andpotentopioids for severe painin the third step. Adjuvant drugs may be involvedinallsteps.
In a retrospective study of 1229 patients with can-cer pain, the author reports that the analgesic ladder is effectivein71%.3Manypatients donotgetadequate pain
relief.4,5
Factors relatedtopatients, healthcareinstitutionsand regulatorypoliciesondrugusecontributetothe undertreat-mentofpain.6,7Manypatientswithmoderatetoseverepain
donotreceiveanalgesicsandonly24%ofthosewithsevere painaremedicatedwithapotentopioid.Inonestudy,32% ofpatientsreportedthatthediscomfortwassogreatthat theypreferreddeath.8Despitetheevolutionofknowledge
aboutpain,morethan80%ofpatientswithadvanced can-cer sufferfrompain.9 Inasystematic review,the authors
suggestthat painisundertreatedinapproximatelyhalfof patients.10
Few studies have proposed an alternative to the
WHO ladder11 and suggested that opioids are
pre-scribed inappropriately.12 In areview,the authorssuggest
that the WHO protocol does not use evidence-based
recommendations.13 Some authors criticize the
restric-tion of potent opioids for the third step.14 In a study
of 5084 patients, 56% had moderate to severe pain at leastmonthly.8Betterpaincontrolandpatientsatisfaction
could be obtained withthe use of potent opioidsas first medication.14
Because of these controversies, further studies are needed. The aim of thisstudy wasto determine whether theuseofmorphineinthefirststepoftheWHOladdercan improvetheoutcome.
Method
Model
Prospectiverandomizedstudy.
Participants
Afterapprovalby theEthicsCommitteeandthe informed written consent was obtained, the effectiveness of
mor-phine used in the first step of the WHO ladder was
investigated in patients with locally advanced and/or metastatic cancer. Patients with difficulty in maintaining clinicalfollow-up,cognitiveimpairmentandprevious treat-mentwithopioidswereexcluded.Thestudywasregistered atclinicaltrials.govundernumberNCT01541124.
Randomization,interventionandevaluation
Thepatientsweredividedintotwogroups withtheuseof envelopes containing the number of the patient and the grouptowhichhe(she)belonged. Patientswereincluded inthesequencebyallotmentinthevisit.G1patientswere treatedaccording tothe guidelinesof the WHO analgesic ladderand startedonthefirst step,withparacetamol1g every six hours (maximum dose 4g/day); in the second step,codeine (30mg) everyfourhours(maximum dose of 360mg/day);and morphine10mgevery fourhoursin the thirdstep.G2patientsreceivedmorphine10mgeveryfour hours.Wheneverindicated,adjuvantdrugswereassociated tothetreatment.
According topain intensity, G1 patients switched drug inobedience totheanalgesic ladderand G2 patientshad adjusted the dose of the analgesic drug. The need for palliativecancertherapy,suchasradiotherapy, chemother-apyorhormonetherapy,wasindicatedbytheoncologist.
Painintensityeverytwoweeksbyusingthevisual ana-loguescale(VAS),qualityoflifeeveryfourweeksthrough thebriefquestionnaireofqualityoflifeoftheWHO,15
Evaluated for inclusion (n: 150)
Excluded (n: 90)
•Not attended to inclusion criteria (n: 90) •Refused to participate (n: 0)
Randomized (n: 60)
Included in G1 (n: 30) Treated (n: 30) Not treated (n: 0) Included in G2 (n: 30)
Treated (n: 30) Not treated (n: 0)
Lost to follow-up (n: 6) Lost to follow-up (n: 1)
Evaluated (n: 24) Evaluated (n: 29)
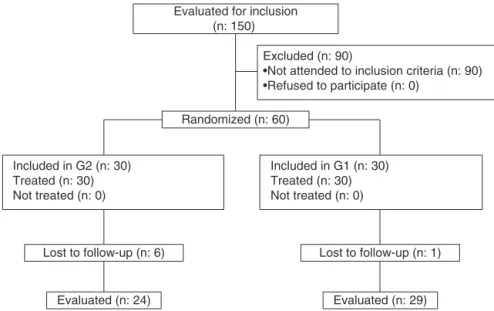
Figure1 CONSORTdiagram.
needforsupplementalanalgesicswereevaluated.Adverse effectswererecorded.Follow-upwasdoneforthreemonths oruntilthedeathofthepatient.
Statistical
analysis
Tocalculatethesamplesize,BioEstat2.0programwasused. Themeanandstandard deviationofanothersimilarstudy wereusedasreference.14Foraconfidencelevelof95%anda
studypowerof80%,30patientspergroup(60intotal)were required.Forthestatistical analysis,GraphPadPrism pro-gramwasused.TheStudentttesttocompareage,weight andheight;chi-squaretestforpatientsatisfaction,needfor complementationandadverse effects;and Mann---Whitney testforpainintensity,qualityoflifeandphysicalfunction wereused.p-Values≤0.05wereconsideredstatistically sig-nificantandtheresultswereexpressedasmean±SD.
Results
Thesequenceofthisstudyisshowninthediagram(Fig.1). 60patientswereincluded,30in eachgroup.Byreasonof death,only24patientsfromG1and29fromG2completed thestudy.The groups weresimilarwithrespectto demo-graphics(sex,age,weightandheight)(Table1).
Themostcommonlocationsoftumorswereinthehead andneck (G1:22, G2:26), withthe sameregion for pain
Table1 Demographicdata(mean± SD).
G1 G2 p
GenderM:F 25:5 27:3 0.7065a
Age(years) 58.7±12.4 57.5±12.7 0.7071b Weight(kg) 59.8±13.8 58.6±13.0 0.7301b Height(cm) 166±0.1 167±0.1 0.7045b
G1,WHOladder;G2,morphineinthe1ststep.
aFisher’test. b Studentttest.
(G1: 21, G2: 26). The most frequent type of pain was somatic(G1: 27,G2: 30).There wasnosignificant differ-encebetweenthegroupswithrespecttothepainduration (G1:4m;G2:3m)andprevioususeofparacetamol(G1:5, G2:2),dipyrone(G1:24,G2:24)NSAIDs(G1,4G2:10), tri-cyclicantidepressants(G1,1G2,1),anxiolytics(G1:1,G2: 0)andnouseofmedication(G1:2,G2:1).
There was no difference in the need for
comple-mentation between groups on the third (G1: 0; G2: 11,
p=0.5057),fourth(G1:5;G2:9,p=0.6696),fifth(G1:10, G2:7,p=0.5970),sixth(G1:3,G2:7,p=0.1966)orseventh (G1:3,G2:5,p=0.3576) visit(Studentttest).Therewas nodifference inpain intensity (Table 2)or quality of life (Table 3). There was no difference in physical capacity on the first (G1: 0.7±0.6, G2: 0.8±0.6, p=0.4430), second(G1:1±0.6,G2:0,9±0,5,p=0.8564),third(G1: 1.1±0.5, G2: 1.1±0.5, p=1.000), fourth (G: 1.2±0, 4, G2:1.1±0.5,p=0.4203),fifth(G1:1.2±0.6,G2:1.1±0.4,
p=0.6234),sixth(G1:1.2±0.6,G2:1.20±0.6,p=0.7197)
Table 2 Pain intensity by visual analogue scale (cm; mean± SD).
Follow-up G1 G2 p
1stvisit 5.8±0.4a 5.8±0.4a 0.5267 2ndweek 4.6±2.3a 4.6±2.6a 0.9579 4thweek 4.9±2.1a 4.2±2.3a 0.2019 6thweek 3.7±2.6b 3.7±1.9b 0.9548 8thweek 2.9±2.6c 3.8±2.5c 0.2307 10thweek 2.5±1.9e 3.4±2.2c 0.1185 12thweek 2.3±2.1f 2.9±2.5d 0.3400
G1,WHOladder;G2,morphineinthe1ststep. Studentttest.
Table3 Qualityoflife.
Follow-up G1 G2 p
1stvisit 92.2± 11.7a 93.0±10.5a 0.7816 4thweek 88.3±11.2a 89.7±13.1a 0.6511 8thweek 88.7±13.2b 92.0±10.4b 0.3003 12thweek 91.1±13.3d 91.0±12.8c 0.9641
G1,WHOladder;G2,morphineinthe1ststep. Studentttest.
a 30. b 28. c 27. d 23.
or seventh (G1: 1.2±0.5, G2: 1.4±0.7, p=0443) visit (Mann---Whitney). Satisfaction with treatment was similar inbothgroups:onthesecond(G1:20,G2:24,p=0.5275), third (G1: 22,G2: 27, p=0.3288), fourth (G1: 22 G2: 28,
p=0.1056),fifth(G1:26,G2:26,p=1),sixth(G1:24,G2:29,
p=1)andseventh(G1:24,G2:28,p=1)visit(chi-square). There was statistically significant difference between groups in the second visit to nausea (G1: 5, G2: 15,
p=0.0088),constipation(G1:14,G2:25,p=0.0071), dizzi-ness(G1,6,G2:14,p=0.0376)anddrowsiness(G1:13,G2: 27,p=0.0005)andtherewasalsoastatisticallysignificant differenceinthethirdvisittodrowsiness(G1:17,G2:25;
p=0.05),alwayswithgreaterfrequencyinG2(chi-square).
Discussion
Inthisstudy,therewasareductioninpainintensityinthe twogroups,whichsuggeststhatthetechniques are effec-tive.Inanotherstudy,patientsreceivingpotentopioidshad betterpaincontrol andgreater satisfactionthanthe con-ventionalgroup,butwithmoreadverseeffects.11
It is possible thatthe combination of paracetamoland morphine resulted in better analgesic effect. In other studies, the combination of potent opioids and non-opioidsresultedin bettercontrolof pain.12,14 However,in
one study half the patients previously treated with the
combination of paracetamol with a potent opioid also obtained pain control without paracetamol;a substantial number of patients discontinued the use of this agent, becauseoftheinconvenienceofswallowingsomany medi-cations,andstillmaintainedcontrolofpain.17,18According
tothesedata,G2patientsdidnotrequireverylargedoses ofmorphineforpainrelief,evenwithoutparacetamol.For patientswithmoderatetosevere painwhopreviouslydid notuseopioids,alowerinitialdoseofmorphine(15mg/day) maybeeffectiveandwelltolerated.19
There wasnoworseningof qualityof life and physical capacityduring the course of this study,but this did not reflectthenegativeimpactofthedisease.Inanotherstudy, although patients receiving potent opioids have obtained betterpaincontrol,thequalityoflifeandphysicalfunction graduallydeteriorated.14
Inthisstudytherewasnodifferenceinpatient satisfac-tion,which is an important form of assessment. Another important point is the incidence of adverse effects. In anotherstudy,patientsreceivingpotentopioidsweremore satisfied,buthadmoreadverseeffects.11Therewasalower
incidenceofnauseainpatientswithconventionaltreatment andinwhomthedosesofopioidswereadjustedaccording totheseverityofpain.14Inthisstudy,ahigherincidenceof
adverseeffectsoccurredwhenmorphinewasthefirstdrug administered,whichisinagreementwiththevalidationof theWHOladder.3However,noimpairmentofqualityoflife
wasobservedinthesecondandthirdvisits,whichsupports theuseofmorphineasafirstdrug.Effectssuchasnausea, vomitingandconstipationcanbemanagedwithprophylactic antiemeticsandlaxatives.Itispossiblethattheincidenceof drowsinessanddizzinesswascomparabletothatobserved withtheWHOladderiftheG2patientshadreceivedlower dosesofmorphine andinassociation withparacetamolor dipyrone.The initialdoseofmorphinein G2wasfixed for allpatients,whichmayhavecontributedtothehigher inci-denceofadverseeffects.Theindividualizationoftheinitial dosebasedontheintensityofpain,withgradualincreases, canreducetheincidenceofadverseeffects.
The motivationfor thisstudy wasthe smallnumberof studiesinvestigatingan option tothe WHOladderfor the
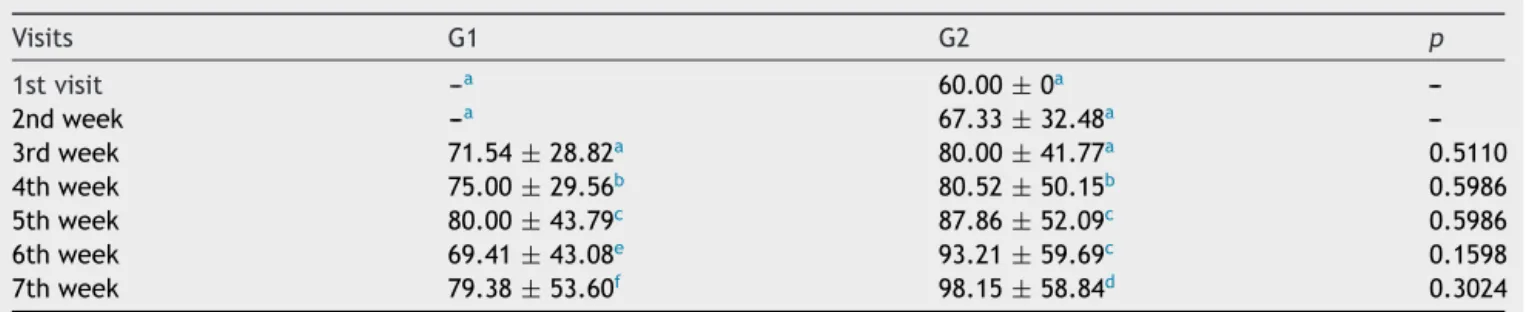
Table4 Morphinedose(mg/day).
Visits G1 G2 p
1stvisit ---a 60.00±0a
---2ndweek ---a 67.33±32.48a
---3rdweek 71.54±28.82a 80.00±41.77a 0.5110
4thweek 75.00±29.56b 80.52±50.15b 0.5986
5thweek 80.00±43.79c 87.86±52.09c 0.5986
6thweek 69.41±43.08e 93.21±59.69c 0.1598
7thweek 79.38±53.60f 98.15±58.84d 0.3024
G1,withladder;G2,withoutladder. Studentttest.
treatmentofcancerpain.About30%ofpatientshave moder-atetoseverepainandonereasonmaybetheinappropriate prescriptionofopioids.12
The sample wasobtained in twoyears and sixmonths becauseofthedifficultyoffindingpatientswhoattendedto theinclusioncriteria.Inasimilarstudy,theauthorsfailedto includethenumberofthecalculatedsample.11 Inanother
study,patientswithmild tomoderatepainwere included andwouldbeexcludedonlyiftheywereusingpotent opi-oids,andthisfacilitatedtheallocation.14Itisbelievedthat
thesamplesizeofthisstudyissufficienttoreflecttheeffect ofthemedicationsaccordingtoWHOandoftheuseof mor-phineasafirstmedication.Thepatients’clinicalconditions makeitdifficulttoimplementtheprotocolinthisgroupwith advancedcancer.
In this study, high incidence of head and neck tumors was diagnosed, unlike other studies,11,14 but all patients
attendedtothe inclusioncriteriabecausethecancer was alreadyinan advancedstage atdiagnosis, withmoderate pain,andneverpreviouslytreatedwithopioids.Inonestudy, twooutofthreepatientswithheadorneckcancerhadpain forsixmonthsbeforediagnosis.20Themostcommonlyused
painkillerbeforethefirstconsultationwasdipyrone,andin anotherstudyanti-inflammatorywerethedrugsmostoften used.11
Itcanbeconcludedthatbothmethodsoftreating pain in advanced cancer patients are comparable, with the differencethat patients receiving morphine asfirst med-ication have more adverse effects on the beginning of treatment.Forselectedpatientswithseverepain,theuse of a potent opioid may be a more appropriate measure. The main limitation of this study is its impossibility of the use of a double-blind design. More studies are rec-ommended to evaluate options for the analgesic ladder (Table4).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.KanavosP.Therisingburdenofcancerinthedevelopingworld. AnnOncol.2006;17:15---23.
2.PaiceJA.Chronictreatment-relatedpainincancersurvivors. Pain.2011;152:S84---9.
3.Ventafridda V, Tamburini M, CaraceniA, et al. A validation study of the WHO method for cancer pain relief. Cancer. 1987;59:850---6.
4.Apolone G, Corli O, Caraceni A, et al. Pattern and quality ofcareofcancerpainmanagement.ResultsfromtheCancer
PainOutcome ResearchStudyGroup.Br JCancer.2009;100: 1566---74.
5.ColsonJ,KoyyalaguntaD,FalcoFJE,etal.Asystematicreview ofobservationalstudiesontheeffectivenessofopioidtherapy forcancerpain.PainPhys.2011;14:E85---102.
6.ReidCM,Gooberman-HillR, Hanks GW.Opioidanalgesicsfor cancerpain:symptomcontrolforthelivingorcomfortforthe dying?Aqualitativestudytoinvestigatethefactorsinfluencing thedecisiontoacceptmorphineforpaincausedbycancer.Ann Oncol.2008;19:44---8.
7.FairchildA.Under-treatmentofcancerpain.CurrOpinSupport PalliatCare.2010;4:11---5.
8.BreivikH,ChernyN, CollettB, etal. Cancer-relatedpain: a pan-European survey of prevalence, treatment, and patient attitudes.AnnOncol.2009;20:1420---33.
9.CostantiniM,RipamontiC,BeccaroM,etal.Prevalence, dis-tress,management,andreliefofpainduringthelast3months ofcancerpatients’life.ResultsofanItalianmortality follow-backsurvey.AnnOncol.2009;20:729---35.
10.DeandreaS, MontanariM, MojaL, ApoloneG. Prevalence of undertreatmentincancerpain.Areviewofpublished litera-ture.AnnOncol.2008;19:1985---91.
11.MaltoniM,ScarpiE,ModonesiC,et al.Avalidationstudyof theWHOanalgesicladder:atwo-stepvsthree-stepstrategy. SupportCareCancer.2005;13:888---94.
12.KlepstadP,KaasaS,ChernyN,etal.Painandpaintreatments inEuropeanpalliativecareunits.Acrosssectionalsurveyfrom theEuropeanAssociationforPalliativeCareResearchNetwork. PalliatMed.2005;19:477---84.
13.FerreiraKASL,KimuraM,TeixeiraMJ.TheWHOanalgesic lad-derforcancerpaincontrol,twenty yearsofuse. Howmuch painreliefdoes one getfrom using it?Support CareCancer. 2006;14:1086---93.
14.MarinangeliF, CiccozziA, Leonardis M, et al. Use of strong opioidsin advancedcancer pain: a randomizedtrial. JPain SymptomManage.2004;27:409---16.
15.Fleck MPA, Louzada S, Xavier M, et al. Aplicac¸ão da versão emportuguêsdoinstrumentoabreviadodeavaliac¸ãoda qual-idadedevida‘‘WHOQOL-brief’’.RevSaúdePública.2000;34: 178---83.
16.MyersJ,GardinerK,HarrisK,etal.Evaluatingcorrelationand interraterreliabilityforfourperformancescalesinthe Pallia-tiveCareSetting.JPainSymptomManage.2010;39:250---8. 17.Dios PD, Lestón JS. Oral cancer pain. Oral Oncol.
2010;46:448---51.
18.AxelssonB,StellbornP,StrömG.Analgesiceffectof paraceta-moloncancerrelatedpaininconcurrentstrongopioidtherapy. Aprospectiveclinicalstudy.ActaOncol.2008;47:891---5. 19.Israel FJ, Parker G, Charles M, et al. Lack of benefit from
paracetamol (acetaminophen) for palliative cancer patients requiringhigh-dosestrongopioids:arandomized,double-blind, placebo-controlled,crossovertrial. JPain SymptomManage. 2010;39:548---54.