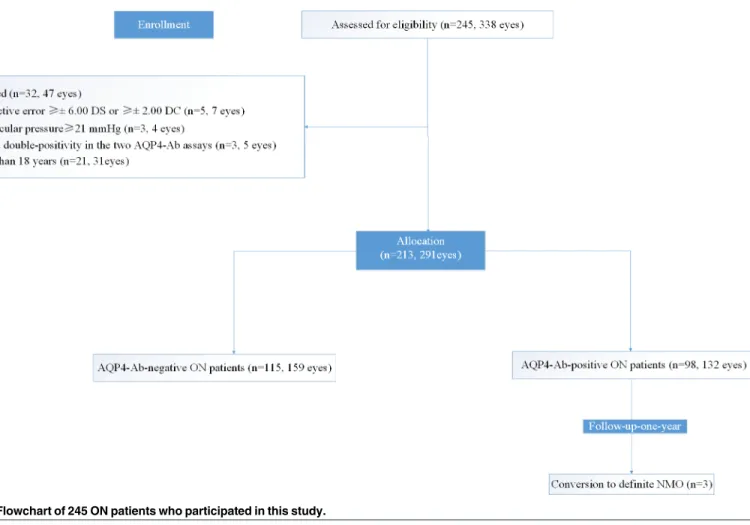
Structural Alterations of Segmented Macular Inner Layers in Aquaporin4-Antibody-Positive Optic Neuritis Patients in a Chinese Population.
Texto
Imagem

Documentos relacionados
Em rios ibéricos, assim como na maioria dos rios temperados, a emergência dos invertebrados mais importantes para a alimentação de peixes, como os Diptera,
After the reconstructed porous medium is generated, the graph of 3-D pore space (skeleton) can be obtained by using a thimiing algorithrn, which
Fuente: elaborado por los autores. Hay variación de velocidad entre los subtítulos es un problema técnico que no fue observado por el subtitulador y que puede tener
Paisagista, CITAB, Apart 1013, 5000-501 Vila Real, [email protected] Resumo Faz-se a indicação das funções que as árvores e os espaços arborizados desempenham no espaço urbano, bem como
têm, como escalão A, se formos aos escalões e começarmos a penalizá-los por…, os pais se calhar começam a interessar-se mais, porque o pai que tem escalão A não tem dinheiro
Diante disto, este trabalho busca analisar a importância do processo de gerenciamento em busca de projetos com resultados mais satisfatórios para todos os envolvidos, sejam eles
Por isso mesmo, escolhemos tal elemento para nossoprQ grama, visto que apesar de sua simplicidade, consegue (com um bom processo de discretização) bons
Comparando os resultados obtidos para Portugal com o Top 10 de cada atributo turístico, verifica-se que Portugal é associado mais frequentemente que a média (dos restantes
