Desorption Ionization-Time of Flight Mass Spectrometry)
for a Rapid Diagnosis of Urinary Tract Infection
Almudena Burillo1,2*, Bele´n Rodrı´guez-Sa´nchez1,4, Ana Ramiro1, Emilia Cercenado1,2,3,4, Marta Rodrı´guez-Cre´ixems1,3,4, Emilio Bouza1,2,3,4
1Department of Clinical Microbiology & Infectious Diseases, Hospital General Universitario Gregorio Maran˜o´n - Instituto de Investigacio´n Sanitaria Gregorio Maran˜o´n, Madrid, Madrid, Spain,2Facultad de Medicina, Universidad Complutense de Madrid (UCM), Madrid, Madrid, Spain,3Red Espan˜ola de Investigacio´n en Patologı´a Infecciosa (REIPI RD06/0008/1025), Sevilla, Sevilla, Spain,4CIBER de Enfermedades Respiratorias (CIBERES CB06/06/0058), Palma de Mallorca, Islas Baleares, Spain
Abstract
Microbiological confirmation of a urinary tract infection (UTI) takes 24–48 h. In the meantime, patients are usually given empirical antibiotics, sometimes inappropriately. We assessed the feasibility of sequentially performing a Gram stain and MALDI-TOF MS mass spectrometry (MS) on urine samples to anticipate clinically useful information. In May-June 2012, we randomly selected 1000 urine samples from patients with suspected UTI. All were Gram stained and those yielding bacteria of a single morphotype were processed for MALDI-TOF MS. Our sequential algorithm was correlated with the standard semiquantitative urine culture result as follows: Match, the information provided was anticipative of culture result; Minor error, the information provided was partially anticipative of culture result; Major error, the information provided was incorrect, potentially leading to inappropriate changes in antimicrobial therapy. A positive culture was obtained in 242/1000 samples. The Gram stain revealed a single morphotype in 207 samples, which were subjected to MALDI-TOF MS. The diagnostic performance of the Gram stain was: sensitivity (Se) 81.3%, specificity (Sp) 93.2%, positive predictive value (PPV) 81.3%, negative predictive value (NPV) 93.2%, positive likelihood ratio (+LR) 11.91, negative likelihood ratio (2LR) 0.20 and accuracy 90.0% while that of MALDI-TOF MS was: Se 79.2%, Sp 73.5,+LR 2.99,2LR 0.28 and accuracy 78.3%. The use of both techniques provided information anticipative of the culture result in 82.7% of cases, information with minor errors in 13.4% and information with major errors in 3.9%. Results were available within 1 h. Our serial algorithm provided information that was consistent or showed minor errors for 96.1% of urine samples from patients with suspected UTI. The clinical impacts of this rapid UTI diagnosis strategy need to be assessed through indicators of adequacy of treatment such as a reduced time to appropriate empirical treatment or earlier withdrawal of unnecessary antibiotics.
Citation:Burillo A, Rodrı´guez-Sa´nchez B, Ramiro A, Cercenado E, Rodrı´guez-Cre´ixems M, et al. (2014) Gram-Stain Plus MALDI-TOF MS (Matrix-Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry) for a Rapid Diagnosis of Urinary Tract Infection. PLoS ONE 9(1): e86915. doi:10.1371/ journal.pone.0086915
Editor:Dongsheng Zhou, Beijing Institute of Microbiology and Epidemiology, China
ReceivedAugust 13, 2013;AcceptedDecember 15, 2013;PublishedJanuary 22, 2014
Copyright:ß2014 Burillo et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding:The authors have no support or funding to report.
Competing Interests:The authors declare that no competing interests exist.
* E-mail: [email protected]
Introduction
Urinary tract infections (UTI) are among the most common infections [1]. Microbiological confirmation of a UTI takes 24– 48 h. In the meantime, patients are usually given empirical antimicrobial therapy, sometimes unnecessarily or inadequately [2]. Anticipation of clinically useful information is of the utmost importance, with both diagnostic and therapeutic consequences [3,4].
Traditionally, a rapid diagnosis of UTI entailed a Gram stain on urine samples [5]. Several studies conducted mostly in the 1970s and 1980s assessed the usefulness of this stain, which proved to be one of the most rapid, reliable and inexpensive methods for anticipating bacteriuria at .105 colony forming units/ml [6]. However, the Gram stain has been abandoned as a routine diagnostic test in most microbiology laboratories.
A new technology, Matrix-Assisted Laser Desorption Ioniza-tion-Time Of Flight Mass Spectrometry (MALDI-TOF MS), has been recently introduced for the analysis of different biomolecules.
This mass spectrometry procedure has been successfully used for the rapid identification of microorganisms already isolated by culture [7,8] but has been scarcely employed for diagnostic purposes directly on clinical samples, with the exception of positive blood cultures, and urine samples [9–15].
In this article, we assess the feasibility of systematically performing a Gram-stain followed by MALDI-TOF MS on urine samples and determine the capacity of this algorithm to anticipate clinically useful information. This algorithm predicted the presence or absence of bacteriuria and the causative pathogen.
Methods
Ethics Statement
Setting
Our institution is a large teaching hospital with 1,550 beds that serves approximately 715,000 of Madrid’s inhabitants. It has an active surgery program including solid organ transplants.
Processing of Urine Samples
During May-June 2012, we randomly selected 1000 urine samples from patients with UTI symptoms (minimal volume of urine submitted was 15 ml). All samples were cultured (2.5ml) on
Cystine Lactose-Electrolyte-Deficient (CLED) agar (bio-Me´rieux, Marcy l’Etoile, France) and incubated in ambient air at 35uC for 18 h. Negative plates were incubated for a further 24 h. The cutoff for a positive culture was $105 colony forming units (cfu) per milliliter of one or two different species [16]. Identification and susceptibility testing were performed by conventional methods (MicroScanß, Siemens, Tarrytown, NY).
Gram Stain
A Gram stain was performed on all uncentrifuged samples and those with bacteria of a single morphotype per 20 oil-immersion fields were processed for MALDI-TOF MS spectrometry.
Gram Stain Interpretation
Agreement between the Gram stain and the culture result was defined as follows.
Full agreement: the Gram stain result was consistent with the bacteria recovered in the culture. Partial agreement: only one of two microorganisms observed was recovered in culture, or viceversa, one of two microorganisms recovered in the culture was not observed. Disagreement: microorganisms observed were not recovered in culture and/or those not observed did appear on the culture plates.
MALDI-TOF Mass Spectrometry
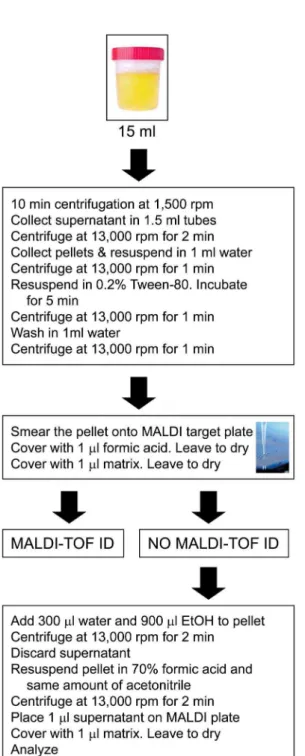
a) Sample preparation. Each 15 ml urine sample was centri-fuged at 1,500 revolutions per minute (rpm) for 10 min to remove leukocytes. The supernatant was collected and aliquoted into 1.5 ml-microcentrifuge tubes and centrifuged at 13,000 rpm for 2 min. Pellets from all tubes were recovered and resuspended in 1 ml high-performance liquid chromatography (HPLC)-quality water (Sigma-Aldrich, St. Gallen Rheintal, Switzerland). After another centrifugation at 13,000 for 1 min, the pellet was incubated in 0.2% Tween-80 (Sigma-Aldrich) for 5 min and centrifuged at 13,000 rpm for 1 min. The pellet was then washed to eliminate the detergent and centrifuged at 13,000 rpm for a further minute.
After discarding the supernatant, the pellet was spotted onto a polished steel MALDI target plate using a 1ml sterile loop and
allowed to dry. Next, it was covered with 1ml of formic acid (70%
vol/vol) and left to dry. Then, 1ml of matrix solution (a -cyano-4-hydroxy-cinnamic acid solution in 50% acetonitrile and 2.5% trifluoroacetic acid) was added prior to the acquisition of spectra in a mass spectrometer.
Samples in which no microorganism identification was possible were further tested after a protein extraction step (see supplemen-tal material). All extracted and non-extracted samples were tested in duplicate to determine the reproducibility of the method. The final score for each sample was the average score of the two spots. The turnaround time was 30 min for the first method and 45 min for the second.
b) MALDI-TOF MS. Measurements were acquired in a Microflex LT bench top mass spectrometer (Bruker Dal-tonics, Germany) using the default settings. According to the manufacturer, a score$2.0 indicated species identification, a score between 1.7 and 2.0 indicated genus identification and a score of,1.7 indicates no identification.
c) MALDI-TOF MS interpretation. The MALDI-TOF MS result was correlated with the culture result as follows:true positive, the MALDI-TOF MS and culture result were consistent; MALDI-TOF MS identified only one microor-ganism when two different microormicroor-ganisms were isolated in the culture; in patients with a recent UTI diagnosis, on antibiotic treatment and with a negative urine culture, MALDI-TOF MS identified a microorganism concordant with the prior positive urine culture;true negative, a negative culture in the absence of MALDI-TOF MS identification;
false positive, MALDI-TOF MS identification differed from the microorganism(s) identified in the cultures; orfalse negative, a positive culture in the absence of MALDI-TOF MS identification.
Sequential Algorithm (Gram Stain Followed by MALDI-TOF MS) Interpretation
Our algorithm was correlated with the culture result, as follows: Match: the information that would be reported to the clinician according to the Gram stain 6 MALDI-TOF MS results was anticipative of the culture result. We defined as a match any of the following situations:
a) No microorganisms detected by Gram staining (and therefore no MALDI-TOF MS was performed) in samples returning a negative culture;
b) Microorganisms detected by Gram staining and MALDI-TOF MS identification matched the microorganism(s) identified in samples;
c) Mixed flora detected by Gram staining (and therefore no MALDI-TOF was performed) in samples returning a contaminated culture.
Minor error: the information that would be reported to the clinician according to the Gram stain6MALDI-TOF MS result was partially anticipative of the culture result. We defined as a minor error any of the following situations:
a) No microorganisms detected by Gram staining (and therefore no MALDI-TOF was performed) in samples returning a contaminated culture;
b) Mixed flora detected by Gram staining (and therefore no MALDI-TOF was performed) in samples returning a negative or positive culture;
c) Microorganisms detected by Gram staining in the absence of MALDI-TOF MS identification in samples returning a negative or a matching positive culture.
Major error: the information that would be reported to the clinician according to the Gram stain6MALDI-TOF MS result was incorrect and would have potentially led to inappropriate changes in antimicrobial therapy. We defined as major error any of the following situations:
b) Microorganisms detected by Gram staining and MALDI-TOF MS identification did not match the culture result.
Statistics
Categorical variables are provided with their frequency distributions. Continuous variables are summarized as medians and inter-quartile ranges (IQR). For the Gram stain, mass spectrometry and sequential algorithm methods, sensitivity, specificity, positive and negative predictive values (PPV and NPV only for the Gram stain), and positive (+LR) and negative (2LR) likelihood ratios, with their 95% confidence intervals, were calculated. Accuracy was defined as the sum of true positive and true negative results. All statistical tests were performed using SPSS ver. 15.0.
Results
Over the study period, 1000 samples from 958 patients were randomly selected for inclusion in the study: 43.2% of these patients were adult men (n = 414), and 3.8% were under 18 years of age (n = 36). Median age was 60.2 years (IQR 41.2–76.3) with no differences between sexes. Distribution by sampling technique was: 91.6% midstream voided, 6.8% bladder catheterization, 1.1% obtained during surgery and 0.6% obtained from patients with a permanent urinary catheter. The origin of the samples was: inpatients, 42.1%; emergency department, 28.8%; outpatient clinics, 25.8%; primary care, 2.6%; unknown, 0.7%.
Of the 1000 samples examined, 242 returned a positive culture. Out of 252 microorganisms isolated, 208 (82.5%) were Gram-negative, 36 (14.3%) were Gram-positive and 8 (3.2%) were yeasts. In only 10 samples (4.1%) were two different microorganisms isolated. The most frequently isolated microorganisms were
Escherichia coli (58.3%), Enterococcus faecalis (8.3%) and Klebsiella pneumoniae(7.9%).
Gram Stain
All 1000 samples were Gram stained. Microorganisms were detected in 267 samples. Gram negative microorganisms were seen in 52.1% of the occasions, Gram positive microorganisms in 20.2%, yeasts in 5.2% and mixed flora in 22.5%. Out of 733 samples in which no microorganisms were detected by Gram staining, 93.2% (n = 683) returned negative cultures.
Full agreement of the Gram stain with the culture result was recorded for 854 or 85.4% of the samples (95% CI 83.2–87.6); partial agreement for 46 or 4.6% (95% CI 3.3–5.9) and disagreement for 100 or 10.0% (95% CI 8.1–11.9). To define the diagnostic performance of the Gram stain, ‘‘partial agree-ments’’ were considered as true positive results. The diagnostic performance of the Gram stain was: Se 81.3% (95% CI 76.4– 86.1), Sp 93.2% (95% CI 91.3–95.1), PPV 81.3% (95% CI 76.4– 86.1), NPV 93.2% (95% CI 91.3–95.1),+LR 11.91 (95% CI 9.06– 15.67),2LR 0.20 (95% CI 0.16–0.26) and accuracy 90.0% (95% CI 88.1–91.9).
MALDI-TOF MS
The 207 samples yielding a single morphotype in the Gram stain were subjected to MALDI-TOF MS. The performance of this test was as follows: correct identification, 130, and only one microorganism identified, 7 (true positives), for a total of 137 (66.2%); no identification in samples with a negative culture (true negative), 25 (12.1%); incorrect identification (false positive), 9 (4.3%); and no identification in samples returning a positive culture (false negative), 36 (17.4%).
The protein extraction protocol was employed every time MALDI-TOF MS failed to offer an identification. That is, it was used on 84 out of 207 samples (40.6%). This procedure allowed to reach a final identification in 20/207 (9.7%) additional samples and gave 3 false positive results. Without extraction, MALDI-TOF’s diagnostic performance was: Se 68.0% (95% CI 60.8– 75.2), Sp 81.3 (95% IC 66.2–96.3),+LR 3.63 (IC95% 1.75–7.51), and 2LR 0.39 (95% CI 0.30–0.52). With extraction, MALDI-TOF’s diagnostic performance was: Se 79.2% (95% CI 72.9– 85.5), Sp 73.5 (95% IC 57.2–89.8),+LR 2.99 (IC95% 1.70–5.27), and 2LR 0.28 (95% CI 0.20–0.40). Thus, without extraction, sensitivity would have been lower.
In our study, out of 1000 urine samples, 10 were found to have 2 different species in cultures; MALDI-TOF MS identified 1 of the 2 isolates in two samples, provided an unreliable identification in one sample and provided no identification in the remaining 7 samples.
In Table 1 we present data on MALDI-TOF MS and conventional identification of monomicrobial cultures in patients with UTI.
False positive MALDI-TOF MS results did not match the Gram stain results. True negative MALDI-TOF MS identifica-tions corresponded to false positive Gram stain results. False negative MALDI-TOF MS results did not correspond to any particular bacterial species.
We did not find any differences in the performance of MALDI-TOF MS with the various types of organisms causing UTI. Nevertheless, this could be due to small sample size.
Sequential Testing Algorithm
The combined performance of the two techniques is shown in Table 2. Overall, our testing algorithm would have provided clinicians with information anticipative of the culture result (82.7%, 95% CI 80.3–85.1) or with minor errors (13.4%, 95% CI 11.2–15.6) for 96.1% of the samples. Only for 3.9% (95% CI 2.7–5.1) of the samples, would the information provided to clinicians have potentially led to changes in antimicrobial therapy that would not benefit the patient.
Of 207 samples in which a single morphotype was detected by Gram staining, MALDI-TOF MS provided an identification in 146 samples and provided no identification in 61 samples. When MALDI-TOF MS provided an identification, this was correct in 93.8% (137/146) of cases, whereas when no identification was given, this negative result was erroneous for 59.0% (36/61) of the samples.
When we examined the spectra recorded in 31/36 positive samples for which no MALDI-TOF MS identification was achieved, three intense peaks were observed, corresponding to the humana-defensins 1, 2 and 3, at a mass to charge ratio of around 3440 Da. The presence of these molecules is known to suppress bacterial protein peaks and therefore prevent database matching [14], acting as a confounder that precludes the etiologic diagnosis of UTI by MALDI-TOF MS performed on urine samples. All our samples containing defensins (n = 31) yielded a positive culture.
detected, in 25/30 of the cases the subsequent cultures were negative.
Turnaround Time
The time needed for these two rapid techniques was signifi-cantly shorter than that required for the more conventional culture methods. For all samples, results were available within one h. We have included in Fig. 1 a flowchart describing the diagnostic procedure.
Discussion
By performing a Gram stain followed by MALDI-TOF MS directly on urine samples we were able to predict the presence or absence of bacteriuria and the causative microorganism in patients with a suspicion of UTI reasonably well and within a working laboratory shift. According to our findings, physicians would receive therapeutically helpful information for 96.1% of samples in less than 1 h. Only in 0.4 out of 10 cases would inappropriate information be provided.
Managing patients with a UTI entails a considerable amount of work for clinicians and microbiology laboratory personnel [17]. The standard quantitative urine culture takes 2–3 days, such that before results are available, clinicians often initiate treatment with antibiotics. These antibiotics are in many cases unnecessary,
inefficient or cover a wider spectrum of microorganisms than necessary [18]. The use of numerous tests to speed up the diagnosis [19–22] has been effectively assessed, but the perfor-mance of these tests (sensitivity/specificity) has been variable at: nitrite (41–64%/85–98%), leukocyte esterase (48–86%/17–93%), white-cell count in urine (67–80%/82–90%). Even when com-bined, false negative results occur in around 10% of patients with a UTI. Moreover, they do not assess the etiology of UTI and cannot replace urine cultures.
The usefulness of Gram staining uncentrifuged urine to identify significant bacteriuria was first demonstrated in 1968 [23] and this has since been occasionally used as a screening test for UTI [24– 26]. Its reported accuracy for the diagnosis of UTI has been: sensitivity, 82.2–97.9%; specificity, 66.0–95.0%; positive predic-tive value, 31.6–94.3%, and negapredic-tive predicpredic-tive value, 95.2– 99.5%, varying with the different counts of microorganisms in the sample, amongst other factors [25–28]. When compared to alternative rapid screening tests, the Gram stain has proved to be more accurate [22,26] and less expensive [28] than other rapid screening tests. In addition, the time needed for Gram staining and microscopy examination is relatively short [5].
Some authors propose that only counts$105cfu/ml should be reported, as these are 73.9 times more likely to correlate with a clinically significant UTI than lower counts [29]. With this cutoff for UTI, only 38 positive urine samples were missed.
Table 1.MALDI-TOF MS versus conventional identification of 242 positive monobacterial cultures.
Conventional identification (no. of cases)
Correlation with Gram stain (%)
Correlation with MALDI-TOF MS identification (%)
MALDI-TOF MS score (median, IQR)*
Escherichia coli(144) 84.0 84.2 2.1 (2.0–2.2)
Klebsiella pneumoniae(20) 90.0 75.0 2.2 (2.0–2.3)
Enterococcus faecalis(19) 78.9 60.0 1.9 (1.8–2.1)
Pseudomonas aeruginosa(9) 77.7 60.0 2.1 (1.8–2.2)
Proteus mirabilis(7) 85.7 80.0 2.2 (2.1–2.2)
Candida albicans(6) 66.7 – –
Staphylococcus aureus(5) 80.0 75.0 1.8 (1.7–2.3)
Enterobacter cloacae(4) 75.0 100.0 2.0 (1.8–2.2)
Candida glabrata(3) 100.0 100.0 1.7 (1.7–1.8)
Klebsiella oxytoca(3) 66.7 50.0 2.4
Acinetobacter baumanii(2) 100.0 100.0 1.8 (1.8–1.9)
Enterococcus faecium(2) 50.0 – –
Lactobacillusspp. (2) 100.0 100.0 1.9 (1.8–1.9)
Morganella morganii(2) 100.0 100.0 2.0 (1.7–2.4)
Staphylococcus epidermidis(2) 100.0 100.0 1.8 (1.7–2.0)
Streptococcus agalactiae(2) 50.0 100.0 1.7
Streptococcus gallolyticus(2) 50.0 100.0 1.7
Candida krusei(1) 100.0 – –
Candida tropicalis(1) 100.0 – –
Enterobacter sakazakii(1) 100.0 100.0 1.9
Gardnerella vaginalis(1) 100.0 100.0 1.7
Providencia stuartii(1) 100.0 – –
Pseudomonas putida(1) – Not performed –
Serratia marcescens(1) – Not performed –
Streptococcus viridans(1) – Not performed –
The clinical impacts of rapidly reporting Gram stain informa-tion on urine samples submitted for culture have not been sufficiently addressed and only one previous study including 57 samples has examined this issue to date [30].
The general consensus is that MALDI-TOF MS is a fast, reliable and cost-effective technique that is easily implemented [7,8]. However, only a few studies have explored its use directly on organic fluids, before microbial isolation [31,32]. Limited data related to the direct use of MALDI-TOF MS on urine samples are available [12–15]. One of the difficulties of this technique arises from insufficient numbers of bacteria in the sample; the threshold of microorganisms required varies among the different species [12,15,33,34]. Thus, samples need to be preselected depending on their bacterial load [15]. We believe that the best way to do this is by Gram staining, which will also indicate the type of responsible microorganism.
Some authors have warned of the need to improve the sensitivity of this technology, although they admitted that the majority of urine samples collected from patients with common urinary tract infections have bacterial counts .105cfu/ml and can therefore be identified by MALDI-TOF MS [15].
UTI with counts under 105cfu/ml do, of course, exist. Present rapid screening tests (Gram stain, dipstick urine analysis or flow cytometry) are not sensitive enough for samples with bacterial counts under this threshold [35]. However, they have a high negative predictive value and this is why these screening methods should continued to be used to rule out bacteriuria and avoid plating negative urine samples, as are the majority of samples. The high costs and labor requirements of culture can only be controlled by effective utilization of this test [35,36].
In patients with upper or complicated UTI, if there is no clinical improvement within 48 hours of starting antibiotic treatment, in
the case of recurrent UTI, or if there are any other complicating factors, then no pre-screening should be done and these urine samples should all be cultured, giving value to counts$102–3cfu/ ml.
There is some concern regarding the performance of MALDI-TOF MS directly on clinical samples testing positive for specific microorganisms. It is well known that yeast identification at the species level achievable by MALDI-TOF MS in positive blood cultures, even after protein extraction, is poor [9,37]. The same can be said for certain streptococci [38]. This poor performance was also observed in our study. The scores obtained for urine cultures containingCandida glabratausing our diagnostic algorithm only support an identification at the genus level, which is not more informative for the clinician than the Gram stain. The same applied to urine cultures positive for certain Gram positive microorganisms such as Streptococcus agalactiae and Streptococcus gallolyticus. Still, for the Bruker MALDI Biotyper system, lowering the species-secure score cutoff to.1.7 instead of the manufactur-er’s recommendation of$2.0 is now deemed acceptable by some authors [39,40].
Regarding mixed urine cultures, in a recent study by Wang et al., the MALDI-TOF MS detection of 2 microorganisms present in urine specimens was tested by spiking sterile saline aliquots with 2 different bacterial species at different dilutions. The authors observed that the two types of bacterium could be identified in a mixture only if they appeared at ratios of 1:1 or 1:2 [15]. In their study, 2 different species were recovered from cultures in 44 urine samples (out of 1456 clinical samples). In 4 of these samples, 2 types of bacterium were identified by MALDI-TOF MS. In 20 samples, only 1 of the 2 isolates was identified and in the remaining 20 samples, MALDI-TOF MS provided an unreliable identification. Our experience was similar. These two
Table 2.Results of the sequential testing algorithm (Gram followed by MALDI-TOF MS).
Gram stain MALDI-TOF MS Culture result Match n (%) Minor error n (%) Major error n (%)
No m.o. (n = 733) Not performed Negative 683 (68.3) – –
Contaminated – 12 (1.2) –
Positive – – 38 (3.8)
M.o.* seen (n = 207) Correct identification Negative** 1 (0.1) – –
Contaminated*** 7 (0.7) – –
Positive 129 (12.9) – –
Incorrect identification Negative{
– 7 (0.7) –
Contaminated – 1 (0.1) –
Positive – – 1 (0.1)
No identification Negative – 25 (2.5) –
Positive{{
– 36 (3.6) –
Mixed flora (n = 60)
Not performed Negative – 15 (1.5) –
Contaminated 7 (0.7) – –
Positive – 38 (3.8) –
Total (n = 1000) 827 (82.7) 134 (13.4) 39 (3.9)
*M.o.: microorganisms.
**Patient with a recent UTI diagnosis on antibiotic treatment. The UTI was caused by thesameorganism identified with MALDI-TOF MS, according to the prior positive urine culture.
***One microorganism identified by MALDI-TOF MS.
{Patients with a recent UTI diagnosis on antibiotic treatment. The UTI was caused by adifferentorganism than that identified with MALDI-TOF MS, according to the prior positive urine culture.
{{
In 31/36 samples,a-defensins suppressed bacterial peaks rendering no identification with MALDI-TOF MS.
examples indicate that this technology is not yet adequate for the identification of different bacterial strains directly on clinical samples. Still, as confirmed in our study, most UTI (over 90%) are monomicrobial [27,41,42].
In a study by Ko¨hling et al., 107 urine samples from patients with clinical suspicion of UTI that were not preselecteda priorifor high bacterial counts revealed an overall sensitivity of the
MALDI-TOF MS method of 60.7% [14]. These authors reported an interesting phenomenon. Thus, when they analyzed the spectra yielded by 22/26 positive samples for which no identification was achieved, they found a triplet of intense peaks corresponding to humana-defensins 1, 2 and 3, located at a mass to charge ratio of around 3440 Da. The presence ofa-defensins suppressed bacterial peaks and prevented database matching such that microorganisms could not be identified directly in the urine samples. We also observed this phenomenon in our work. When the authors tested samples without defensins, the sensitivity of the MALDI-TOF MS procedure used directly on urine samples was 97.1% for counts $105cfu/ml.
In our study, after reviewing the medical records of the patients with humana-defensins, we could not find any common clinical feature among them with regard to type of patient, underlying disease, clinical presentation or outcome.
The potential clinical impacts of being able to identify the causative pathogen of any infection is directly related to how much knowing the taxon would serve to direct empiric antibiotic therapy [3]. To assess this, it is also desirable to know the local epidemiology (community –preferable– or hospital surveillance data) and associated resistance patterns in each setting [43]. MALDI-TOF MS has already proved its usefulness in reducing the time to effective and optimal antibiotic treatment in both bacteremia and candidemia [11,44,45]. In effect, the value of microbiologic data is often inversely proportional to the time interval necessary for its generation [3].
Our serial diagnostic algorithm Gram stain plus MALDI-TOF MS was able to provide in under an hour an etiologic diagnosis of UTI. This diagnosis allows for the adjustment of empiric antibiotic treatment, especially when the causative microorganism are not those most frequently associated with this type of infection (i.e., non-fermenting Gram-negative bacilli, yeasts) or when they have resistance mechanisms (i.e., AmpC betalactamase-producing
Enterobacteriaceae,Staphylococcus aureus).
As a limitation of our study, we should mention that being a single-center study, its results may only reflect local practice patterns. However, we included 1000 urine samples from all types of patients and did not preselect any subgroup with greater clinical suspicion of UTI. A disadvantage of the method proposed is that it requires a minimum sample volume of 15 ml of urine.
Future studies should address the clinical impacts of our rapid diagnosis algorithm for UTI by examining its capacity to improve the adequacy of treatment in terms of reducing the time of empiric antibiotic treatment or allowing for the earlier withdrawal of unnecessary antibiotics.
Acknowledgments
The authors thank Ana Burton for editorial assistance and Dr. Cristina Ferna´ndez for help with the statistical analysis of the data.
Author Contributions
Conceived and designed the experiments: EB AB. Performed the experiments: AB BR-S AR EC. Analyzed the data: EB AB. Contributed reagents/materials/analysis tools: AB EC MR-C. Wrote the paper: AB BR-S AR EC MR-C EB.
References
1. Foxman B (2010) The epidemiology of urinary tract infection. Nat Rev Urol 7: 653–660.
2. McIsaac WJ, Hunchak CL (2011) Overestimation error and unnecessary antibiotic prescriptions for acute cystitis in adult women. Med Decis Making 31: 405–411.
3. Staneck JL (1985) Screening tests and ‘‘rapid’’ identification. Is anybody out there listening? Diagn Microbiol Infect Dis 3: 51S–57S.
4. Foxman B, Brown P (2003) Epidemiology of urinary tract infections: transmission and risk factors, incidence, and costs. Infect Dis Clin North Am 17: 227–241.
5. Lewis JF, Alexander J (1976) Microscopy of stained urine smears to determine the need for quantitative culture. J Clin Microbiol 4: 372–374.
6. Clarridge JE, Johnson JR, Pezzlo MT (1998) Cumitech 2B, Laboratory diagnosis of urinary tract infections; Welssfeld AS, editor. Washington, D. C.: American Society for Microbiology. 21 p.
7. Ho YP, Reddy PM (2011) Advances in mass spectrometry for the identification of pathogens. Mass Spectrom Rev 30: 1203–1224.
8. Cherkaoui A, Hibbs J, Emonet S, Tangomo M, Girard M, et al. (2010) Comparison of two matrix-assisted laser desorption ionization-time of flight mass spectrometry methods with conventional phenotypic identification for routine identification of bacteria to the species level. J Clin Microbiol 48: 1169–1175. 9. La Scola B, Raoult D (2009) Direct identification of bacteria in positive blood
culture bottles by matrix-assisted laser desorption ionisation time-of-flight mass spectrometry. PloS One 4: e8041.
10. Ferroni A, Suarez S, Beretti JL, Dauphin B, Bille E, et al. (2010) Real-time identification of bacteria andCandidaspecies in positive blood culture broths by matrix-assisted laser desorption ionization-time of flight mass spectrometry. J Clin Microbiol 48: 1542–1548.
11. Vlek AL, Bonten MJ, Boel CH (2012) Direct matrix-assisted laser desorption ionization time-of-flight mass spectrometry improves appropriateness of antibiotic treatment of bacteremia. PloS One 7: e32589.
12. Ferreira L, Sanchez-Juanes F, Gonzalez-Avila M, Cembrero-Fucinos D, Herrero-Hernandez A, et al. (2010) Direct identification of urinary tract pathogens from urine samples by matrix-assisted laser desorption ionization-time of flight mass spectrometry. J Clin Microbiol 48: 2110–2115.
13. Ferreira L, Sanchez-Juanes F, Munoz-Bellido JL, Gonzalez-Buitrago JM (2011) Rapid method for direct identification of bacteria in urine and blood culture samples by matrix-assisted laser desorption ionization time-of-flight mass spectrometry: intact cell vs. extraction method. Clin Microbiol Infect 17: 1007–1012.
14. Kohling HL, Bittner A, Muller KD, Buer J, Becker M, et al. (2012) Direct identification of bacteria in urine samples by matrix-assisted laser desorption/ ionization time-of-flight mass spectrometry and relevance of defensins as interfering factors. J Med Microbiol 61: 339–344.
15. Wang XH, Zhang G, Fan YY, Yang X, Sui WJ, et al. (2013) Direct identification of bacteria causing urinary tract infections by combining matrix-assisted laser desorption ionization-time of flight mass spectrometry with UF-1000i urine flow cytometry. J Microbiol Methods 92: 231–235.
16. Pezzlo M, York MK, Church DL (2010) Urine cultures. In: Garcia LS, editor. Clinical Procedures Handbook. 3rd ed. Washington, D. C.: ASM Press. 3.12.11-13.12.31.
17. Bouza E, San Juan R, Munoz P, Voss A, Kluytmans J (2001) A European perspective on nosocomial urinary tract infections I. Report on the microbiology workload, etiology and antimicrobial susceptibility (ESGNI-003 study). Europe-an Study Group on Nosocomial Infections. Clin Microbiol Infect 7: 523–531. 18. Sundqvist M, Kahlmeter G (2009) ‘Pre-emptive culturing’ will improve the
chance of ‘getting it right’ when empirical therapy of urinary tract infections fails. J Antimicrob Chemother 64: 227–228.
19. Deville WL, Yzermans JC, van Duijn NP, Bezemer PD, van der Windt DA, et al. (2004) The urine dipstick test useful to rule out infections. A meta-analysis of the accuracy. BMC Urol 4: 4.
20. Wilson ML, Gaido L (2004) Laboratory diagnosis of urinary tract infections in adult patients. Clin Infect Dis 38: 1150–1158.
21. St John A, Boyd JC, Lowes AJ, Price CP (2006) The use of urinary dipstick tests to exclude urinary tract infection: a systematic review of the literature. Am J Clin Pathol 126: 428–436.
22. Williams GJ, Macaskill P, Chan SF, Turner RM, Hodson E, et al. (2010) Absolute and relative accuracy of rapid urine tests for urinary tract infection in children: a meta-analysis. Lancet Infect Dis10: 240–250.
23. Goulden BE (1968) Assessment of the usefulness of the examination of a gram smear of fresh uncentrifuged urine in the determination of significant bacteriuria in dogs. N Z Vet J 16: 1–2.
24. Jorgensen JH, Jones PM (1975) Comparative evaluation of theLimulusassay and the direct Gram stain for detection of significant bacteriuria. Am J Clin Pathol 63: 142–148.
25. Robins DG, Rogers KB, White RH, Osman MS (1975) Urine microscopy as an aid to detection of bacteriuria. Lancet 1: 476–478.
26. Crout FV, Tilton RC (1984) Rapid screening of urine for significant bacteriuria by Gram stain, acridine orange stain, and the Autobac MTS system. Diagn Microbiol Infect Dis 2: 179–186.
27. Tilton RE, Tilton RC (1980) Automated direct antimicrobial susceptibility testing of microscopically screened urine cultures. J Clin Microbiol 11: 157–161. 28. Wiwanitkit V, Udomsantisuk N, Boonchalermvichian C (2005) Diagnostic value and cost utility analysis for urine Gram stain and urine microscopic examination as screening tests for urinary tract infection. Urol Res 33: 220–222. 29. Kwon JH, Fausone MK, Du H, Robicsek A, Peterson LR (2012) Impact of
laboratory-reported urine culture colony counts on the diagnosis and treatment of urinary tract infection for hospitalized patients. Am J Clin Pathol 137: 778– 784.
30. Kuijper EJ, van der Meer J, de Jong MD, Speelman P, Dankert J (2003) Usefulness of Gram stain for diagnosis of lower respiratory tract infection or urinary tract infection and as an aid in guiding treatment. Eur J Clin Microbiol Infect Dis 22: 228–234.
31. Spanu T, Posteraro B, Fiori B, D’Inzeo T, Campoli S, et al. (2012) Direct maldi-tof mass spectrometry assay of blood culture broths for rapid identification of
Candidaspecies causing bloodstream infections: an observational study in two large microbiology laboratories. J Clin Microbiol 50: 176–179.
32. Rodrı´guez-Sa´nchez B, Sa´nchez-Carrillo C, Ruiz A, Rodrı´guez-Cre´ixems M, Bouza E (2012) Rapid identification of pathogens by MALDI-TOF MS in blood culture bottles. In: American Society of Microbiology, editor. Interscience Conference on Antimicrobial Agents and Chemotherapy. San Francisco, 9–12 September, 2012. pp. D-726.
33. Bjørnholt JV, Nilsen SM, Noorland I, Wigemyr M, Løken CH, et al. (2011) MALDI-TOF mass spectrometry ID of bacteria directly from cerebrospinal fluid: what you see is what you get. Clin Microbiol Infect 17: S66.
34. Christner M, Rohde H, Wolters M, Sobottka I, Wegscheider K, et al. (2010) Rapid identification of bacteria from positive blood culture bottles by use of matrix-assisted laser desorption-ionization time of flight mass spectrometry fingerprinting. J Clin Microbiol 48: 1584–1591.
35. Kulkarni S, Nigrin J (2013) Letter to the Editor re: ‘‘Performance of flow cytometry to screen urine for bacteria and white blood cells prior to urine culture’’. Clin Biochem. doi: 10.1016/j.clinbiochem.2013.09.010.
36. Hartley S, Valley S, Kuhn L, Washer LL, Gandhi T, et al. (2013) Inappropriate testing for urinary tract infection in hospitalized patients: an opportunity for improvement. Infect Control Hosp Epidemiol 34: 1204–1207.
37. Rodriguez-Sanchez B, Sanchez-Carrillo C, Ruiz A, Marin M, Cercenado E, et al. (2013) Direct identification of pathogens from positive blood cultures using matrix-assisted laser desorption/ionization time-of-flight (MALDI-TOF) mass spectrometry. Clin Microbiol Infect. Epub ahead of print.
38. Loonen AJ, Jansz AR, Stalpers J, Wolffs PF, van den Brule AJ (2012) An evaluation of three processing methods and the effect of reduced culture times for faster direct identification of pathogens from BacT/ALERT blood cultures by MALDI-TOF MS. Eur J Clin Microbiol Infect Dis 31: 1575–1583. 39. Hoyos-Mallecot Y, Miranda-Casas C, Cabrera-Alvargonzalez JJ,
Gomez-Camarasa C, Perez-Ramirez MD, et al. (2013) [Bacterial identification from blood cultures by a rapid Matrix-Assisted Laser Desorption-Ionisation Time-of-Flight mass spectrometry technique]. Enferm Infecc Microbiol Clin 31: 152– 155.
40. Cheng JW, Tang YE, Jureen R, Lin RTP, Teo JWP (2013) Modified protocol for yeast identification using matrix-assisted laser desorption ionization-time of flight mass spectrometry. AJMR American Journal of Microbiological Research. pp. 71–73.
41. Kallenius G, Dornbusch K, Hallander HO, Jakobsson K (1981) Comparison of direct and standardized antibiotic susceptibility testing in bacteriuria. Che-mother 27: 99–105.
42. Bronnestam R (1999) Direct antimicrobial susceptibility testing in bacteriuria. APMIS 107: 437–444.
43. Burd EM, Kehl KS (2011) A critical apparisal of the role of the clinical microbiology laboratory in the diagnosis of urinary tract infections. J Clin Microbiol 49: S34–S38.
44. Clerc O, Prod’hom G, Vogne C, Bizzini A, Calandra T, et al. (2013) Impact of matrix-assisted laser desorption ionization time-of-flight mass spectrometry on the clinical management of patients with Gram-negative bacteremia: a prospective observational study. Clin Infect Dis 56: 1101–1107.