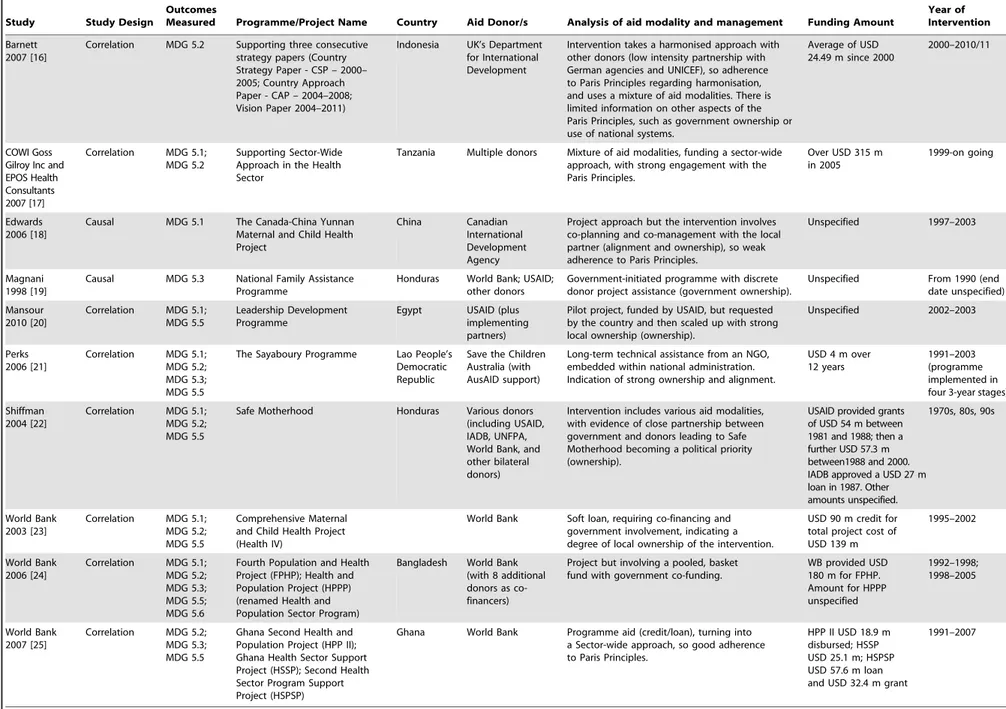
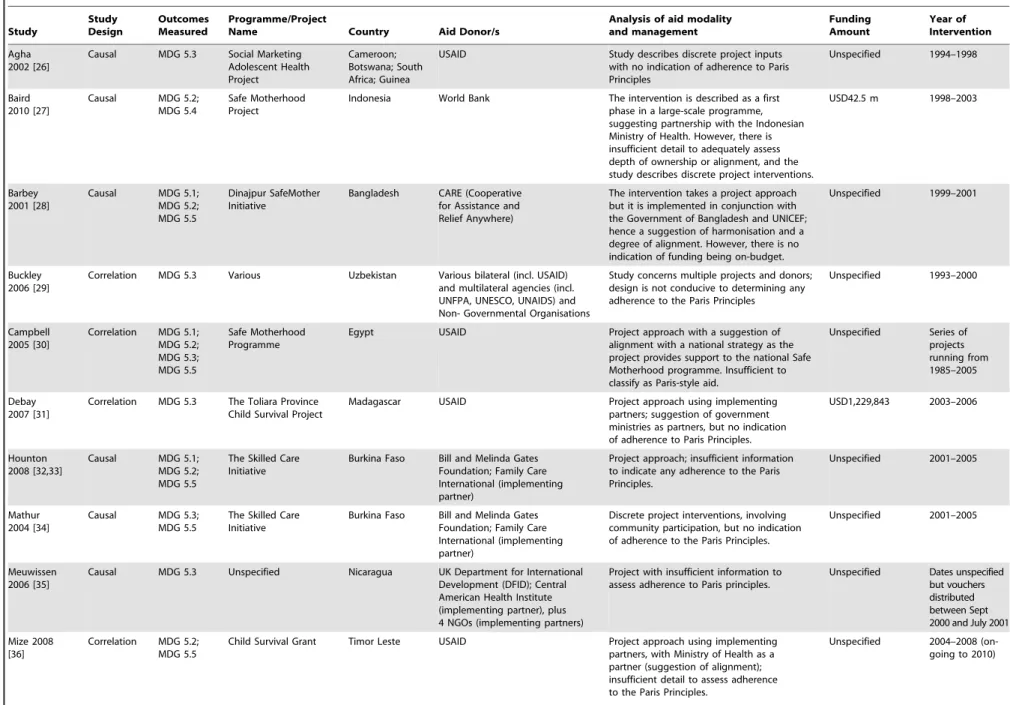
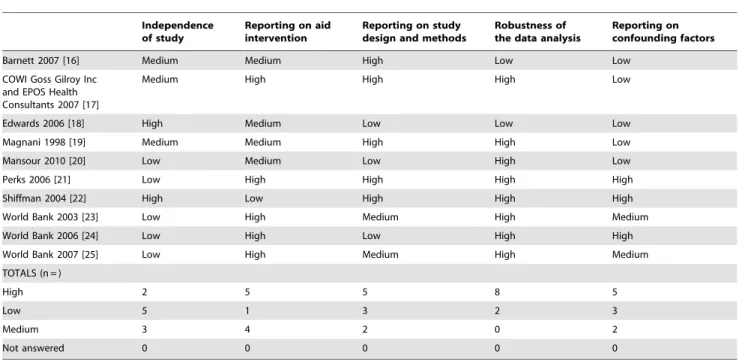
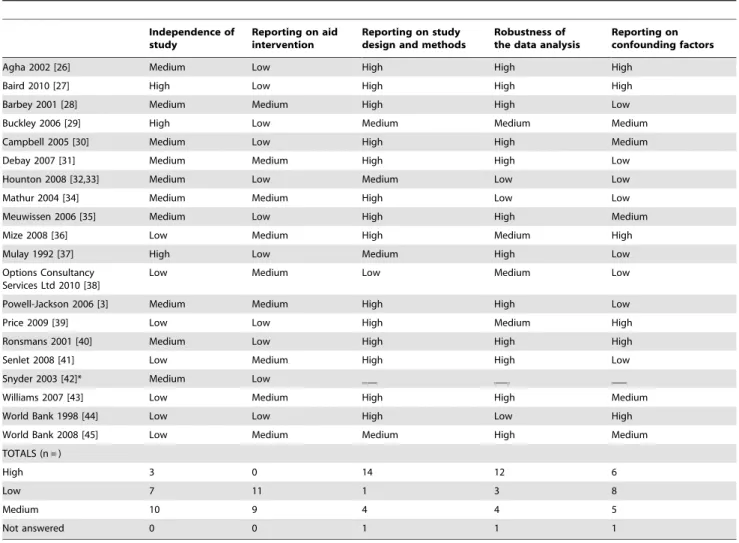
The impact of official development aid on maternal and reproductive health outcomes: a systematic review.
Texto
Imagem
Documentos relacionados
Isso posto, nesse panorama ainda esquecido pelo sistema de inovação nacional, é que se busca por possibilidades de substituição do encarceramento em Unidades Penais de
O presente trabalho teve como objetivo minimizar o sabor amargo da carne escura de atum (Euthynnus pelamis), através da fermentação lática, utilizando Lactobacillus casei subsp...
O objetivo deste artigo é pontuar aspectos teóricos e de método sobre o Grupo Reflexivo de Mediação Biográfica (GRMB), com foco na produção e recepção de
O consultor deverá informar o cliente, no momento do briefing inicial, de quais as empresas onde não pode efetuar pesquisa do candidato (regra do off-limits). Ou seja, perceber
Afinal, se o marido, por qualquer circunstância, não puder assum ir a direção da Família, a lei reconhece à mulher aptidão para ficar com os poderes de chefia, substituição que
Na hepatite B, as enzimas hepáticas têm valores menores tanto para quem toma quanto para os que não tomam café comparados ao vírus C, porém os dados foram estatisticamente
Há evidências de que as isoflavonas agliconas são absorvidas mais rapidamente pelo intestino delgado do que as formas glicosiladas, logo, é importante avaliar não somente
É nesta mudança, abruptamente solicitada e muitas das vezes legislada, que nos vão impondo, neste contexto de sociedades sem emprego; a ordem para a flexibilização como
