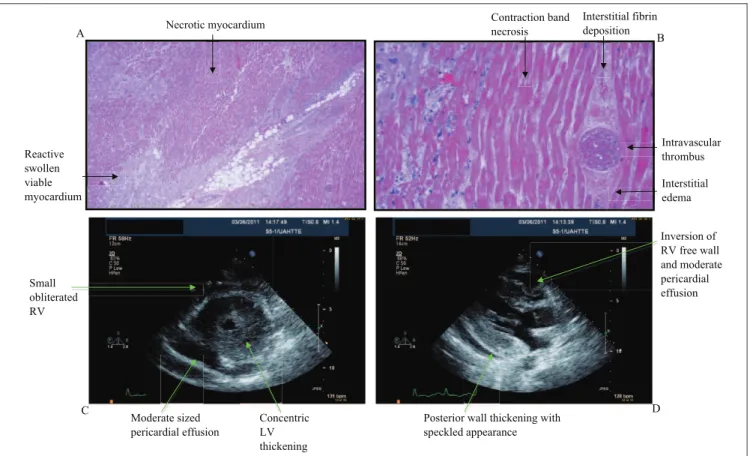
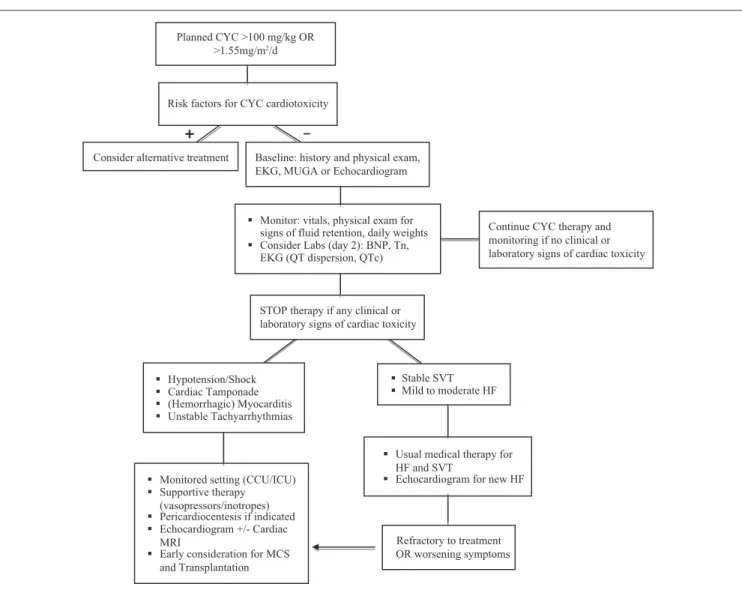
Cyclophosphamide-Induced Cardiomyopathy
Texto
Imagem

Documentos relacionados
ABSTRACT - Although most children with human immunodeficiency virus (HIV) infection have neurological dysfunction, in childhood the incidence of symptomatic cerebrovascular disease
In general, before this period, a diagnosis is only made in patients with the most severe form of the disease with early manifesta- tions of heart failure, or in the presence of
Chronic administration of ghrelin improves left ventricular dysfunction and atten- uates development of cardiac cachexia in rats with heart failure. Papotti M, Ghe C, Cassoni
No que se refere às concepções pessoais de inteligência verificam-se, contudo, resultados ligeiramente diferentes, isto é, tanto na escala es- tática como na escala total, são
cardiac involvement in the neonatal period to incidences as high as 45% to 75% in naive severe patients 29. In patients with left ventricular dysfunction, the mean percentage of
Stress-induced cardiomyopathy, also know as reversible left ventricular apical ballooning, “Broken-Heart” syndrome, and in Japan, Takotsubo, is characterized by the presence of
Cardiac resynchronization therapy; echocardiography/ methods; ventricular dysfunction, left; heart failure... As mentioned in the study, the CMRI considered a reference method
According to current guidelines of chronic heart failure, one must consider the performance of cardiac catheterization in patients with left ventricular dysfunction of unknown
